General Topics

SELF-ASSESSMENT QUESTIONS
Please attempt the following questions before reading the tutorial.
- The following are true concerning malignant hyperthermia (MH):
- It is inherited in an autosomal recessive manner
- Accurate diagnosis can be made by DNA testing
- Patients have usually had previous uneventful general anaesthesia on diagnosis
- It is the most likely diagnosis when intraoperative hypercapnia and tachycardia are present
- Generalised muscle rigidity is a late sign
- Concerning master muscle spasm (MMS):
- It is defined as impeding intubation and lasting 2 minutes
- It is usually a sign of susceptibility to MH
- It may be a sign of other muscle diseases
- For anaesthesia after MMS it is advisable to avoid the use of MH trigger agents
- It is more common in children and young adults
- Concerning the management of malignant hyperthermia:
- Treatment should occur with dantrolene initial dose of 1mg/kg as soon as possible
- Recrudescence occurs in 25% of cases
- Active cooling should include ice packs to large areas of the body
- Mortality following prompt diagnosis and treatment is 2-3%
- Prophylactic dantrolene should be used in MH susceptible patients undergoing general anaesthesia
INTRODUCTION
Malignant hyperthermia (MH) is an uncommon pharmacogenetic disorder of muscle induced by exposure to suxamethonium and all the volatile anaesthetic agents. It is characterized by hypermetabolism, muscle rigidity and muscle injury.
AETIOLOGY
- MH susceptibility is inherited as an autosomal dominant condition with variable penetrance. Administration of triggering agents leads to an uncontrolled release of free calcium from the sarcoplasmic reticulum of skeletal muscle.
- This could be due to an abnormality at any point in the excitation-contraction coupling process, but the most likely site is the junction between the T tubule (involving the dihydropyridine receptor) and the sarcoplasmic reticulum (involving the ryanodine receptor, responsible for calcium efflux).
- In 50-70% of affected families there are links to the ryanodine receptor gene (RYR1) located on chromosome 19. This is a huge gene and many mutations have been identified, but only a small proportion has been shown to have an effect.
EPIDEMIOLOGY
- Incidence is approximately 1:10 000 – 15 000. All races are affected.
- Previous uneventful anaesthesia with triggering agents does not preclude MH. Seventy-five percent of MH index cases have had previous anaesthesia prior to their MH crisis (average 3 previous uneventful anaesthetics).
- Mortality rates have fallen dramatically from 70-80% to 2-3% due to increased awareness, improved monitoring standards and the availability of dantrolene.
CLINICAL PRESENTATION
Classic malignant hyperthermia.
The clinical features are a direct consequence of loss of skeletal muscle calcium homeostasis, resulting in increased intracellular calcium ion concentration, which causes muscle rigidity, hypermetabolism, and rhabdomyolysis. The diagnosis may be difficult as there is no one sign that is unique to MH, and the onset may be rapid or insidious.
- Unexplained increased CO2 production and tachycardia are the initial signs in the classic case. The rise in CO2 production results in tachypnoea in the spontaneously breathing patient or a rise in end-tidal CO2 in a ventilated patient.
- BP is often unstable, with a tendency for decreasing SpO2.
- Increase in body temperature occurs later, and may be at a rate of > 1 °C every 5 minutes.
- Generalised muscle rigidity, raised plasma CK and myoglobinuria are late signs.
- Cardiac arrhythmias, hyperkalaemia and disseminated intravascular coagulation maydevelop.
- Arterial blood gas analysis shows hypercarbia with respiratory and metabolic acidosis. Elevation of the end-tidal CO2 is one of the earliest, most sensitive and specific signs of MH. However, vigorous hyperventilation may mask hypercarbia and delay diagnosis.
In almost all cases, the first manifestations of the syndrome occur in the operating room but the interval between administration of triggering drugs and onset of symptoms is variable. The most rapid reactions have occurred after the use of suxamethonium followed by maintenance with a volatile agent. MH does not start after the trigger is removed, although it may only be identified in the recovery room. Therefore postoperative pyrexia will not be due to MH unless there is evidence of increased CO2 production or tachycardia in theatre or the very early recovery period. However confidence on assessing this is dependent on the quality of the notes.
Masseter muscle spasm
Rigidity of the jaw muscles after administration of suxamethonium, referred to as masseter muscle spasm(MMS) may be the first sign of possible susceptibility to MH. It is defined as impeding intubation and lasting for 2 minutes. It is more common in children and young adults and is not relieved by repeat doses of suxamethonium or non-depolarising relaxants. Over 25% of patients presenting with MMS alone will subsequently prove to be MH susceptible, even if anaesthesia has proceeded with volatile agents apparently uneventfully.
Only in rare cases does MH follow immediately after MMS. More commonly, if the anaesthetic is continued with a triggering agent, the initial signs of MH appear after 20 min or longer. If the anaesthetic is discontinued, the patient usually recovers uneventfully.
Therefore surgery should usually be postponed if possible. If surgery must be continued, it should be with non-triggering agents and the use of end-tidal CO2 and core temperature monitoring. After MMS, the patient should be observed carefully for 12-24 h for myoglobinuria and signs of MH. CK testing at 24 hrs is also useful.
MMS differential diagnosis:
- Myotonic syndrome
- Temporo-mandibular joint dysfunction
- Underdosing with suxamethonium
- Not allowing sufficient time for suxamethonium to act before intubation
- Increased muscle tone after suxamethonium in the presence of fever or elevated plasma catecholamine
MH differential diagnosis
- Inadequate anaesthesia or analgesia
- Inappropriate breathing circuit / fresh gas flow / ventilation
- Endocrine disorders: phaeochromocytoma and thyrotoxicosis Sepsis
TREATMENT OF MALIGNANT HYPERTHERMIA
Early diagnosis and treatment are key to successful management – on recognition of a reaction several modes of treatment need to be started at once. It is important to know where the dantrolene is kept in your theatre.
The acute episode
Call for help
Take measures to stop the MH process
- Discontinue the administration of all inhalation agents and suxamethonium.
- Hyperventilate the patient with 100% O2 at > 10 l/min via a clean breathing circuit. Do not waste time securing another anaesthetic machine – use an Ambu bag and an O2 cylinder initially.
- Stop surgery if possible. Otherwise maintain anaesthesia with intravenous agents such as propofol until surgery is completed.
- Give dantrolene 2-3 mg/kg. Repeat doses of 1 mg/kg (up to a maximum of 10 mg/kg) should be given until the tachycardia, rise in CO2 production and pyrexia start to subside. Assistance is helpful in mixing dantrolene, which is presented in 20 mg ampoules formulated with 3 g of mannitol. Each vial should be mixed with 60 ml of sterile distilled water. Dantrolene may dissolve faster if several ampoules are emptied into a sterile dish and a large volume of sterile water added. Increasing the temperature of the diluent will also help speed the mixing process.
- Commence active cooling – use cold i.v. fluids and place ice packs on the groin and in the axillae. Consider gastric and bladder lavage. Avoid peripheral vasoconstriction, which will result from excessive use of ice to the skin, as this will prevent heat loss.
Monitor
ECG, SpO2, end-tidal CO2, invasive arterial BP, CVP, core and peripheral temperature, urine output and pH, arterial blood gases, central mixed venous blood gas, potassium, haematocrit, platelets, clotting, creatine kinase (peaks at 12-24 hours).
Treat the effects of MH
- Hypoxaemia and acidosis: 100% O2, hyperventilate, sodium bicarbonate.
- Hyperkalaemia: glucose and insulin, sodium bicarbonate, i.v calcium chloride if significant cardiac effects. During therapy of MH, hypokalaemia frequently results. However, potassium replacement should be undertaken very cautiously, if at all, because potassium may retrigger an MH episode.
- Cardiac arrhythmias: procainamide, Mg, amiodarone, lidocaine. Avoid Ca channel blockers (verapamil can interact with dantrolene to produce hyperkalaemia and myocardial depression).
- Disseminated intravascular coagulation: fresh frozen plasma, cryoprecipitate, platelets.
Subsequent management
- Continue monitoring and symptomatic treatment.
- Be aware of the possibility of recrudescence of MH: as many of 25% patients may experience a relapse within hours of the first episode.
- Assess for renal failure. In order to minimise renal tubular damage by myoglobin, it is important to maintain a diuresis, preferably with alkalinised urine.
Significant muscle weakness and pain may follow MH, resulting from muscle destruction and dantrolene administration; this should be managed symptomatically. Recovery of strength may take weeks to months.
Dantrolene is a hydantoin derivative which acts within the muscle cell to reduce calcium release by the sarcoplasmic reticulum. During an MH episode, dantrolene reduces intracellular calcium levels. It can be dramatically effective when given in time. The average dose required is 3 mg/kg. Occasionally further doses are required during the next 48 hours.
Muscle weakness may persist for 24 hours after dantrolene therapy is discontinued. Other side effects of dantrolene administration are nausea and vomiting, phlebitis, and prolongation of the effects of non-depolarizing muscle relaxants.
MANAGEMENT OF PATIENTS SUSCEPTIBLE TO MH
Patients susceptible to MH should not be denied surgery solely because of MH. The anaesthetist should take time to reassure patients and their families that he or she is familiar with MH and its implications and that appropriate techniques, monitoring and therapy will be instituted as necessary.
Consideration should be given to the use of regional anaesthesia.
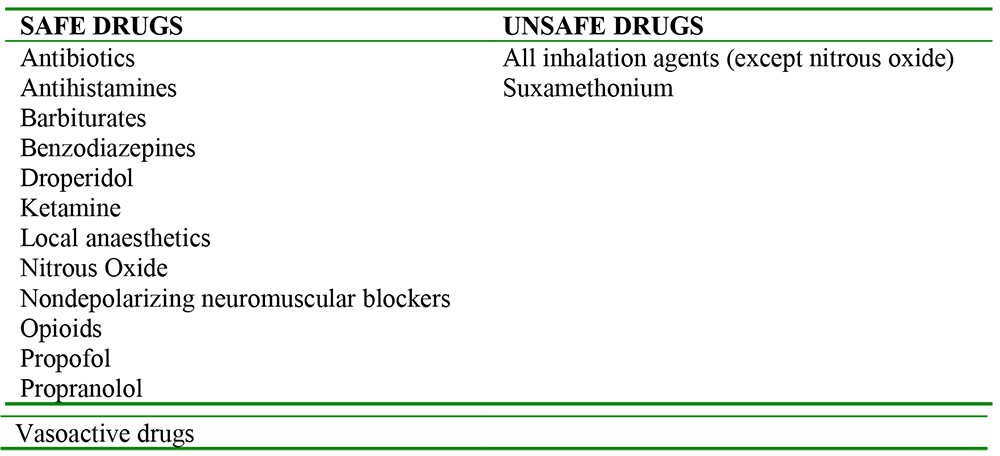
For general anaesthesia an MH ‘safe’ anaesthetic technique is used. i.e. avoiding suxamethonium and all volatile agents. The anaesthetic machine is prepared by removing all vaporizers, changing CO2 absorbent and blowing O2 at 10 l/min for 30 min through both anaesthetic machine and ventilator. A volatile free anaesthetic machine may be kept especially for such patients. New breathing circuits, LMA’s and endotracheal tubes should be used.
Dantrolene should be readily available in the operating room but is not used prophylactically because of its side effects.
End-tidal CO2 should be monitored. Body core temperature should be monitored by nasopharyngeal, rectal or oesophageal routes in all patients.
Obstetrics
Plans for any emergency situation should be made with the anaesthetist during pregnancy.
It is important to anticipate potential airway problems and consider the possibility of awake fibreoptic intubation.
Regional techniques should be encouraged.
If general anaesthesia is required an MH safe technique can be used, using rocuronium to facilitate intubation, and propofol infusion for maintenance of anaesthesia.
The baby of an MH susceptible parent will have a 50% chance of being affected therefore should be treated as potentially MH susceptible.
CONFIRMATION OF DIAGNOSIS
The mainstay of MH diagnosis is in vitro contracture testing (IVCT) performed at specialist centres. As living tissue is required, the patient must attend the centre for a muscle biopsy and subsequent pharmacological testing of fresh muscle strips. Tissue is excised from the vastus medialis muscle, usually under femoral nerve block.
The tests involve measurement of the tension generated in response to separate exposures to halothane and caffeine. Compared with normal individuals, the tension in muscle from MH susceptible patients increases at lower halothane and caffeine concentrations.
Once a case is confirmed, family members are investigated in the same way, starting with first degree relatives. DNA diagnosis for MH has recently been introduced. However, this is on a limited basis because of the complexities of the genetics of MH. It complements the standard IVCT method and cannot be used in isolation at the present time.
CONDITIONS ASSOCIATED WITH MH
The only condition definitely associated with MH is central core disease, an inherited disorder of peripheral muscle weakness. Patients with this condition should be considered as potentially, but not invariably, susceptible to MH and referred for screening. The possible association between MH and heat stroke remains controversial.
MULTIPLE CHOICE ANSWERS
- FFTFT
- TFTTT
- FTFTF
REFERENCES AND FURTHER READING
- Halsall PJ, Hopkins PM. Malignant Hyperthermia British Journal of Anaesthesia CEPD Reviews 2003. Vol 3 Number 1, pages 5-9.
- Guidelines for the management of a Malignant Hyperthermia Crisis. AAGBI 2007 www.aagbi.org/publications/guidelines/docs/malignanthyp07amended.pdf
- Oxford Handbook of Anaesthesia, Second edition, pages 260-264.
- Barash PG, Cullen BF. Clinical Anaesthesia. Pages 530-546.
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/