General Topics

KEY POINTS
- Drowning involves respiratory impairment from submersion/immersion in Drowning outcomes are classified as death, morbidity and no morbidity.
- The pathophysiology of drowning is complex, largely unknown, differing with water temperature and with immersion or submersion.
- Management of respiratory failure for drowning victims requires oxygenation and positive end-expiratory pressure either through noninvasive or invasive ventilation.+
- Short submersion time, quick rescue and rapid administration of rescue breaths are crucial for a good prognosis.
- Rapid cooling of the brain prior to asphyxia is neuroprotective.
INTRODUCTION
Drowning is the third leading cause of unintentional injury death worldwide, affecting approximately 236 000 victims per year. This is despite a reduction in unintentional drowning rates of 44.5% between 1990 and 2017.1 Overall drowning figures should also include intentional, transport–related and natural disaster–related drowning, making the global burden of drowning much larger. Considering these numbers, prevention of drowning should be on the global agenda.2 Detailed discussions about drowning prevention are beyond the scope of this tutorial. The World Health Organisation (WHO) has published a guide of preventative measures.2 Unintentional drowning-associated mortality is generally higher in children, in males and in countries with a low to middle sociodemographic index.3
Definition
PATHOPHYSIOLOGY
The pathophysiology of drowning is complex, largely unknown and different between immersion and submersion events. At the same time, an initial immersed victim can become submerged. As a result, various pathophysiological events in different combinations and time sequences may take place. This tutorial will discuss theories most relevant for anaesthesiologists.6
Effect of Water Temperature
Effects of Immersion in Hot Water
Water temperature can significantly influence drowning pathophysiology. Drowning in warm water mainly occurs in Japan, where Ofuro bathing is part of the culture and believed to have beneficial homeostatic effects. Drowning occurs while leaving a hot bath due to loss of hydrostatic pressure from the water. This induces hypotension, leading to hypoperfusion of critical organs. This poses a threat in elderly individuals and especially those with coexistent hypertension, coronary artery disease and congestive heart failure.6
Peripheral Effects of Immersion in Cold Water
Although it is expected that more drownings will occur in tepid or warm water due to climate change, prolonged immersion in cold water occurs more frequently than immersion in warm water. Cold shock, cooling of superficial nerves and muscles and hypothermia initiate central responses that may lead to drowning. In case of sudden immersion in cold water, a cold shock may develop due to intense stimulation of cold receptors in the skin. This causes reflexive gasping and hyperventilation. Gasping and hyperventilation depress breath-holding, which increases the risk of aspiration of water and drowning.6
After cooling of the skin, superficial nerves and muscles are functionally depressed by cold temperature. Muscle performance declines by approximately 5% for every degree reduction in muscle temperature. Muscle temperatures below 208C reduce the velocity and amplitude of nerve action potentials. Muscle temperatures of 5-158C may lead to peripheral nerve blockade. Cooling of muscles and nerves in the limbs may cause an individual to drown by physical incapacitation before central hypothermia sets in.6
Central Effects of Immersion in Cold Water
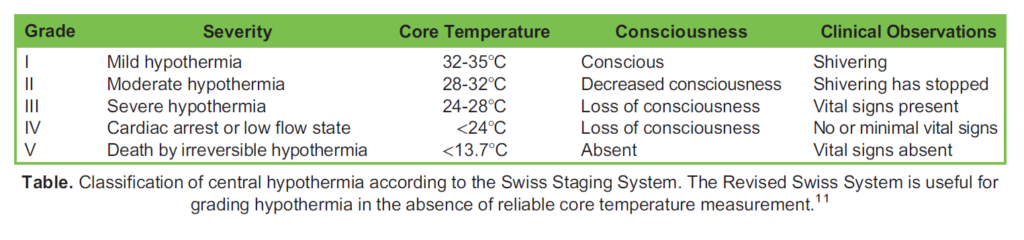
Central hypothermia has several stages, although clinical presentation may not always correlate with actual temperature (Table). Central hypothermia slows cellular metabolism in all organs. This reduces the function of the brain, heart and lungs. Impairment of one or more of these organs may convert an immersion event to a submersion event due to decreased consciousness and cardiac or respiratory failure.6
Cardiovascular effects include progressive bradycardia through a direct effect on pacemaker cells, with progressive slowing down of myocardial conduction. Ventricular fibrillation (VF) may occur spontaneously at temperatures below 288C or after manipulation of individuals with less severe hypothermia. Coagulation disorders may occur due to changes in blood viscosity and dysfunction of coagulation factors. Circulatory failure induces metabolic acidosis. Acidosis may worsen during therapeutic rewarming due to improved perfusion in the organs that had been in a hypoxic state. Other contributors to metabolic acidosis include ineffective metabolism of glucose and lactate in the liver and reduced renal capacity to maintain acid-base homeostasis.6
Individuals with severe hypothermia are deeply comatose. Clinical observations of vital signs may be difficult due to low respiratory rate and severe bradycardia. There may also be absent reflexes and dilated pupils, which may lead one to conclude that the individual is dead. For this reason, a traditional quote is that “no one is dead until warm and dead.” The implication is that attempts to rewarm deeply hypothermic persons need to be initiated before the person can formally be declared dead.6,7
Breath Holding and Diving Reflex
When submersion occurs, breath-holding ability is crucial. The urge to breathe can be temporarily suppressed by swallowing. This may prolong breath-holding time until levels of oxygen and carbon dioxide in the blood drive an irresistible urge to breathe. Breath-holding time is influenced by multiple factors such as metabolic rate, prior hyperventilation and experience with the unpleasant physical sensations of prolonged breath holding. Alcohol intoxication decreases breath-holding time and, in the context of cold shock, breath holding can become impossible. Breath-holding time can vary; in cold water, a range of 10-100 seconds is described, while in warm water, 45 seconds to 20 minutes have been described, with the latter occurring in experienced divers after preoxygenation.6,8,9
Next to breath holding, the diving reflex may explain why drowning victims are able to survive after long-lasting submersion. This is a cardiovascular response protecting against hypoxia and is most active in children. Activation of facial cold receptors results in peripheral vasoconstriction and bradycardia, reducing the total body oxygen consumption and delaying oxygen desaturation.6,9
Laryngeal Spasm and Aspiration
Laryngeal spasm may be protective until a quick rescue occurs but under water will quickly resolve with progressive hypoxia and continuing attempts to breathe. On the other end, the occurrence of laryngeal spasm may cause extraordinary negative hydrostatic pressures during forceful inspiration efforts, resulting in transudate in the alveoli and pulmonary oedema.6
During the process of water aspiration, the surfactant in the alveoli is damaged and washed away, causing alveolar collapse, ventilation-perfusion mismatch, shunting and respiratory insufficiency. Aspiration of dirty water or stomach contents will often result in pneumonia.6
Aspiration of hypo- or hypertonic water also damages the alveolar-capillary membrane by changing the oncotic/hydrostatic pressure balance acting on alveolar capillaries. This results in plasma leaking into alveoli, causing pulmonary oedema. Pulmo- nary oedema may also occur due to changes in the permeability of the blood-lung barrier because of increases in circulating catecholamines brought about by hypoxia and stress. Plasma entering alveoli further endangers oxygenation and ventilation through the formation of intercellular oedema and foam in the alveoli and airways.6
Most postmortem examinations typically show traces of liquid in the lungs from aspiration. The absence of liquid in the lungs after death by drowning is usually explained by the occurrence of laryngeal spasm; alternatively, dry lungs may be explained by the individual being deceased before immersion or submersion.6
Neurophysiology
Neurologic outcome plays an important role in mortality and morbidity after drowning. The details of the cerebral changes with drowning are still largely unknown. The speed with which hypoxia, due to asphyxia, and hypothermia (if present) occur seems to influence cerebral changes and neurological outcome. The speed of cooling down is determined by the temperature of the water and how much cold water has been inhaled or ingested. Cerebral blood flow after drowning declines quickly with sub- mersion in cold water. Blood flow is about 50% less at a water temperature of 08C. Hyperventilation may cause a drop in arte- rial pCO2, resulting in cerebral vasoconstriction. The reduction in cerebral blood flow is less if individuals can suppress hyperventilation and have adapted to cold temperatures.10
The amount of time the brain is able to withstand oxygen and energy substrate depletion is strongly correlated with temperature. Rapid cooling of the brain before the occurrence of hypoxic circulatory arrest can be crucial for a good prognosis. Cerebral protection is greater with hypothermia at the moment of circulation loss. In these victims, the brain has the time to cool down while cardiac arrest has not yet occurred. Once it occurs, the hypothermic brain will be better protected against the effects of progressive hypoxia.6,10
TREATMENT
Most drowning victims are able to save themselves or are rescued by bystanders or professionals and do not require medical care. Medical care is necessary in 1-6% of all rescues, and less than 0.5% of all rescues involve basic life support (BLS). This tutorial provides an overview of best practice treatment; however, there is only evidence from observational studies to inform clinical practice guidelines for drowning. Existing evidence is mainly from high-income countries and lacks uniformity.11,12
The Breathing Patient
When confronted in the emergency department with a breathing drowning victim, a regular airway–breathing–circulation (ABC) approach, with emphasis on early oxygenation, is best practice. Assessment of adequate respiration and oxygenation is based on clinical assessment of vital signs, auscultation of the lungs, pulse oximetry, blood gas analysis, chest X-ray and, recently, lung ultrasound.13 Hypoxia in drowning victims is due to a combination of respiratory insufficiency and fluid in the lungs. It may necessitate the use of positive end-expiratory pressure (PEEP) to improve oxygenation. If appropriate, noninvasive ventilation (NIV) can be used. Use of NIV might avoid the need for intubation in noncomatose individuals. Effective NIV in drowning is mainly observed in haemodynamically stable persons with an initial Glasgow Coma Scale score >12.14 The treatment of drowning victims requiring respiratory support resembles the treatment of an individual with acute respiratory distress syndrome, although a drowning victim has the potential to recover more quickly. In most patients, 48 hours of ventilation are needed for adequate surfactant regeneration.6,7
Although hypoxemia is the main factor influencing outcome in drowning victims, persistence of hypothermia plays a role as well. When rescuers fail to properly insulate the body of the drowning victim, hypothermia may progress. Further cooling down after a rescue especially may occur if the individual is unable to shiver due to deep hypothermia or exhaustion. As a consequence of this, loss of consciousness and respiratory depression may occur, which can contribute further to hypoxemia. Treatment of existing hypothermia as well as minimisation of ongoing decreases in core temperature is essential to diminish the risk of circulatory arrest from deep hypothermia.7
Risk of aspiration may be increased through attempts to remove water from the lungs with abdominal compressions or downward positioning of the head. These manoeuvres should be avoided. Prophylactic antibiotic treatment is not indicated as the bacterial load in pools, rivers and beaches is often insufficient to induce pneumonia. Pneumonia develops in less than 15% of drowning victims admitted to hospital. Antibiotic treatment based on clinical and radiologic findings alone is not advised and should be based on positive cultures. In addition, prophylactic antibiotic treatment is associated with a higher rate of therapy- resistant hospital-acquired infections. The incidence of pneumonia increases to 34-52% in the third or fourth week of hospitalisation among those who remain ventilated, and close monitoring of infection parameters and cultures is needed when a drowned person remains on a ventilator for a prolonged period of time.7,14
The Nonbreathing Patient
In a nonbreathing victim, cardiopulmonary resuscitation according to BLS or advanced life support (ALS) guidelines has usually been started in the prehospital setting. BLS is most effective when started with five initial rescue breaths as the most likely cause of arrest is hypoxia. Initial ventilations with high insufflation pressure are often needed with an aim to overcome impaired lung compliance due to fluid and foam occluding the airways.6,7,11 Although true for all resuscitations, it is important to under- stand that the sooner after drowning that ventilation is started, the better the neurologic prognosis. This has to do with the anoxic cause of the cardiac arrest resulting either in a person who looks dead but still has circulation (in which ventilation will improve circulation) or in an oxygen-depleted person at the start of the resuscitation (where it makes no sense to circulate hypoxic blood by compressions only). Under certain circumstances, a trained rescuer may even be able to commence assisted ventilation while the person is still in the water.7,11,12
In general, a cardiac arrest caused by anoxia is preceded by a period of progressive bradycardia and nonshockable rhythm disorders; VF is rare. For this reason, the use of an automated external defibrillator (AED) has a low priority in drowning resus- citation and it is better to attach the AED once good-quality BLS is performed.7,11,12
Hypothermia in drowning victims may, however, complicate BLS and ALS because vital signs are difficult to detect in extreme hypothermia. The best approach is for the first person to allow 1 minute for detection of vital signs while a second person commences rescue breaths. Intubation should not be delayed considering the benefits of adequate oxygenation and protection against aspiration outweigh the risk of inducing VF through manipulation of the individual.7
Hypothermia may render the heart unresponsive to cardioactive medications, electric pacing or defibrillation. It may also predispose to medication toxicity due to slowed metabolism and excretion. In individuals with a temperature below 308C, medication should not be administered. Between 30 and 358C, medication dosing intervals should be doubled compared with regular dosing.7
Because most arrhythmias disappear after warming, and because bradycardia in hypothermia is physiological, pacing is indicated only in the event of a persistent clinically relevant bradycardia after reaching normothermia. In the rare case of VF in an individual with a temperature below 308C, a defibrillator shock may be delivered according to the ALS protocol with a maximum of three. However, response to the shocks may not occur unless the core temperature increases to mild hypothermic levels.6,7,11
The use of a thermometer capable of measuring extreme temperatures is essential to guide resuscitation after drowning. Lower oesophageal temperature correlates well with heart temperature, but most importantly, temperature measurement should be from a consistent site. Although treatment may require a deviation from the standard ALS protocol, hypothermia protects the brain against hypoxia when the hypothermia has preceded asphyxia.6,7
Drowning victims suffering cardiopulmonary arrest may respond to extracorporeal life support (ECLS). ECLS, when available, may play a role in resuscitation as well as in rewarming the individual. Rewarming using ECLS may be considered in individuals with a core temperature <328C and potassium levels <8 mmol/L. Promising results with ECLS in drowning victims have been observed in young individuals with hypothermia <288C. The preferred technique is veno-arterial extracorporeal membrane oxygenation because of the ability to maintain circulatory support after warming and the limited need for anticoagulation.15,16
During warming, vasodilation can occur and may require additional resuscitation measures. In cases of return of spontaneous circulation (ROSC), standard ALS protocol should be followed. This includes goals of preventing hyperthermia, either caused by infection or other mechanisms, aiming for normal electrolyte balance, normoglycemia and prevention of secondary brain damage. The decision to persist with aggressive resuscitation in victims who might respond to this treatment is a difficult one and should be reserved for experienced physicians.7,10,17,18
PROGNOSIS
There are several factors that can improve prognosis. All of these factors are related to a short hypoxia period and include a shorter duration of submersion due to rapid rescue by bystanders and quicker arrival of skilled personnel to maintain resuscitation.7,17 Rescuers should, however, also consider their own safety first when attempting a rescue; every year many individuals drown trying to help a drowning victim.19 Factors that are associated with a poorer prognosis include finding the victim unconsciousness with dilated unresponsive pupils, need for intubation on scene or upon arrival at the emergency department and victims needing to receive ECLS who are severely acidotic.12,17
SUMMARY
Drowning injury involves many scenarios in which hypoxia, temperature, inhalation of liquid, duration of insult and initiation and quality of rescue and resuscitation all play important roles. Hypothermia is the most common accompaniment to a cardiorespiratory insult and can significantly influence management. Hypothermia being present before hypoxia may be protective. Resuscitation should prioritise treatment of hypoxia commencing with 5 rescue breaths and the introduction of PEEP through either NIV or invasive ventilation. During ongoing resuscitation, the impact of severe hypothermia on circulation should be considered as these may necessitate deviation from standard protocols of resuscitative management.
REFERENCES
- Franklin R, Peden A, Hamilton E, et al. The burden of unintentional drowning: global, regional and national estimates of mortality from the Global Burden of Disease 2017 Study. Inj Prev. 2020;26:i83-i95.
- Scarr JP, Jagnoor J. Identifying opportunities for multisectoral action for drowning prevention: a scoping review. Inj Prev. 2022;28(6):585-594. doi:10.1136/ip-2022-044712
- World Health Organization. Preventing Drowning: An Implementation Guide. 2017. Accessed June 23, 2023. https://www. who.int/publications-detail-redirect/9789241511933
- World Health Organization. Fact Sheet: Drowning. Accessed June 23, 2023. https://www.who.int/news-room/fact-sheets/ detail/drowning
- Van Beeck E, Branche C, Szpilman D, Modell J, Bierens J. A new definition of drowning: towards documentation and pre- vention of a global public health problem. Bull World Health Org. 2005;83:853-856.
- Bierens J, Lunetta P, Tipton M, Warner D. Physiology of drowning: a review. Physiology. 2016;31:147-166.
- Szpilman D, Morgan P. Management of the drowning patient. Chest. 2021;159(4):1473-1483.
- Suggitt C. 56-year-old freediver holds breath for almost 25 minutes breaking record. Guinness World Records. Published May 12, 2021. Accessed June 23, 2023. https://www.guinnessworldrecords.com/news/2021/5/freediver-holds-breath-for- almost-25-minutes-breaking-record-660285
- Tetzlaff K, Lemaitre F, Burgstahler C, Luetkens JA, Eichhorn L. Going to extremes of lung physiology-deep breath-hold div- ing. Front Physiol. 2021;12:710429.
- Topjian A, Berg R, Bierens J, et al. Brain resuscitation in the drowning victim. Neurocrit Care. 2012;17(3):441-467.
- Truhlár A, Deakin C, Soar J, et al. European Resuscitation Council guidelines for resuscitation 2015 section 4. Cardiac arrest in special circumstances. Resuscitation. 2015;95:148-201.
- Bierens J, Abelairas-Gomez C, Barcala Furelos R, et al. Resuscitation and emergency care in drowning: a scoping review. Resuscitation. 2021;162:205-217.
- Bloise S, Martucci V, Marcellino A, Sanseviero M, Lubrano R. Lung ultrasound in children drowning victims in pediatric emergency department. Pediatr Int. 2022;64(1):e15095. doi:10.1111/ped.15095
- Michelet P, Bouzana F, Charmensat O, et al. Acute respiratory failure after drowning: a retrospective multicenter survey. Eur J Emerg Med. 2017;24:295-300.
- Visser K, Schepp R. The treatment of accidental hypothermia and drowning with the aid of extracorporeal circulation/ ECMO. J Cardiothorac Surg. 2013;8(1):O83.
- Jasny T, Kloka J, Old O, et al. Results from 237 extracorporeal membrane oxygenation runs with drowned patients: a nationwide retrospective study. Crit Care. 2023;27(1):293. doi:10.1186/s13054-023-04580-w
- Quan L, Bierens J, Lis R, Rowhani-Rahbar A, Morley P, Perkins G. Predicting outcome of drowning at the scene: a system- atic review and meta-analyses. Resuscitation. 2016;104:63-75.
- Brennan CE, Hong TKF, Wang VJ. Predictors of safe discharge for pediatric drowning patients in the emergency depart- ment. Am J Emerg Med. 2018;36(9):1619-1623. doi:10.1016/j.ajem.2018.01.050
- Lawes JC, Rijksen EJT, Brander RW, Franklin RC, Daw S. Dying to help: fatal bystander rescues in Australian coastal environ- ments. PLoS One. 2020 Sep 16;15(9):e0238317. doi:10.1371/journal.pone.0238317
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/