Intensive Care Medicine

KEY POINTS
- Infective encephalitis is a medical emergency where prompt diagnosis and treatment dramatically improve rates of survival without neurological disability. A low index of suspicion is required.
- Empirical intravenous aciclovir should be administered within 6 hours of the diagnosis being suspected, as it is effective against the most common causative pathogens: herpes simplex virus and varicella zoster virus.
- Patients may be referred to critical care for ongoing management if they need physiological or organ support as a result of organ dysfunction arising from this infective process.
- Critical care also has a role in preventing or limiting secondary brain injury that can arise from this neurological infection.
INTRODUCTION
Infective encephalitis is the acute inflammation of the brain parenchyma as a result of an infectious process. The infection is usually viral but bacterial, fungal, or parasitic infection may be implicated. A minority of patients will develop a severe manifestation of infective encephalitis and may deteriorate and require organ support, often prior to the diagnosis being confirmed. A low index of clinical suspicion and prompt (often empirical) antimicrobial treatment is crucial for the best chance of a recovery without disability. Management in the critical care setting focuses on treating the primary pathology whilst preventing secondary brain injury.
EPIDEMIOLOGY
The incidence of infective encephalitis varies widely according to geographical region. Worldwide, the incidence is estimated to be 1.5 to 7 cases/100,000 inhabitants/y.1 Children, the elderly, and the immunocompromised are more vulnerable to viral encephalitis.
A large proportion of the world’s population has been exposed to herpes simplex virus (HSV), with an 80% to 90% rate of seropositivity and herpes simplex virus encephalitis (HSV/HSE) remains the most commonly implicated pathogen in industrialised nations, accounting for up to 50% of cases where a cause is identified.2,3,4 The majority of HSE is caused by HSV-1, although HSV-2 causes 10% of the infections, usually in the immunocompromised and in neonates.5 It may be caused by primary infection or virus reactivation. It is important to note that 37% to 70% of cases of encephalitis do not have an identified cause2 (Commonly implicated organisms are listed in Table 1.).
Mortality and morbidity rates vary according to causative pathogen. Without antiviral treatment, mortality from HSE is at least 70% with fewer than 3% of survivors returning to baseline function.6 Even with treatment, mortality may still be as high as 30%.6
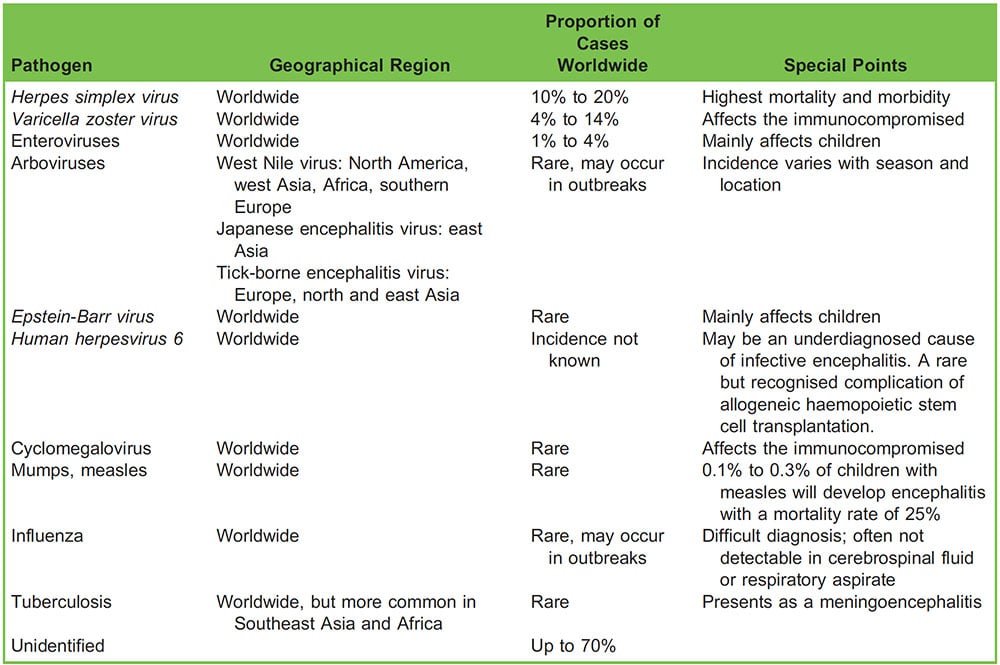
Table 1. Aetiology of infective encephalitis2,8
In survivors, debilitating sequelae can include chronic fatigue, headaches, epilepsy, and problems with balance and coordination.7
PATHOPHYSIOLOGY
Viruses typically access the central nervous system (CNS) via haematogenous spread from the site of an injury (eg, mosquito or animal bite) or mucous membrane infection. In the case of HSV reactivation, it is thought that the virus lies dormant in the trigeminal ganglia and, on reactivation, travels along the olfactory tract to the brain.9 A transient viraemia is followed by seeding within the brain parenchyma, primarily in the grey matter. The infection may affect the brain tissue diffusely or may be limited to a focus. There is perivascular lymphocytic infiltration and disruption of the blood brain barrier which may lead to cerebral oedema with subsequent neurological deterioration.9 Brain shift and tentorial herniation may also occur and are associated with a high mortality.
Viral meningitis is usually mild and self-limiting. In contrast, viral encephalitis is a medical emergency which warrants prompt intervention. There may be initial diagnostic ambiguity as there is overlap in clinical signs and histopathological features (and the two may exist simultaneous as a meningoencephalitis) but, if there is clinical suspicion, viral encephalitis should be treated with antivirals until the diagnosis is excluded.7,9
CLINICAL FEATURES
The classic clinical features of encephalitis are headache, altered mental state, and fever. Pyrexia on hospital admission may be absent in up to 10% of patients with HSE so any history of recent febrile illness in the preceding days and weeks should be elicited.10
Depending on aetiology, other neurological signs may include the following:
- Seizures, generalised or partial
- Behavioural disturbance
- Memory impairment and disorientation
-
Hallucinations of various sensory modality
- Focal signs such as hemiparesis, cranial nerve palsies, dysphasia, and aphasia
Any immunocompromised patient or recent foreign traveller should alert clinicians to the possibility of alternative, atypical causative pathogens.
Differential diagnoses
A wide range of differential diagnoses can make the initial diagnosis of infective encephalitis difficult (Table 2). If infection is thought to be responsible in an immunocompromised patient, the list of causative organisms is even greater.
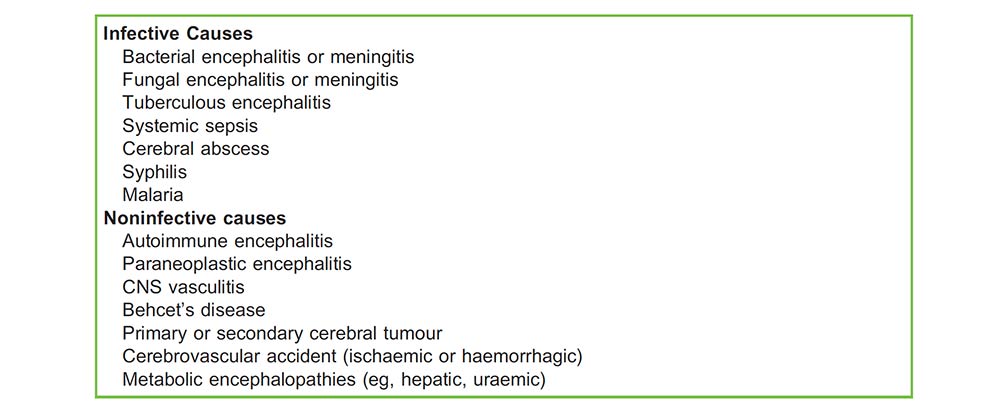
Table 2. Differential diagnoses for infective encephalitis. Please note this list is not exhaustive
Additionally, a particular type of immune-mediated postinfectious encephalitis (also known as acute disseminated encephalomyelitis) can occur following a viral infection.
Similarity in presentation between these differentials may lead to delay in suspecting and treating infective encephalitis.
A more subacute presentation, with a predominance of behavioural changes and extrapyramidal signs involving the face and arms, suggests an autoimmune encephalitis.10
Herpes simplex virus encephalitis
HSE deserves a specific mention as the most common cause of infective encephalitis in the developed world. The infection is usually localised to the inferior frontal and temporal lobes. The immune response causes cytokine release leading to inflammation and apoptosis of neuronal cells.
These patients will typically present with 24 to 48 hours of gradually worsening headache, fever, and confusion. Olfactory or gustatory hallucinations, dysphagia, memory loss, behavioural disturbance, complex partial seizures, and aphasia may also occur.9,11
INVESTIGATION
Presenting features may not point to a clear diagnosis of infective encephalitis so there should be a low threshold for commencing empirical treatment for CNS infection whilst investigations are underway. This index of suspicion should be further lowered for immunocompromised patients, in whom encephalitis may present in a subacute fashion (over weeks to months) with altered mental state but few other clinical features.
The algorithm in Figure 1 gives some guidance as to the management needed in the event that infective encephalitis is suspected and this guides simultaneous investigation and treatment.
After obtaining a comprehensive history, including details such as history of travel, contact with animals, and ascertaining whether the patient is immunosuppressed, the specific key investigations can be divided as follows:
- Neuroimaging
- Cerebrospinal fluid analysis
- Septic screening
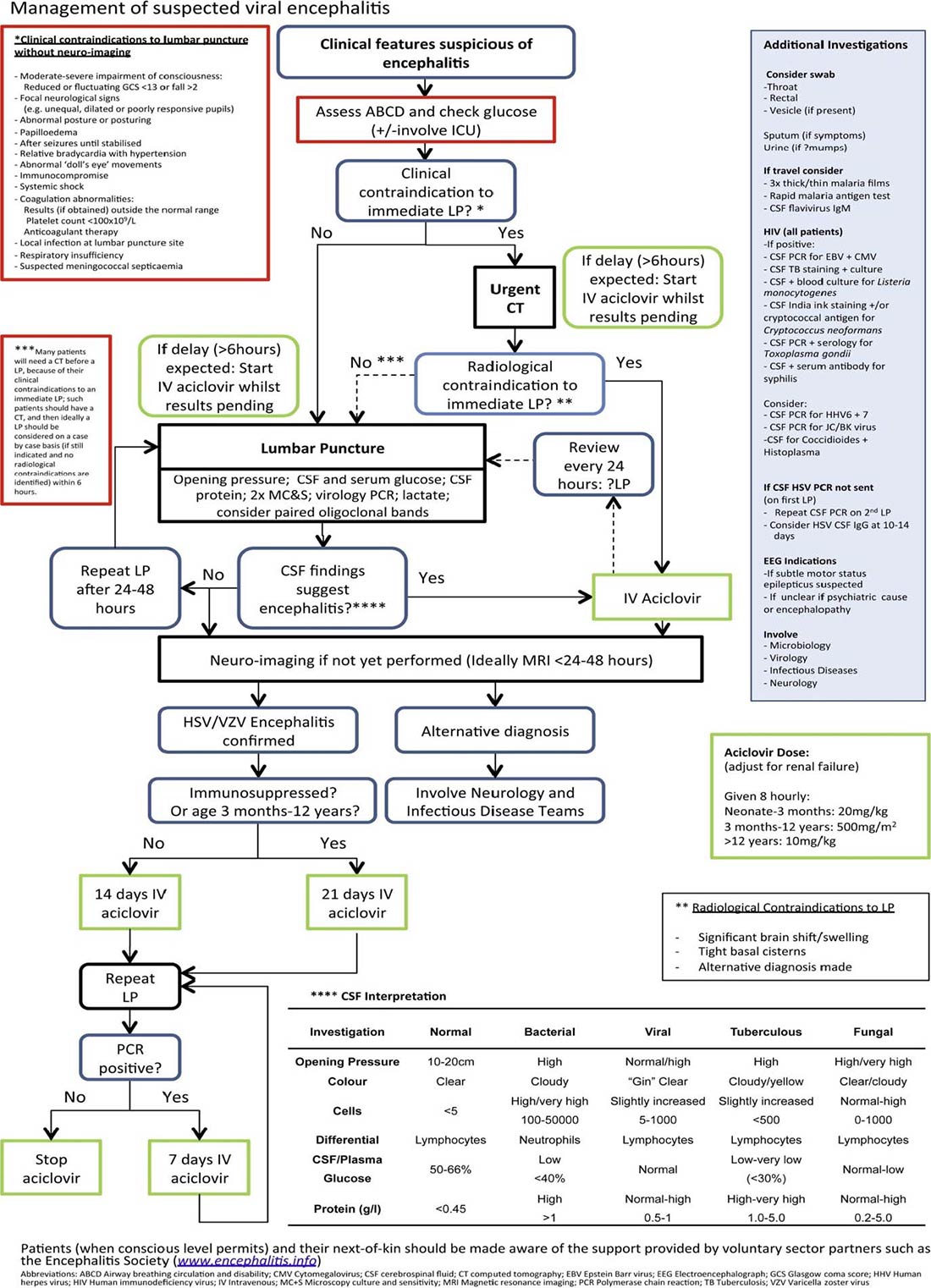
Figure 1. Management algorithm for suspected infective encephalitis (reproduced by permission from Journal of Infection).4
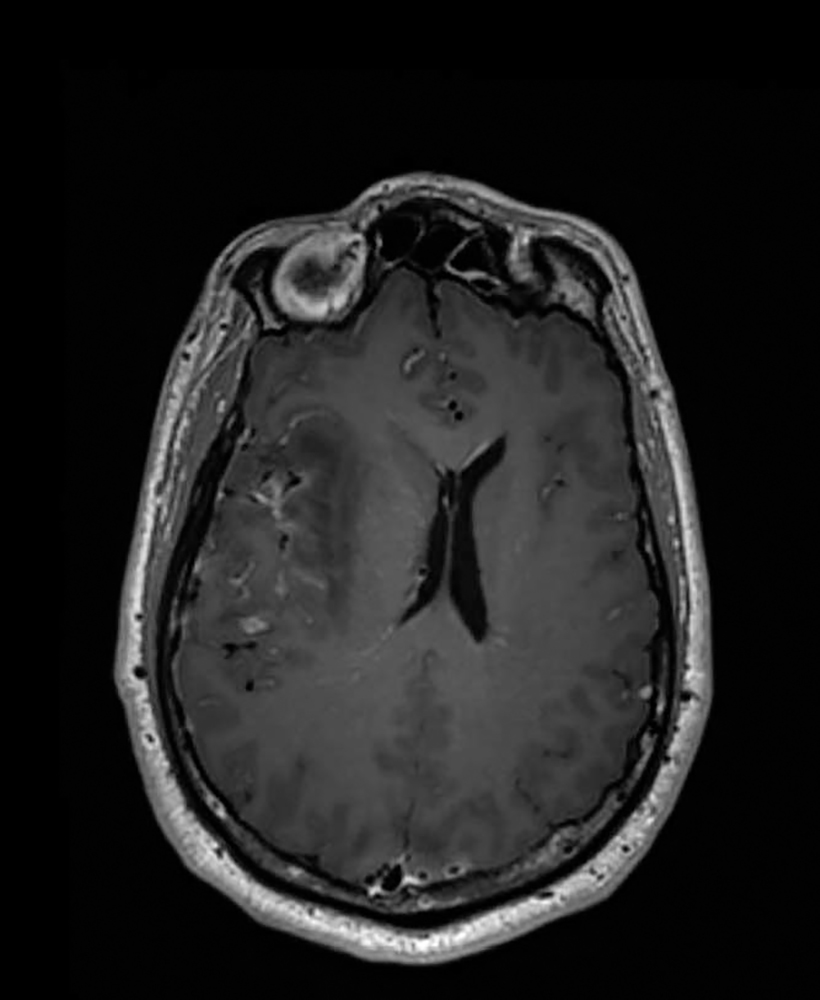
Figure 2. Herpes encephalitis affecting the right temporal lobe, causing oedema and midline shiftImage provided by The Walton Centre NHS Foundation Trust, Liverpool, United Kingdom.
Neuroimaging
A computed tomography (CT) scan of the brain helps to rule out other intracranial pathology and shows radiological features of raised intracranial pressure (which may influence the decision to perform lumbar puncture). A CT scan can be performed quickly and easily in most acute medical centres.
A diffusion-weighted magnetic resonance imaging (MRI) scan can be considered if available (Figure 2). In early encephalitis this is a much more sensitive imaging modality than CT and it can highlight the characteristic pattern of focal changes, the configuration of which depends on the causative pathogen. In HSE, lesions are visible in 90% of cases. It can also prompt an early change in working diagnosis if subtle focal changes are seen, for example, those distinguishing viral encephalitis from postinfective encephalitis.10 Early neuroradiologist input is recommended. The logistical problems of undertaking MRI in patients with altered levels of consciousness and/or those needing a scan out of hours may preclude this investigation in many centres, certainly at an early stage.
Cerebrospinal Fluid Analysis
Lumbar puncture (LP) for cerebral spinal fluid (CSF) analysis should be performed urgently if there are no contraindications (eg, anticoagulation, pathological coagulopathy, or raised intracranial pressure). Intravenous antimicrobials can be commenced prior to LP if these issues cause any delay.
The CSF investigations should include opening pressure, total and differential white cell count, red cell count, glucose, protein, microscopy, and culture and sensitivities for bacteria. Initial results help in the diagnosis of bacterial meningitis but can be less conclusive in viral encephalitis.
Typically, white cell count is 10 to 100 × 106/L and primarily lymphocytic. However, white cell count may be normal or very high (suggesting bacterial meningitis) in early viral encephalitis and may also be difficult to interpret in the immunocompromised. The CSF glucose maybe normal or low, and protein is either mildly elevated or normal.9 If initial LP is nondiagnostic, a second should be performed 24 to 48 hours later.5
A CSF sample should be stored for virological or other future investigations. Viral polymerase chain reaction (PCR) may be negative in early encephalitis but may become positive as the disease progresses, although sensitivity may fall following empirical antiviral therapy.
Initial viral testing should look for HSV-1, HSV-2, varicella zoster virus, and enterovirus. Additional tests in immunocompromised patients should include the following:
- CSF PCR for Epstein-Barr virus and cyclomegalovirus
- CSF acid-fast bacillus staining and culture for Mycobacterium tuberculosis
- CSF and blood culture for Listeria monocytogenes
- India ink staining and/or cryptococcal antigen testing for Cryptococcus neoformans
- Antibody testing—and if positive, CSF PCR for Toxoplasma gondii
- Antibody testing of serum—and if positive, CSF for syphilis5
Septic Screening
Further cultures, such as blood cultures, can also help identify bacterial and fungal infections. Cultures from other sites, guided by clinical examination findings, also need to be taken.
Throat and rectal swabs for enterovirus investigations should be considered and swabs sent from vesicles,if present, in all patients with suspected viral encephalitis.5 When there is a recent or concomitant respiratory tract infection, sputum, bronchial lavage, or nose and throat swabs should be sent. A CSF PCR should be performed for mumps if there is any suspicion of this; parotid gland duct or buccal swabs should also be sent for viral culture or PCR.5
The United Kingdom National Guidelines recommend human immunodeficiency virus testing for all patients with suspected encephalitis irrespective of interpretation of risk factors.5,12
Further Investigation
In patients with suspected encephalitis in whom no diagnosis has been made after the first week, stereotactic brain biopsy should be considered, especially if there are focal abnormalities on imaging. If imaging does not indicate focal abnormalities, an open biopsy from the nondominant frontal lobe may be performed.5
MANAGEMENT
Immediate Management
If empirical antiviral therapy has not already been commenced, it should be started once an LP has been performed.5 This will usually be intravenous aciclovir (10 mg/kg TDS, reduced in patients with renal impairment) which inhibits viral DNA synthesis and is relatively nontoxic.
Immunocompromised patients or those with a history of recent foreign travel should be discussed early with the medical microbiology team as it may be prudent to empirically cover a broader range of pathogens. They should be isolated from the main ward and nursed with barrier precautions including mask, gown, gloves, and strict hand washing.
Broad-spectrum antibiotics appropriate for CNS infection should also be commenced to cover a bacterial cause of encephalitis.
Transfer to a tertiary neurological unit may be appropriate to allow access to regular neurological specialist review and MRI and electroencephalogram (EEG) facilities, as well as when significant diagnostic delay occurs, is inconclusive, or the patient fails to respond to initial treatment.5,10 The Encephalitis Society’s management guideline recommends that patients with suspected acute encephalitis have access to immediate neurological specialist opinion and be managed in a setting where clinical neurological review can be obtained as soon as possible, and definitely within 24 hours of referral.9
Critical Care Management
A proportion of patients with infective encephalitis will deteriorate and need admitting to critical care, typically due to the following:
- Reduced conscious level requiring airway protection
- Respiratory failure secondary to reduced conscious level, aspiration, or atelectasis due to a poliomyelitis-like paralysis2
- Seizures which may be refractory to initial anticonvulsant management and require deep sedation
The principles of management in critical care are to provide organ and physiological support as required and for management to prevent or limit secondary brain injury.
Organ Support
Organ system support is provided using invasive or noninvasive mechanisms as per any other critical illness. Patients with impaired consciousness may need closer observation and nursing care and may also need interventions to protect or maintain their airway. Such patients may also need a degree of respiratory support if their ventilation or oxygenation is compromised by their reduced conscious level. This may include sedation, intubation, and ventilation.
Neuroprotection
Whilst infective encephalitis and its effects may lead to a primary brain injury, critical care aims to reduce or prevent secondary brain injury by adhering to the following neuroprotective parameters with the aim of optimising cerebral perfusion pressure and cerebral oxygenation:
- Maintenance of mean arterial pressure >80 mmHg (or targeted to maintain cerebral perfusion pressure >60 mmHg if intracranial pressure [ICP] is being monitored)
- PO2 >13 kPa
- Normocapnia, PCO2 4.5 to 5.3 kPa
- Normothermia, achieved with antipyretics and/or active cooling if necessary
- Normoglycaemia, achieved with insulin infusion as necessary
- Haemoglobin concentration of at least 80 g/dL, particularly in significant cerebral oedema. Although haemoglobin concentrations as low as 70 g/L are well tolerated in the majority of critical care patients, this degree of anaemia could be considered harmful in brain-injured patients 2,13
- Avoidance of cerebral venous congestion with 30-degree head-up bed tilt and avoidance of endotracheal tube ties
- Avoidance of cerebral oedema associated with hyponatraemia
- Monitoring for, and treatment of, seizure activity (see below)
ICP Monitoring
ICP monitoring is not used routinely but maybe considered if there are clinical or radiological signs of mass effect. Efforts should be made to keep ICP < 20 mmHg through maintenance of the neuroprotective parameters outlined above, with escalated treatment options including deepening sedation, paralysis, and osmotherapy. If ICP remains refractory to medical management, decompressive craniotomy may be considered.
Seizure Management
While seizure activity may be clinically apparent, it should be remembered that encephalitis is one of the most common causes of nonconvulsive status epilepticus.10 Seizures should be controlled with anticonvulsants or, if refractory, infusions of sedatives. There is no evidence to support the use of primary prophylaxis.10,13 The initial recommended drug is intravenous lorazepam administered in increments of 2 mg every 1 to 2 minutes to a maximum cumulative dose of 0.1 mg/kg2.
EEG has a role in determining whether the sedated patient is having seizures (to inform whether existing anticonvulsant therapy is effective or if further or alternative therapy is needed, plus whether a sedation hold is appropriate). It is also helpful in the investigation of the patient failing to wake from sedation. In patients with mildly altered behaviour and diagnostic uncertainty, an EEG can be performed to look for encephalopathic changes.
Role of Corticosteroids
The usefulness of corticosteroids in the treatment of acute infective encephalitis is unclear, although it is theorised that they may modulate the inflammatory processes that cause cellular damage in HSE. In view of the lack of evidence of benefit, corticosteroids may be used under specialist instruction and supervision in selected cases where there is significant vasogenic oedema and mass effect.2,5 In encephalitis with an inflammatory vasculopathy component (eg, varicella zoster virus), there is a better-defined basis for the use of corticosteroids although optimal dosing regimen is unknown.2,5
Continuing Antiviral Treatment
In immunocompetent adult patients with proven HSE, intravenous aciclovir should be continued for 14 days and a repeat LP performed at this time to confirm that the CSF is negative for HSV by PCR. If the CSF is still positive, aciclovir should continue with weekly PCR until it is negative.5
Immunocompromised or paediatric patients with HSE should be treated with intravenous aciclovir for at least 21 days, following which a further CSF PCR for HSV should be sent. Long-term oral aciclovir should be considered until the patient’s CD4 count is > 200 × 106/L.5 Cyclomegalovirus encephalitis should be treated with ganciclovir, foscarnet, or cidofovir.5
In immunocompetent patients with suspected encephalitis who are HSV PCR negative, prophylactic aciclovir can be stopped if
- an alternative diagnosis has been made;
- CSF HSV PCR is negative on 2 occasions 24–48 hours apart, and MRI is not characteristic for HSV encephalitis;
- CSF HSV PCR is negative more than >72 hours after neurological symptom onset, with unaltered consciousness, normal MRI (performed . 72 hours after symptom onset); and
- CSF white cell count is less than 5/mm.3,5
Infective Encephalitis in Children
In industrialised nations, the incidence of infective encephalitis in children is 10.5 to 13.8 per 100,000.8 HSV is the most common pathogen implicated in childhood infective encephalitis. A vaccination history should be elicited as measles infection can be complicated by a concurrent encephalitis.
The general management principles are the same as those outlined for adult patients.
The dose of intravenous aciclovir for the initial treatment of suspected or confirmed HSE in children should be as follows:
- 3 months to 12 years: 500 mg/m2 every 8 hours
- >12 years: 10 mg/kg every 8 hours5
Children with suspected encephalitis should have the additional involvement of paediatricians, paediatric neuroradiologists and, where indicated, paediatric neurosurgeons.
SUMMARY
Intensive care clinicians should maintain a low index of suspicion regarding the diagnosis of infective encephalitis, as delays in treatment are associated with increased mortality and long-term neurological sequelae in survivors. Initial misdiagnosis as encephalopathy is a common reason for such a delay. Prompt antimicrobial treatment, early involvement of neurologists, and treatment strategies to manage and prevent complications are keys to achieving the best possible outcomes in these patients.
REFERENCES
- Boucher A, Hermann JL, Morand P et al, Epidemiology of infectious encephalitis causes in 2016, Me´ d Maladies Infect. 2017;47(3):221–235.
- Kramer AH. Viral encephalitis in the ICU. Crit Care Clin. 2013;29(3):621-649.
- Whitley RJ. Herpes simplex encephalitis: adolescents and adults. Antiviral Res. 2006;71:141-148.
- Steiner I, Kennedy PG, Pachner AR. The neurotropic herpes viruses: herpes simplex and varicella zoster. Lancet Neurol 2007;6(11):1015–28.
- Solomon T, Michael BD, Smith PE et al, Management of suspected viral encephalitis in adults; Association of British Neurologists and British Infection Association National Guidelines, Journal of Infection 2012; 64(4):347–73.
- Kennedy PGE, Chaudhuri A. Herpes Simplex Encephalitis. Journal of Neurology, Neurosurgery & Psychiatry, 2002;73(3):237–238.
- Ellington A, Encephalitis Society. Physical difficulties after encephalitis. https://www.encephalitis.info/physical-difficultiesafter- encephalitis. (accessed on 30/10/2019).
- Jmor F, Emsley HCA, Fischer M et al. The incidence of acute encephalitis syndrome in Western industrialised and tropical countries. Virol J 2008;5:134. https://doi:10.1186/1743-422X-5-134
- Ropper AH, Gress DR, Diringer MN et al. Neurological and Neurosurgical Intensive Care, 4th edition. Philadelphia, Lippincott, Williams and Wilkins 2004.
- Stoeter DJ, Michael BD, Solomon T et al. Managing acute central nervous system infections in the UK adult intensive care unit. J Intensive Care Soc 2015;16(4):330–338.
- Michael BD, and Solomon T. Seizures and encephalitis: clinical features, management and potential pathophysiologic mechanisms. Epilepsia 2012; 53(s4): 63–71.
- British HIV Association. UK National Guidelines for HIV Testing 2008. https://www.bhiva.org/HIV testing-guidelines. (accessed on 30/10/2019)
- Kramer AH, Zygun DA. Anemia and red blood cell transfusion in neurocritical care. Crit Care 2009;13:R89.
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/