Cardiothoracic Anaesthesia

KEY POINTS
- Children born with hypoplastic left heart syndrome rely on a single right ventricle to supply both the systemic and pulmonary circulations.
- A series of surgical procedures are carried out to separate the circulations, with systemic venous return ultimately draining directly to the pulmonary artery and the right ventricle pumping to the systemic circulation.
- It is essential to consider the stage of palliation, the target oxygen saturation and what effect supplemental oxygen or intubation and ventilation will have on cardiac output and function.
- IV fluid resuscitation and inodilators are key components of resuscitation, with intubation and ventilation reserved for cases of severe systemic hypoperfusion.
- As survival increases, complications associated with the single-ventricle circulation have also increased.
INTRODUCTION
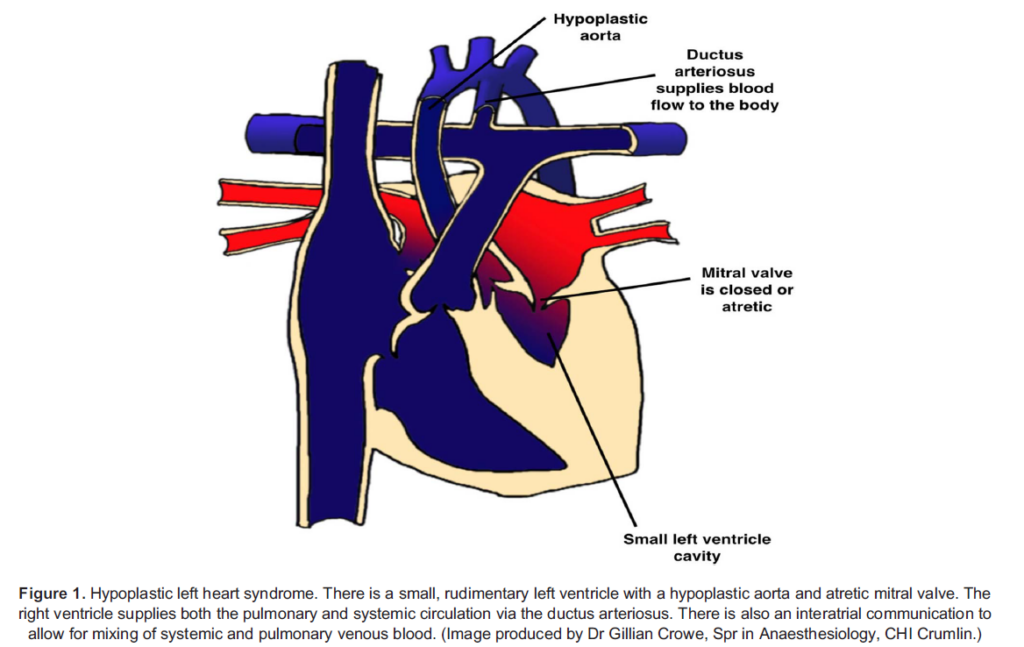
Hypoplastic left heart syndrome (HLHS) is one of the most complex congenital cardiac lesions. It is characterised by a small, rudimentary left ventricle with a hypoplastic aorta and atretic mitral valve (Figure 1). There is complete obstruction to systemic blood flow, and the right ventricle supplies both the pulmonary and systemic circulation via the ductus arteriosus. The prevalence of HLHS is 31/100,000 live births, and it is fatal without intervention.1 Staged palliative procedures have improved survival rates over the past 40 years, but these patients remain an extremely complex and high-risk cohort. This tutorial aims to provide a basic under- standing of the underlying anatomy and physiology at each stage of the single-ventricle palliation pathway and provide the knowl- edge required to initiate stabilisation and resuscitation of these patients if they present to nonspecialist centres.
UNDERLYING PHYSIOLOGY
Normal Neonatal Physiology
At birth, clamping of the umbilical cord and separation from the placenta causes a significant rise in the systemic vascular resistance (SVR) due to loss of the low-resistance placental bed. Simultaneously, initiation of alveolar ventilation and an increase in arterial oxygen content (PaO2) causes a reduction in pulmonary vascular resistance (PVR) and an increase in pulmonary blood flow.2 These changes combine to cause a reduction in right atrial pressures and an increase in left atrial pressures with commencement of a normal circulation in series, whereby deoxygenated blood drains to the right side of the heart before being transported to the lungs for oxygenation and then drained back to the left side of the heart to supply the systemic circulation.
In utero, the ductus arteriosus connects the aorta to the main pulmonary artery and allows shunting of most of the right ventricular output away from the nonfunctional, high-pressure pulmonary circulation to the systemic circulation. However, with initiation of the first breath and exposure to increased levels of arterial oxygen and decreased levels of prostaglandins, the duct begins to close at 24 to 48 hours of life with complete closure usually achieved after two to three weeks.3 The foramen ovale is a defect in the interatrial septum that allows foetal blood in utero to pass from the right to left atrium, bypassing the pulmonary circulation and supplying oxygen and nutrient-rich blood to the brain. The foramen will also start to close as a result of rising left atrial pressures after institution of a postnatal circulation, with complete closure usually by one year of age. For further reading, please see ATOTW number 91.
HLHS
Children with HLHS rely on a single right ventricle to perfuse both the systemic and pulmonary vascular beds via a parallel circulation. To achieve this, they require the presence of two shunts4:
- An intracardiac shunt, usually at the atrial level, to allow for mixing of oxygenated and deoxygenated pulmonary and systemic venous return, respectively
- A pulmonary-to-systemic shunt, usually at the level of the ductus arteriosus, to provide systemic blood flow in the presence of systemic outflow tract obstruction
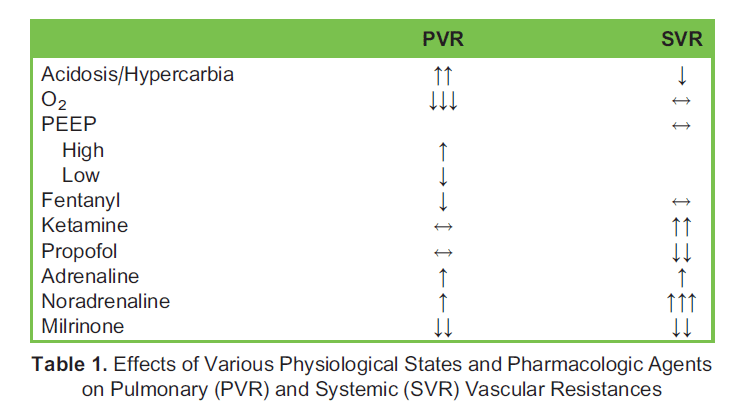
The amount of blood flowing to the pulmonary (Qp) and systemic (Qs) vascular beds is determined by the relative resistances in each. In a normal postnatal circulation, blood flow is balanced, and Qp:Qs is 1. However, in an unpalliated HLHS circulation, anything that decreases PVR or increases SVR will cause a rise in pulmonary blood flow and a reduction in systemic blood flow (Qp:Qs > 1). In this situation, although blood will be well oxygenated, there may be poor systemic perfusion and possible end-organ ischaemia resulting in complications such as necrotising enterocolitis or an acute kidney injury. The excess pulmonary blood flow may also lead to congestive cardiac failure, pulmonary oedema, impaired gas exchange and pulmonary hyper- tension in the long term. The opposite is seen in any situation that increases PVR and decreases SVR, whereby pulmonary blood flow will be poor and oxygenation impaired despite adequate systemic perfusion (Qp:Qs < 1). The physiological factors and pharmacologic agents that affect PVR and SVR are summarised in Table 1.4
In children with HLHS, peripheral oxygen saturations (SpO2) can be used as a surrogate marker for measuring Qp:Qs using the modified Fick principle.5 This states that

However, as aortic and pulmonary artery saturations are identical in a patient with single-ventricle physiology, this can be simplified to

In a neonate, it is assumed that the lungs are relatively healthy, and pulmonary venous saturations are 95% to 100% in room air. It is also assumed that the arterial-venous saturation difference is within normal limits at roughly 25%. Given these assumptions, an SpO2 of 75% to 85% represents a balanced circulation with a Qp:Qs of 1 in children born with HLHS.6
Unfortunately, using this simple approach to estimating Qp:Qs is not without its pitfalls. The assumption of normal healthy lungs and sufficient cardiac output to maintain a normal mixed venous oxygen saturation (SmvO2) is not always a reality in HLHS, and it is important to be mindful of this when assessing these infants.7,8
MANAGEMENT AT EACH STAGE OF THE PALLIATION PATHWAY
A series of staged surgical procedures, which ultimately result in passive systemic venous return to the lungs while the single functioning right ventricle supplies blood to the systemic circulation, remain the primary technique for palliation of children with HLHS resuscitation of these children follows the same basic principles as any other patient. However, it is essential at every stage of the palliation pathway to consider 3 important questions:
- Is it safe to deliver supplemental oxygen?
- Is controlled ventilation appropriate?
- How can I optimise cardiac output?
Unpalliated Neonate
Most cases of HLHS are diagnosed antenatally, and an infusion of prostaglandin E1 is commenced immediately after birth to maintain patency of the ductus arteriosus. Similarly, if flow across the interatrial septal defect is restrictive, then an urgent atrial septostomy may need to be performed to prevent pulmonary venous hypertension.9
Initial management prior to surgery is focused on optimising Qp:Qs to achieve a balanced circulation of 1:1. As PVR begins to drop in the first few days of life, SpO2 will increase, and these children are at risk of developing pulmonary overcirculation (Qp:Qs > 1). If there is evidence of systemic hypoperfusion, a series of stepwise interventions (summarised in Figure 2) should be followed.
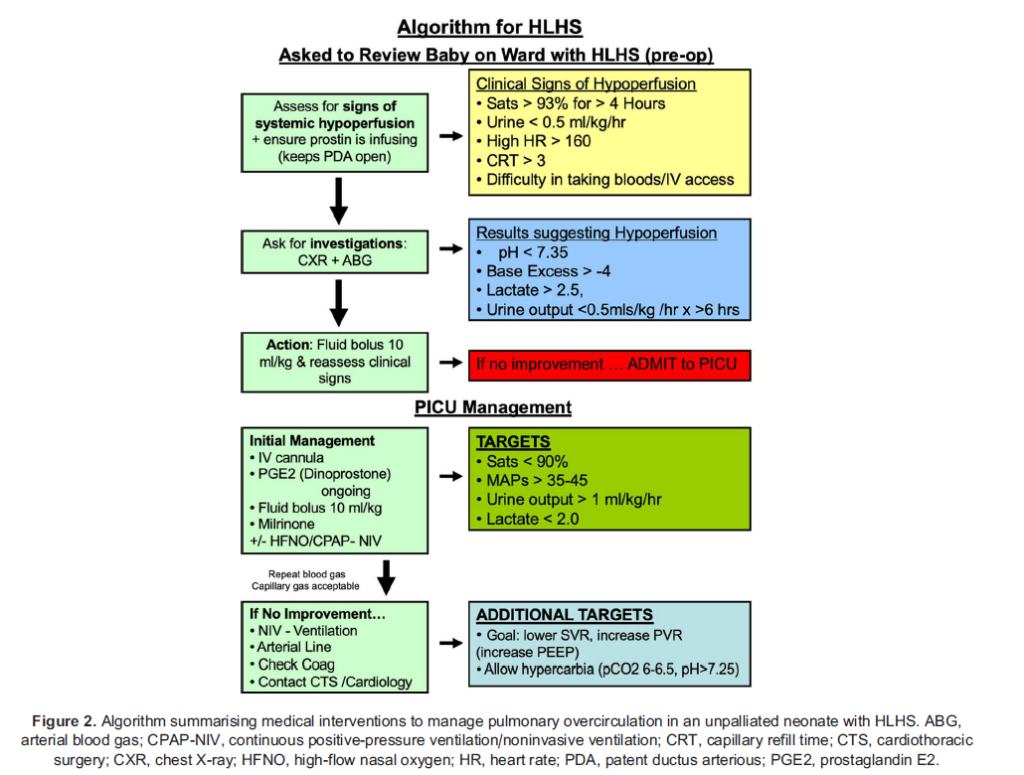
These involve the following:
- Optimising cardiac output: This will improve both Qp and Qs and is best achieved through the use of intravenous (IV) fluids and Phosphodiesterase inhibitors such as milrinone are ideal as they have the advantage of lowering SVR as well as positive inotropy.7 High-flow nasal oxygen (HFNO) therapy and noninvasive ventilation (NIV) have also been shown to augment systemic ventricular output by reducing afterload.10 These may be commenced, using minimal inspired oxygen (FiO2), if there is ongoing concern for poor systemic perfusion.
- Lowering SVR: This is achieved primarily through the use of phosphodiesterase inhibitors.
- Increasing PVR: Oxygen is a potent pulmonary vasodilator and should be used with extreme caution only to achieve a target SpO2 of 75% to 85%. Allowing a mild respiratory acidosis is beneficial, as increased CO2 may reduce SVR and increase cardiac output as well as increase PVR.9 Spontaneous ventilation is preferable, but in cases of severe overcirculation, intubation and controlled ventilation may be necessary. Gentle application of positive end-expiratory pressure (PEEP) can then be used to compress the alveolar vessels and increase PVR.6
Unfortunately, these interventions are merely temporising measures, and surgical repair is ultimately the only definitive treatment.
Stage 1 Palliation
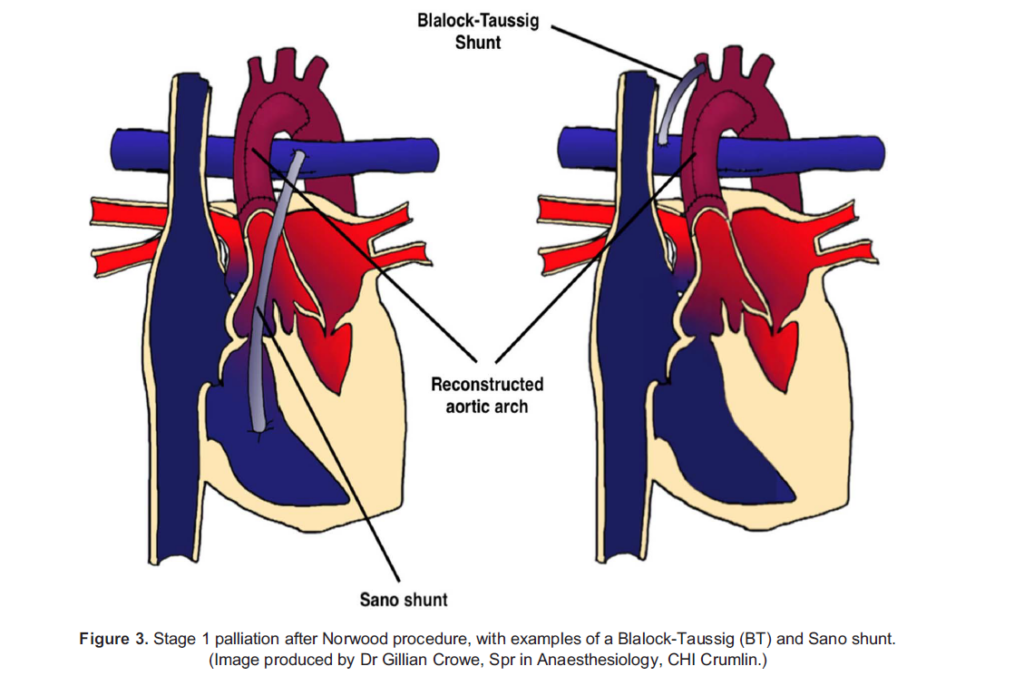
The primary goals of stage 1 palliation are to allow complete intracardiac mixing of oxygenated and deoxygenated blood, to generate a reliable pulmonary blood flow and provide unobstructed systemic perfusion. This creates a more stable and balanced circulation, allowing for prostaglandin to be ceased and growth of the child prior to further surgical repair. The most common stage 1 operation for HLHS remains the Norwood procedure (Figure 3), which is usually carried out between days 3 and 5 of life. This involves the following:
- Augmentation and reconstruction of the hypoplastic aortic arch
- An atrial septectomy to allow complete mixing of pulmonary and systemic venous return
- Ligation of the ductus arteriosus
- Formation of a systemic-to-pulmonary shunt to allow controlled pulmonary blood flow, either in the form of a Blalock-Taussig (BT) shunt from the subclavian or innominate artery to the right pulmonary artery or a Sano shunt from the right
ventricle to the pulmonary artery
After stage 1 palliation, infants still have a parallel circulation, with a single ventricle supplying both vascular beds, and they are at risk of developing pulmonary overcirculation. Interstage mortality is highest at this point, and postoperative myocardial dysfunc- tion and intercurrent illnesses are often poorly tolerated. Key concerns postoperatively are balancing Qp:Qs and optimising cardiac output. Treatment includes cautious use of supplemental oxygen only to maintain SpO2 between 75% and 85%, IV fluids, inodilators and HFNO/NIV to augment cardiac output, with intubation and ventilation reserved for cases of severe systemic hypoperfusion or shock. Shunt thrombosis is a life-threatening complication and should always be considered in cases of extreme hypoxia and shock. This requires immediate echocardiography for assessment and, if present, treatment with systemic heparinisation and urgent surgical intervention.
Stage 2: Bidirectional Glenn/Cavopulmonary Shunt
PVR continues to decrease over the first few months of life and by 3 to 6 months of age is sufficiently low to allow for passive nonpulsatile flow to the pulmonary vasculature. At this point, a bidirectional Glenn procedure is carried out, which involves the following (Figure 4):
- End-to-side anastomosis of the superior vena cava (SVC) to the right pulmonary artery
- Ligation of the BT/Sano shunt and exclusion of all other sources of pulmonary blood flow
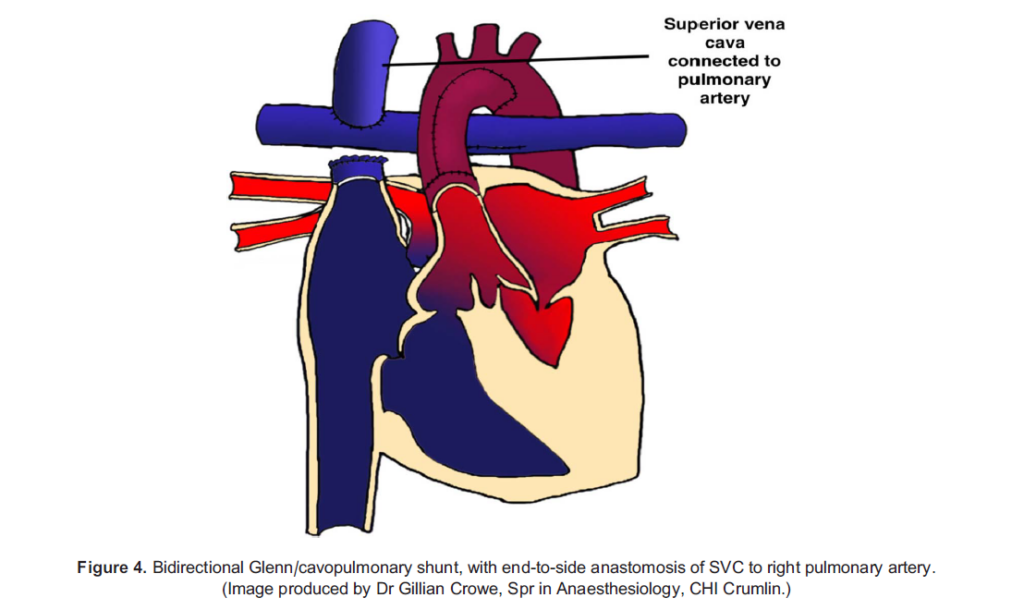
In children post-Glenn, passive SVC flow to the pulmonary arteries is the single source of pulmonary blood flow. This allows for lower pulmonary artery pressures as well as volume unloading of the single ventricle.11 However, an adequate intravascular volume and higher filling pressures are critical to maintaining pulmonary blood flow and cardiac output. Large-volume IV fluid resuscitation is often needed to prevent hypoxia and shock. Mixing of oxygenated and deoxygenated blood will still occur as the inferior vena cava (IVC) drains to the common atrium, with a target postoperative SpO2 of 80% to 85%.12 Oxygen therapy is not a concern, however, as there is no ability for systemic blood flow to shunt to the pulmonary vasculature.
The increased intrathoracic pressures generated by positive-pressure ventilation will cause a fall in SVC blood flow and may potentially worsen oxygenation and cardiac output. Intubation may be required in cases of severe respiratory failure or shock
but should be done with caution. Ventilation at minimal mean airway pressures, judicious use of PEEP and early extubation are advantageous.6 Hypoxia that does not improve after adequate volume resuscitation and optimal ventilation should raise concern for SVC or pulmonary artery thrombosis, the development of venous collaterals or a restrictive interatrial septum.12
Stage 3: Fontan/Total Cavopulmonary Circulation
As the child grows, the relative contribution of SVC flow to venous return diminishes.5 This limits the ability to increase pulmonary blood flow to match increasing demands, and cyanosis will develop. A Fontan circulation is carried out to complete the palliation pathway between 2 to 4 years of age and involves connecting the IVC to the pulmonary artery via a conduit (Figure 5). This allows all systemic venous blood to drain passively to the pulmonary circulation, separating the pulmonary and systemic vascular beds and creating a series circulation.
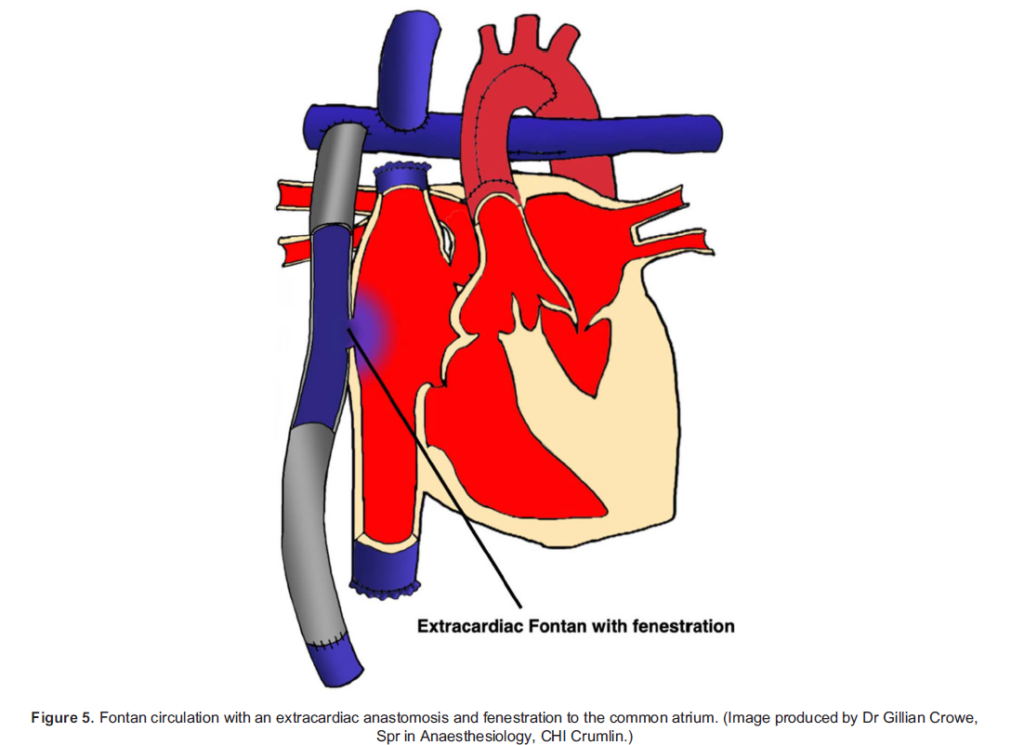
Pulmonary blood flow, and therefore cardiac output, relies entirely on passive venous filling. Any elevation in pulmonary artery pressures, whether it be due to mechanical obstruction from thrombosis, a high PVR or secondary to myocardial dysfunction, will result in cyanosis and shock. A fenestration is often made between the conduit and common atrium to support cardiac out- put by allowing a right-to-left shunt in such circumstances, providing a source of preload to the systemic ventricle that does not pass through the pulmonary circulation. This will occur at the expense of some arterial desaturation. Oxygen saturations are typically between 88% and 92% in a patient who has an atrial fenestration and should be close to normal where no fenestration has been created.12 The fenestration may then be closed at a later date when PVR has reached a consistently low level.5
Spontaneous ventilation enhances venous return and is preferable. These patients are extremely sensitive to changes in pre- load and poorly tolerate hypovolaemia or any reduction in vascular tone.13 Dehydration secondary to an intercurrent illness can easily precipitate a shocked state or thrombosis. The priorities for treatment are adequate volume replacement and optimising cardiac output with inodilators. Intubation and ventilation may be necessary in severe cases but must be done with extreme care to prevent a sudden reduction in preload and complete cardiovascular collapse. Induction agents such as propofol, with its vasodilatory and negative inotropic properties, should be avoided. Higher intrathoracic pressures will reduce pre- load, pulmonary blood flow and hence cardiac output and should be minimised by maintaining low mean airway pressures, short inspiratory times and judicious use of PEEP.14 Care must still be taken to optimise FiO2, PaCO2 and pH to prevent a rise in PVR.
The ‘Failing Fontan’
Although Fontan patients operated on today are expected to have a >80% 30-year survival rate, their altered anatomy and physiology creates serious complications in adulthood. Systolic and diastolic dysfunction, worsening exercise tolerance and cyanosis, thrombosis, arrhythmias, protein-losing enteropathy, hepatic and renal failure, plastic bronchitis, poor growth and neurodevelopmental complications all result from chronically elevated systemic venous pressures and a heart with limited ability to augment cardiac output.15 Standard pharmacological treatments for heart failure appear to have limited effect, with robust evidence lacking, and access to heart transplantation is often limited by comorbidities. There is clearly a dearth of knowledge about how best to manage these patients long term, and as the number reaching adulthood is only set to increase, more research is urgently needed to address this.
SUMMARY
Children born with HLHS are an extremely complex cohort of patients. Their underlying anatomy and physiology create unique challenges for anaesthesiologists and intensivists caring for them. Their resuscitation should follow the same basic principles as any other child, but it is essential at every stage of the palliation pathway to consider how simple interventions such as oxygen therapy or intubation and ventilation may greatly affect their haemodynamic stability.
REFERENCES
- Coats L, O’Connor S, Wren C, et The single-ventricle patient population: a current and future concern a population-based study in the North of England. Heart. 2014;100(17):348-353.
- Hooper SB, Te Pas AB, Lang J, et Cardiovascular transition at birth: a physiological sequence. Pediatr Res. 2015;77(5): 608-614.
- Doherty TM, Hu A, Salik Physiology, Neonatal. StatPearls [Internet]. Tampa, FL: StatPearls; 2023.
- Greaney D, Honjo O, O’Leary The single ventricle pathway in paediatrics for anaesthetists. BJA Educ. 2019;19(5):144-150.
- Schwartz SM, Dent CL, Musa NL, et Single-ventricle physiology. Crit Care Clin. 2003;19(3):393-411.
- Magoon R, Makhija N, Jangid Balancing a single-ventricle circulation: ‘physiology to therapy’. Ind J Thorac Cardiovasc Surg. 2020;36(2):159-162.
- Riordan CJ, Locher JP Jr, Santamore WP, et al. Monitoring systemic venous oxygen saturations in the hypoplastic left heart syndrome. Ann Thorac Surg. 1997;63:835-837.Yarlagadda VV, Almodovar Perioperative care of the infant with single ventricle physiology. Curr Treat Options Cardiovasc Med. 2011;13(5):444-455.
- Rao Single ventricle—a comprehensive review. Children. 2021;8(6):441.
- Inata Y, Takeuchi Complex effects of high-flow nasal cannula therapy on haemodynamics in the paediatric patient after cardiac surgery. J Intensive Care. 2017;5:30.
- Corno AF, Findley TO, Salazar Narrative review of single ventricle: where are we after 40 years? Transl Pediatr. 2023;12(2): 221-244.
- Roeleveld PP, Axelrod DM, Klugman D, et al. Hypoplastic left heart syndrome: from fetus to Fontan. Cardiol Young. 2018;28(11): 1275-1288.
- Jolley M, Colan SD, Rhodes J, et Fontan physiology revisited. Anesth Analg. 2015;121(1):172-182.
- McNamara JR, McMahon A, Griffin M. Perioperative management of the Fontan patient for cardiac and noncardiac sur- gery. J Cardiothorac Vasc Anesth. 2022;36(1):275-285.
- Rychik J, Atz AM, Celermajer DS, et Evaluation and management of the child and adult with Fontan circulation: a scientific statement from the American Heart Association. Circulation. 2019;140:e234-e284
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/