Critical Care

KEY POINTS
- Traditional inotropes mobilise myocardial calcium, increasing
- Levosimendan is a novel inotrope that sensitises the myocardium to calcium, increasing contractility without increasing oxygen consumption.
- Levosimendan also exhibits a host of other beneficial effects on the circulatory system, kidneys and liver via K+ and myocardial ATP channel activation.
- There is not enough evidence at present to recommend routine levosimendan use over standard inotrope
- Levosimendan is a useful inotrope in patients with Takotsubo
- Several other novel inotropes are either in development or are the focus of renewed interest, including the ancient Chinese traditional medicine Shenfu.
INTRODUCTION
Positive inotropes are drugs that enhance myocardial contractility independent of changes in heart rate or loading conditions. Therapeutic inotropic manipulation has a rich history. The ancient Chinese “Shenfu” formula has been used in Chinese traditional medicine for more than 2000 years to manage manifestations of heart failure: strengthening a deficient Yang 阳
(promoting water metabolism) and invigorating a deficient Qi 气 (increasing blood circulation).1
In 1775, the physician and botanist William Withering introduced the use of digitalis to treat the symptoms of heart failure,2 whereas the latter half of the 20th century saw the introduction of the beta-adrenergic agonists, such as dopamine and dobutamine, followed by nonsympathomimetic phosphodiesterase (PDE) inhibitors.3 Both catecholamines and PDE inhibitors act as myocardial calcium mobilisers and therefore share many of the same side effects.4 The use of inotropes may be lifesaving in the management of acute cardiogenic shock, but their use has been consistently associated with an increased morbidity and mortality.2 This has led to the search for alternative inotropic strategies, culminating in the introduction of the myocardial troponin calcium sensitiser, levosimendan, in the 1990s, which is still currently the only agent available in this class.3
In this review, we focus on levosimendan and outline the current evidence available regarding its safety and efficacy. We also describe several new experimental positive inotropic agents with novel pharmacodynamic mechanisms that may become available in the coming years. Finally, we outline how the abovementioned Shenfu formula, in modern intravenous form, has appeared recently in Western medical literature for use in septic shock and heart failure.5
LEVOSIMENDAN
Presentation
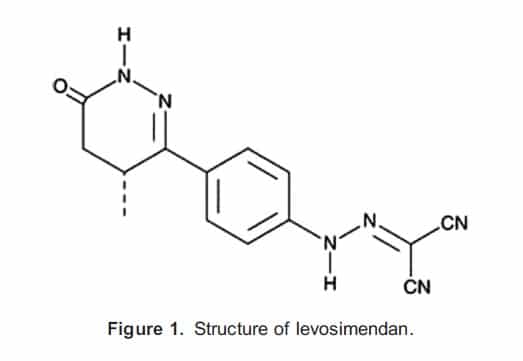
Levosimendan (Figure 1) is the active R enantiomer of simendan, with dextrosimendan (the S enantiomer) being 47 times less potent.6 The drug is usually presented in vials containing 2.5 mg/mL of a clear yellow solution. It is minimally water soluble.
Mechanisms of Action
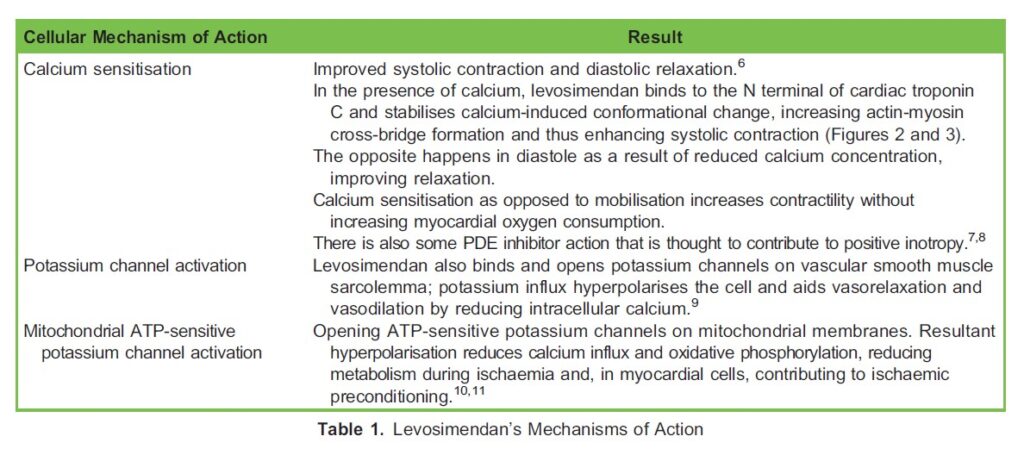
Levosimendan acts primarily by increasing calcium sensitisation in the myocardium, thereby improving both systolic contraction and diastolic relaxation. It also acts on potassium channels in vascular smooth muscle as well as ATP-sensitive potassium channels in the mitochondria (Table 1; Figures 2 and 3).
Pharmacokinetics of Levosimendan
Absorption and Distribution
Levosimendan is normally administered in its intravenous form; however, oral and transdermal preparations also exist. The oral presentation has a bioavailability of 85%. It is 98% protein bound, has a pKa of 6.3 and a volume of distribution of 0.2 L/Kg.
Metabolism and Excretion
Ninety-five percent of levosimendan is conjugated with glutathione to inert cysteine and renally excreted. The residual 5% is metabolised in the intestine to a biologically active metabolite, OR-1855, which is then N-acetylated to OR-1896. Although the elimination half-life of levosimendan is 1 to 1.5 hours, the same property for OR-1896 may exceed 80 hours.
The resultant accumulation of OR-1896 is responsible for the sustained effects of the drug after discontinuation of an infusion, often for up to 7 to 9 days. Therefore, the drug is usually administered as a 24-hour infusion.6
Pharmacodynamics of Levosimendan
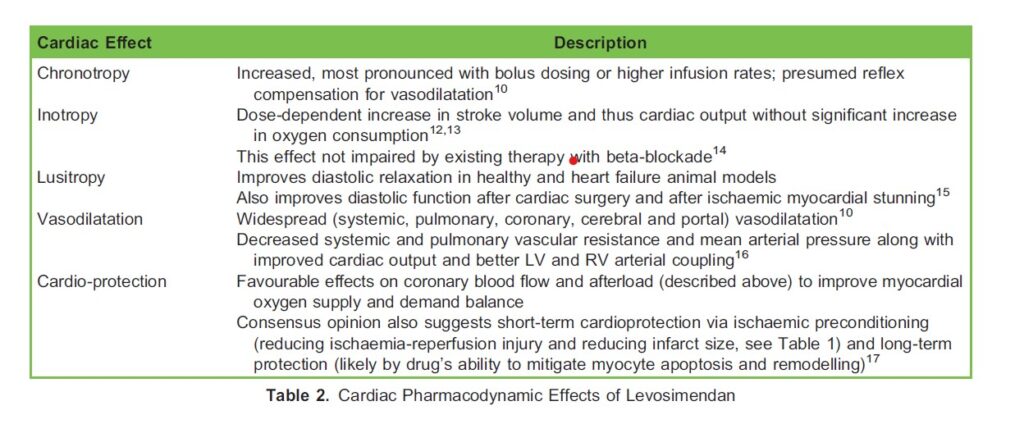
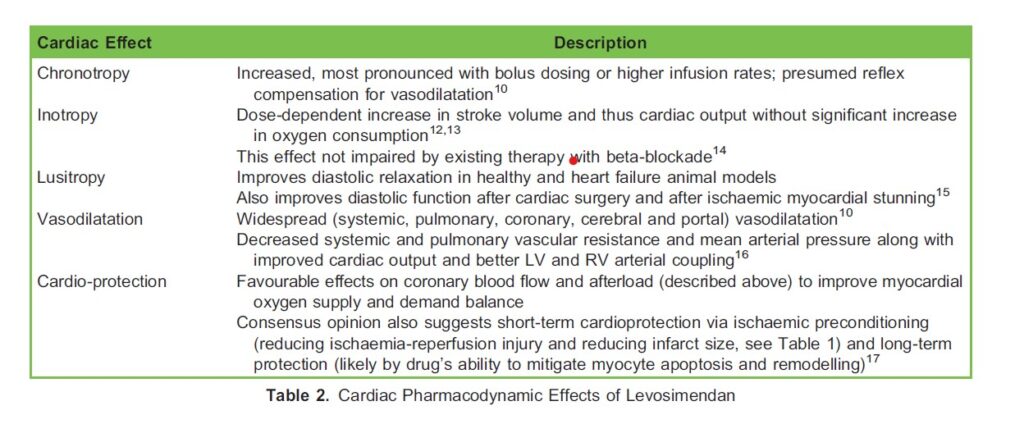
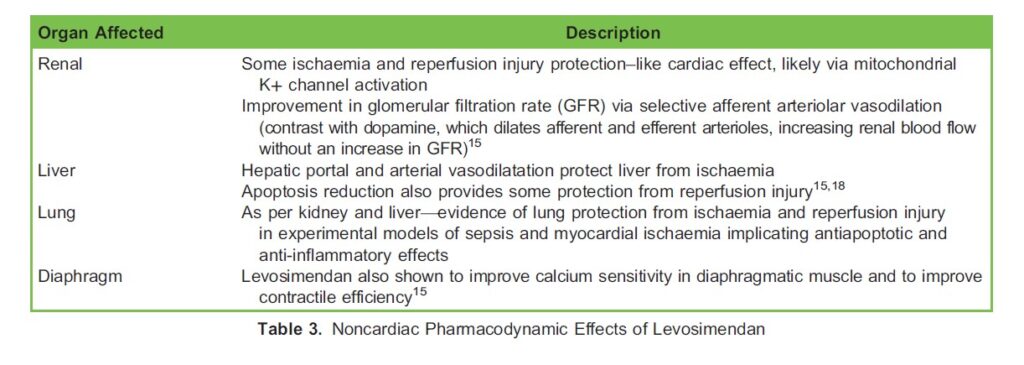
The effect site of most interest for levosimendan is the heart, where it affects inotropy and lusitropy, among others (Table 2). It also exerts positive effects on the kidneys, liver, lungs and diaphragm (Table 3).
Side Effects of Levosimendan
Levosimendan is usually well tolerated with few side effects, but the associated vasodilatation may cause dizziness and headaches and may precipitate hypotension. It is a positive chronotrope and causes tachycardia, enhances AV nodal conduction and reduces the refractory period. High doses prolong the QT interval. There is conflicting evidence regarding the drug’s propensity to cause arrhythmia, specifically atrial fibrillation.10
Indications and Evidence
Acute Heart Failure
In the 2016 European Society of Cardiology guidelines,19 inotropes are recommended in acute heart failure (AHF) for patients with hypotension (systolic blood pressure of ,90 mm Hg) and/or signs and symptoms of hypoperfusion. Levosimendan (or a PDE inhibitor) is recommended when beta-blockade is felt to be contributing to that hypoperfusion. The guidelines recommend the addition of a vasopressor in patients with a systolic blood pressure ,85 mm Hg to offset the vasodilatory effects.
Two early studies compared levosimendan to dobutamine in AHF: LIDO and SURVIVE.20 The small LIDO trial demonstrated that levosimendan’s mechanism of action is independent of beta-blockade and it signalled a mortality benefit. This was further evaluated in the more comprehensive SURVIVE trial, which showed an early decrease in mortality but no difference in longer term follow-up.
The REVIVE I and II studies evaluated levosimendan’s efficacy in treating symptoms of heart failure, showing improved symptoms and shorter hospital stays in patients receiving levosimendan, albeit with a trend to increased arrhythmias (atrial fibrillation and ventricular tachycardia).20 A recent expert review of the role of levosimendan in AHF complicating acute coronary syndrome asserted that levosimendan offers potential benefits in this setting. However, the only large randomised controlled trial evaluating levosimendan after myocardial infarction, the RUSSLAN trial, was primarily designed to evaluate safety and not efficacy for this indication.21
Other than the trials mentioned above, there is a paucity of evidence regarding the use of levosimendan in cardiogenic shock, despite its theoretically favourable characteristics. In the above expert review, the authors recommend avoiding bolus dosing and administering a 24-hour infusion at 0.05 to 0.1 μg/kg/min with the option of increasing to 0.2 μg/kg/min for 1 hour if a more rapid effect is required. As mentioned earlier, concurrent use of a vasopressor may be required.
Advanced Heart Failure
Levosimendan consistently leads to a rapid and sustained decrease in brain natriuretic peptide (BNP) in clinical trials.21 Recent randomised, controlled clinical trials have evaluated using levosimendan on a repetitive basis in patients with advanced heart failure (New York Heart Association III or IV symptoms). The LION-Heart, LAICA and Levo-Rep trials evidenced the safety and tolerability of repetitive use levosimendan in the outpatient setting. All 3 trials showed reductions in NT-pro-BNP levels and trends to a reduction in heart failure–related admissions or readmissions as well as mortality.22
Takotsubo Cardiomyopathy
Levosimendan’s properties would seem to confer unique benefits in the management of cardiogenic shock caused by catecholamine-mediated Takotsubo cardiomyopathy.3 Two small studies have shown accelerated recovery of ejection fraction and decreased length of hospitalisation, along with feasibility and safety, when levosimendan was administered to these patients, although a mortality benefit was not clear.23,24
Renal Perfusion
Evidence is conflicting, but levosimendan appears to have beneficial effects on renal function. These benefits may be mediated mainly through improved cardiac output and decongestion of the venous circulation of the kidney.22,25
Pulmonary Hypertension
The pharmacodynamics of levosimendan suggest a benefit in treating pulmonary hypertension and right heart failure, but there is limited evidence to support this.26 A recent meta-analysis studying the efficacy and safety of levosimendan showed some short-term efficacy in managing RHF of varying aetiology, albeit in small studies.27
Septic Cardiomyopathy
Septic shock is often characterised by vasoplegia, but this may be accompanied by septic cardiomyopathy (SCM). SCM is acute cardiac dysfunction, unrelated to ischaemia, in a patient with sepsis. It may complicate up to 60% of cases of septic shock.28
The most recent Surviving Sepsis Campaign international guidelines recommend dobutamine as the first-line inotrope in patients with measured or suspected low cardiac output assuming adequate left ventricular filling pressures.29 This is despite the fact that adrenergic overstimulation of the myocardium contributes to the pathophysiology of SCM and indeed the observation that esmolol, a β1 antagonist, may paradoxically improve outcomes in SCM.30 Levosimendan would therefore seem to be a promising inotropic drug in the context of SCM, although the evidence is not conclusive. A small study comparing levosimendan to dobutamine in sepsis after 48 hours of conventional therapy showed that levosimendan increased CO and decreased pulmonary congestion as well as increased lactate clearance, mucosal perfusion and renal function without an increase in vasopressor requirements—all factors that remained unaltered by dobutamine.31
The recent LeoPARDS trial, on the other hand, examining early administration of levosimendan in septic shock, was not able to show a difference in mortality or organ dysfunction (the primary endpoint) in patients given conventional therapy for septic shock when compared with the control group (conventional therapy plus a placebo infusion). This was accompanied by a higher incidence of supraventricular tachyarrhythmia and a reduced likelihood of successful extubation.30 The Surviving Sepsis Guidelines therefore question the systematic use of levosimendan and continue to prefer dobutamine.29
Cardiac Surgery
Levosimendan’s effects make it theoretically useful in the context of cardiac surgery. It has been extensively evaluated perioperatively, with most studies focusing on patients with decreased left ventricular ejection function (LVEF). Multiple small studies have shown levosimendan to be associated with improved haemodynamic parameters, a reduction in low cardiac output states postoperatively, decreased intensive care unit (ICU) lengths of stay and a decreased necessity for additional inotropic agents.
Several meta-analyses have demonstrated significant reductions in mortality and kidney injury in cardiac surgery patients with reduced LVEF.32 These findings led a panel of European experts to recommend a preoperative infusion of levosimendan in patients with “generally compromised myocardial function, including right ventricular function,” beginning 1 day preoperatively and continuing for 24 hours.33
The picture, however, has been clouded by the conclusions of 3 subsequent, large, randomised, controlled trials: the LEVO-CTS, CHEETAH and LICORN trials.32 All 3 compared levosimendan to placebo in cardiac surgery patients with low ejection fraction. None of these trials showed a significant difference in mortality, with the CHEETAH trial being stopped early for futility. LEVO-CTS and LICORN also studied ICU hospital length of stay, the need for renal replacement therapy and mechanical cardiac support. They did not find a significant difference in these outcomes. LICORN also found no significant difference in low cardiac output states or duration of catecholamine use.34 A more recent meta-analysis, which included these newer trials, concluded that the evidence does not currently support either prophylactic or therapeutic administration of levosimendan in cardiac surgery.35
OTHER NOVEL INOTROPIC AGENTS
There are a small number of novel inotropic agents, such as omecamtiv mecarbil and istaroxime, that have been developed recently and are undergoing study.36-38 Perhaps the most relevant globally might be Shenfu.
Shenfu injection (SFI) has a long history of use in China in the treatment of 厥脱, the Chinese traditional medical manifestation of shock, and as such cannot be considered to be novel. However, SFI has recently begun to appear in Western medical literature.39
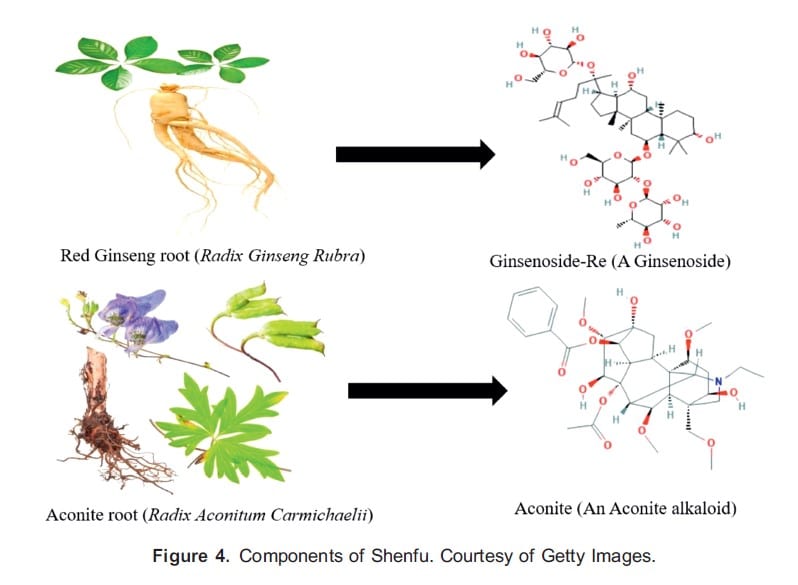
It is a traditional Chinese medicine composed of extracts of red ginseng roots (Radix Ginseng rubra) and aconite roots (Radix Aconitum Carmichaelii) (Figure 4). These components yield a preparation with multiple active ingredients.40,41
There are positive inotropic effects, including some direct beta- and alpha-agonism, as well as augmented catecholamine release, upregulation of β-adrenoreceptors and anti-inflammatory and antioxidant properties.42 Agonism of myocardial β-receptors is obviously not a novel inotropic strategy. However, some of the active ingredients in the mixture have also been shown to upregulate the expression of SERCA2a, decreasing myocardial cytosol calcium levels and protecting against myocardial apoptosis by inhibiting myocardial caspases, as well as decreasing plasma levels of tumour necrosis factor–α and other cytokines.43,44
Despite an extensive volume of publications involving SFI in Chinese medical literature, it is difficult to draw significant conclusions relevant to Western medicine. This is due to disparate methodologies and interpretations and the way in which Chinese traditional medicine is combined with established Western medical techniques in clinical practice in China. A recent randomised controlled trial studied the use of SFI following the return of spontaneous circulation after in-hospital cardiac arrest and showed a significant improvement in outcomes, including greater rates of survival and favourable neurologic outcomes.45 A 2021 meta-analysis of SFI in the management of heart failure concluded that it may be clinically effective and safe but advised the need for a more conclusive evidence base.46
CONCLUSION
Novel inotropic strategies have been in development in recent years to produce the desired clinical effects of improved left ventricular performance without the associated common adverse effects of traditional inotropic agents. Levosimendan entered clinical practice in 2001 but remains the only new inotropic agent currently available, with no conclusive evidence demonstrating a clear superiority or inferiority over standard inotropic drugs.47 There is evidence to suggest that standard inotropic drugs can increase mortality, and we have presented cases in which it may be prudent to use levosimendan as a first-line inotrope. The β-blocked patient suffering AHF or early Takotsubo syndrome are cases in point. However, using familiar and more established agents, backed by an evidence base and existing clinical guideline, will be the default option for most situations.
Other new inotropic agents are in development or in early clinical trials but are unlikely to be introduced into clinical practice soon. SFI, a traditional Chinese medicine that has long been used for a variety of cardiovascular indications in China, is now appearing more frequently in international medical literature. Although this ancient formula is not a novel inotrope, it is new to Western medicine, notwithstanding the fact that some of its effects likely derive from β-agonism. The use of Shenfu requires more robust evidence before it can be considered for use in Western medicine.
REFERENCES
- Fan KL, Wang JH, Kong L, et al. Effect of Shen-Fu injection () on hemodynamics in early volume resuscitation treated septic shock patients. Chin J Integr Med. 2019;25(1):59-63.
- Francis GS, Bartos JA, Adatya Inotropes. J Am Coll Cardiol. 2014;63(20):2069-2078.
- Papp Z, Agostoni P, Alvarez J, et Levosimendan efficacy and safety: 20 years of SIMDAX in clinical use. Card Fail Rev. 2020;6:e19.
- Nagy L, Pollesello P, Papp Inotropes and inodilators for acute heart failure: sarcomere active drugs in focus. J Cardiovasc Pharmacol. 2014;64(3):199-208.
- Mou Z, Lv Z, Li Y, Wang M, Xu Q, Yu Clinical effect of Shenfu injection in patients with septic shock: a meta-analysis and systematic review. Evid Based Complement Alternat Med. 2015;2015:863149.
- Kaheinen P, Pollesello P, Hertelendi Z, et al. Positive inotropic effect of levosimendan is correlated to its stereoselective Ca2+- sensitizing effect but not to stereoselective phosphodiesterase Basic Clin Pharmacol Toxicol. 2006;98(1):74-78.
- Haikala H, Kaheinen P, Levijoki J, Linde´n The role of cAMP- and cGMP-dependent protein kinases in the cardiac actions of the new calcium sensitizer, levosimendan. Cardiovasc Res. 1997;34(3):536-546.
- Orstavik O, Ata SH, Riise J, et Inhibition of phosphodiesterase-3 by levosimendan is sufficient to account for its inotropic effect in failing human heart. Br J Pharmacol. 2014;171(23):5169-5181.
- Yildiz Vasodilating mechanisms of levosimendan: involvement of K+ channels. J Pharmacol Sci. 2007;104(1):1-5.
- Toller WG, Stranz Levosimendan, a new inotropic and vasodilator agent. Anesthesiology. 2006;104(3):556-569.
- Soeding PE, Royse CF, Wright CE, Royse AG, Angus Inoprotection: the perioperative role of levosimendan. Anaesth Intensive Care. 2007;35(6):845-862.
- Nieminen MS, Fruhwald S, Heunks LM, et Levosimendan: current data, clinical use and future development. Heart Lung Vessel. 2013;5(4):227-245.
- Pollesello P, Papp Z, Papp Calcium sensitizers: what have we learned over the last 25 years? Int J Cardiol. 2016;203:543-548.
- Mebazaa A, Nieminen MS, Filippatos GS, et Levosimendan vs. dobutamine: outcomes for acute heart failure patients on beta-blockers in SURVIVE. Eur J Heart Fail. 2009;11(3):304-311.
- Farmakis D, Alvarez J, Gal TB, et Levosimendan beyond inotropy and acute heart failure: evidence of pleiotropic effects on the heart and other organs: An expert panel position paper. Int J Cardiol. 2016;222:303-312.
- Ukkonen H, Saraste M, Akkila J, et Myocardial efficiency during levosimendan infusion in congestive heart failure. Clin Pharmacol Ther. 2000;68(5):522-531.
- Papp Z, E´des I, Fruhwald S, et Levosimendan: molecular mechanisms and clinical implications: consensus of expertson the mechanisms of action of levosimendan. Int J Cardiol. 2012;159(2):82-87.
- Brunner SN, Bogert NV, Schnitzbauer AA, et al. Levosimendan protects human hepatocytes from ischemia-reperfusion injury. PLoS One. 2017;12(11):e0187839.
- Ponikowski P, Voors AA, Anker SD, et 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur J Heart Fail. 2016;18(8):891-975.
- Harjola VP, Giannakoulas G, von Lewinski D, et al. Use of levosimendan in acute heart failure. Eur Heart J Suppl. 2018; 20(suppl I):I2-I10.
- Gustafsson F, Guarracino F, Schwinger The inodilator levosimendan as a treatment for acute heart failure in various settings. Eur Heart J Suppl. 2017;19(suppl C):C2-C7.
- Altenberger J, Gustafsson F, Harjola VP, et al. Levosimendan in acute and advanced heart failure: an appraisal of the clinical database and evaluation of its therapeutic applications. J Cardiovasc Pharmacol. 2018;71(3):129-136.
- Yaman M, Arslan U, Kaya A, et Levosimendan accelerates recovery in patients with takotsubo cardiomyopathy. Cardiol
- J. 2016;23(6):610-
- Santoro F, Ieva R, Ferraretti A, et Safety and feasibility of levosimendan administration in Takotsubo cardiomyopathy: a case series. Cardiovasc Ther. 2013;31(6):e133-e137.
- Pan J, Yang YM, Zhu JY, Lu Multiorgan drug action of levosimendan in critical illnesses. Biomed Res Int. 2019;2019:9731467.
- Hansen MS, Andersen A, Nielsen-Kudsk Levosimendan in pulmonary hypertension and right heart failure. Pulm Circ. 2018;8(3):2045894018790905.
- Qiu J, Jia L, Hao Y, et Efficacy and safety of levosimendan in patients with acute right heart failure: a meta-analysis. Life Sci. 2017;184:30-36.
- Beesley SJ, Weber G, Sarge T, et Septic cardiomyopathy. Crit Care Med. 2018;46(4):625-634.
- Rhodes A, Evans LE, Alhazzani W, et Surviving Sepsis Campaign: international guidelines for management of sepsis and septic shock: 2016. Crit Care Med. 2017;45(3):486-552.
- Herpain A, Bouchez S, Girardis M, et Use of levosimendan in intensive care unit settings: an opinion paper. J Cardiovasc Pharmacol. 2019;73(1):3-14.
- Morelli A, De Castro S, Teboul JL, et al. Effects of levosimendan on systemic and regional hemodynamics in septic myocardial depression. Intensive Care Med. 2005;31(5):638-644.
- Faisal SA, Apatov DA, Ramakrishna H, Weiner Levosimendan in cardiac surgery: evaluating the evidence. J Cardiothorac Vasc Anesth. 2019;33(4):1146-1158.
- Toller W, Heringlake M, Guarracino F, et al. Preoperative and perioperative use of levosimendan in cardiac surgery: European expert opinion. Int J Cardiol. 2015;184:323-336.
- Cholley B, Caruba T, Grosjean S, et Effect of levosimendan on low cardiac output syndrome in patients with low ejection fraction undergoing coronary artery bypass grafting with cardiopulmonary bypass: the LICORN randomized clinical trial. JAMA. 2017;318(6):548-556.
- Putzu A, Clivio S, Belletti A, Cassina T. Perioperative levosimendan in cardiac surgery: a systematic review with meta- analysis and trial sequential analysis. Int J Cardiol. 2018;251:22-31.
- Teerlink JR, Diaz R, Felker GM, et Cardiac myosin activation with omecamtiv mecarbil in systolic heart failure. N Engl J Med. 2021;384(2):105-116.
- Planelles-Herrero VJ, Hartman JJ, Robert-Paganin J, Malik FI, Houdusse Mechanistic and structural basis for activation of cardiac myosin force production by omecamtiv mecarbil. Nat Commun. 2017;8(1):190.
- Aditya S, Rattan Istaroxime: a rising star in acute heart failure. J Pharmacol Pharmacother. 2012;3(4):353-355.
- Varon A, Varon Shenfu, traditional Chinese medicine in sepsis: are we ready for it? Am J Emerg Med. 2015;33(9):1244-1245.
- Zhu J, Kang L, Ye Q, et Effects of Shenfu injection and its main components on the contraction of isolated rat thoracic aortic rings. PLoS One. 2013;8(10):e78026.
- Zhang Y, Tian D, Huang Y, et al. Pharmacokinetic evaluation of Shenfu injection in beagle dogs after intravenous drip Acta Pharm Sin B. 2016;6(6):584-592.
- Zhao D, Wang J, Cui Y, Wu X. Pharmacological effects of Chinese herb aconite (fuzi) on cardiovascular system. J Tradit Chin Med. 2012;32(3):308-313.
- Guo ZJ, Wu CJ, Li Shen-Fu injection () alleviates post-resuscitation myocardial dysfunction by up-regulating expression of sarcoplasmic reticulum Ca(2+)-ATPase. Chin J Integr Med. 2016;22(7):503-509.
- Huang P, Guo Y, Feng S, Zhao G, Li B, Liu Efficacy and safety of Shenfu injection for septic shock: a systematic review and meta-analysis of randomized controlled trials. Am J Emerg Med. 2019;37(12):2197-2204.
- Zhang Q, Li C, Shao F, Zhao L, Wang M, Fang Y. Efficacy and safety of combination therapy of Shenfu injection and postresuscitation bundle in patients with return of spontaneous circulation after in-hospital cardiac arrest: a randomized, assessor-blinded, controlled trial. Crit Care Med. 2017;45(10):1587-1595.
- Huang J, Wang Y, Huang S, et A critical overview of systematic reviews of shenfu injection for heart failure. Cardiovasc Ther. 2021;2021:8816590.
- Cholley B, Levy B, Fellahi JL, et Levosimendan in the light of the results of the recent randomized controlled trials: an expert opinion paper. Crit Care. 2019;23(1):385.
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/