General Topics

QUESTIONS
Before continuing, try to answer the following questions. The answers can be found at the end of the article, together with an explanation.
- Which of the following is true? Massive haemoptysis:
- Usually originates in the pulmonary circulation
- Can arise due to bronchopulmonary fistulae
- In bronchiectasis is always due to infection
- Is generally amenable to surgery when due to diffuse alveolitis
- In aspergillosis is rare
- Which of the following is true? Massive haemoptysis:
- Intubation is preferably with a double-lumen tube in the first instance
- A single lumen tube is preferred if the bleeding is known to be right-sided
- Rigid bronchoscopy may be life-saving
- Flexible bronchoscopy can be carried out through a rigid bronchoscope
- Iced saline lavage has been shown to be effective
- With regard to vasculitis:
- Wegener’s granulomatosis is associated with p-ANCA autoantibody
- Is associated with characteristic nasal signs and symptoms
- Tends not to cause systemic symptoms other than related to renal and respiratory symptoms
- Is associated with the nephrotic syndrome
- Responds well to therapy with steroids
- Angiography and embolisation in massive haemoptysis:
- Is a definitive therapy in the emergency situation
- Can avert the need for thoracic surgery
- Is possible in an unstable patient
- May be repeated
- Can cause stroke or paraplegia
- Concerning tracheoinnominate fistula:
- The outcome is generally good
- May occur in tall thin individuals even with a correctly-sited tracheostomy tube.
- Usually occurs without warning
- The tracheostomy tube should be partially withdrawn and the cuff inflated
- Urgent cardiothoracic surgery is indicated after holding measures
INTRODUCTION
Haemoptysis is a common symptom with many potential causes. Massive haemoptysis accounts for roughly 5% of the total seen. There is no agreed definition of massive haemoptysis in terms of volume of blood, but research articles attach this descriptor to volumes ranging from 100ml to 1000ml within 24 hours. In practice, life-threatening haemoptysis occurs with any volume of blood that could obstruct the airway or cause significant haemodynamic compromise and hence a “magnitude of effect” definition is preferred, i.e. life threatening haemoptysis is that which causes impairment of gas exchange, haemodynamic instability or is greater than 100 mls in 24 hours. (This last is the minimum volume reported to be life-threatening due to asphyxia).
Mortality from a large bleed may be as high as 80% therefore urgent intervention is required to stabilize the patient.
Further investigations can then be performed to establish the cause with the aim of providing targeted treatment.
ANATOMY AND PATHOPHYSIOLOGY
In 90% of cases of massive haemoptysis the source is the bronchial circulation, which supplies the bronchial tree at systemic pressure, as distinct from the low pressure pulmonary circulation.
Several common anatomical variations in the bronchial arterial supply have been described. However, in about 40% of people, two left bronchial arteries, (superior and inferior) arise from the thoracic aorta, whereas the right (single) bronchial artery can arise from either the thoracic aorta, a right posterior intercostal artery or the left superior bronchial artery. Abnormal anatomy can predispose to bleeding, as discussed below.
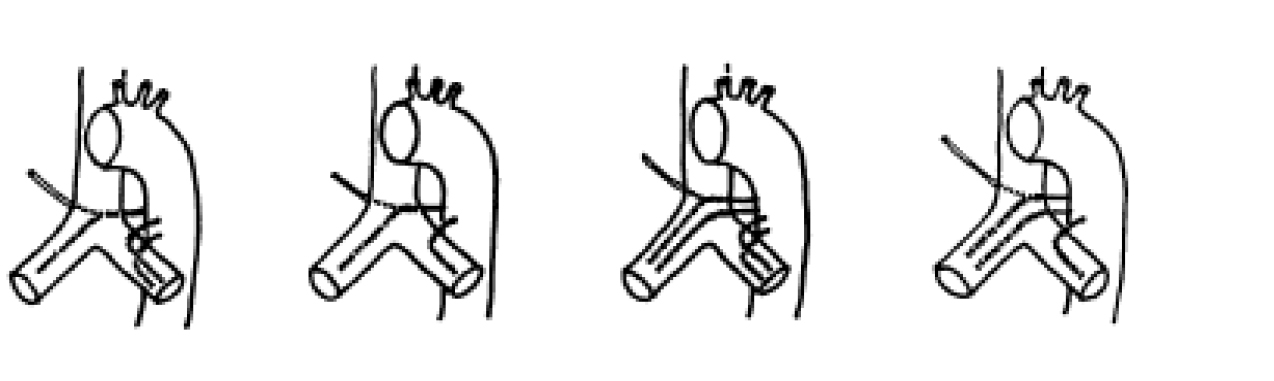
Figure 1. The 4 commonest arrangements of the bronchial artery origins. Reproduced with permission from Yoon et al: Radiographics. 2002;22:6
Chronic inflammatory conditions
In chronic inflammation, angiogenic growth factors induce hypertrophy of the bronchial vessels and new vessel formation. The new vessels are fragile, thin-walled and liable to rupture as they are at systemic pressure.
Bronchial-systemic connections
Abnormal congenital connections between bronchial, internal mammary, intercostal, subclavian and pulmonary arteries can give rise to bleeding or predispose to it in inflammatory conditions.
Pulmonary Arteriovenous Malformations (AVM)
Pulmonary AVMs are developmental abnormalities causing persistent communication between arteries and veins within the lung therefore bypassing the pulmonary capillary bed. 95% derive their blood supply from branches of the pulmonary artery but others have a systemic supply from the aorta, subclavian, internal mammary, bronchial and intercostals arteries. In the case of a systemic arterial supply there is no right to left shunt and therefore no arterial hypoxaemia, which may be demonstrated with large shunts. AVMs may be detected on chest x-ray as one or more lobulated opacities, often in the periphery of the lower lung fields but CT is required for clear identification of lesions.
Congenital absence of a pulmonary artery
Isolated unilateral pulmonary artery agenesis is a rare condition that may not present until adulthood. Published case reports show a variety of presenting symptoms. Haemoptysis is a feature in one fifth, but more frequently recurrent infections (37%) and dyspnoea or limitation of exercise tolerance (40%) are reported. Diagnosis can be aided by ventilation-perfusion scintigraphy, with angiography, and CT and MRI imaging to confirm the extent of the collateral systemic circulation, from which massive haemoptysis can arise.
Other causes of massive haemoptysis can be subclassified as follows, according to the site of pathology:
- Blood vessels
- Vasculitis and pulmonary-renal syndromes
- Bronchial tree
- Bronchiectasis
- Parenchymal cavitatory lung disease
- Lung abscess
- Mycetoma
- Lung malignancy
- Miscellaneous
- Drugs
INITIAL MANAGEMENT
The first priority is to stabilize the patient, which, as with any emergency presentation involves establishing large bore intravenous access, giving IV fluids and transfusing blood products as required, along with correction of any coagulopathy. The cause of bleeding must be clearly established, excluding an upper respiratory tract or gastrointestinal source. Dark blood and the presence of nausea and vomiting suggest a GI source; frothy blood, gurgling in the chest appreciated by the patient, and absence of nausea suggest a chest cause; epistaxis is generally easy to diagnose on examination.
The patient should be transferred to a high dependency or intensive care unit. If the affected lung can be identified the patient should be nursed with this lung down to avoid aspiration into the contralateral lung. Nebulised adrenaline can be used (5-10ml of 1in 10,000 adrenaline) as a temporising measure during transfer.
Airway management
If the patient is at risk of asphyxiation due to the volume of blood then induction of anaesthesia and intubation is required.
Option 1.
Pragmatically, in most instances, this will be with a single lumen tube at first, which should be as large as possible. Suction and bronchial toilet should be carried out immediately. A chest x-ray can be helpful at his stage if not already done and the patient is stable enough to permit it. The flexible bronchoscope can be used to suction clot and instil topical vasoconstrictors or haemostatic agents (see below). Afterwards, the SLT can be advanced under fibreoptic control into the unaffected main bronchus, or if available, a bronchial blocker left inflated in the bleeding side. This allows the endotracheal tube to be withdrawn to the trachea. The flexible bronchoscope, due to its narrow lumen, is less efficient at removing thick clot compared to a rigid bronchoscope.
Option 2
Double lumen tubes are difficult to insert with brisk bleeding and are not large enough to permit passage of a flexible bronchoscope with suction capability. They may buy time until definitive management can proceed or arrest bleeding through tamponade. Left sided tubes are preferable, unless expert, as occlusion of the right main bronchus is difficult to avoid in an emergency situation.
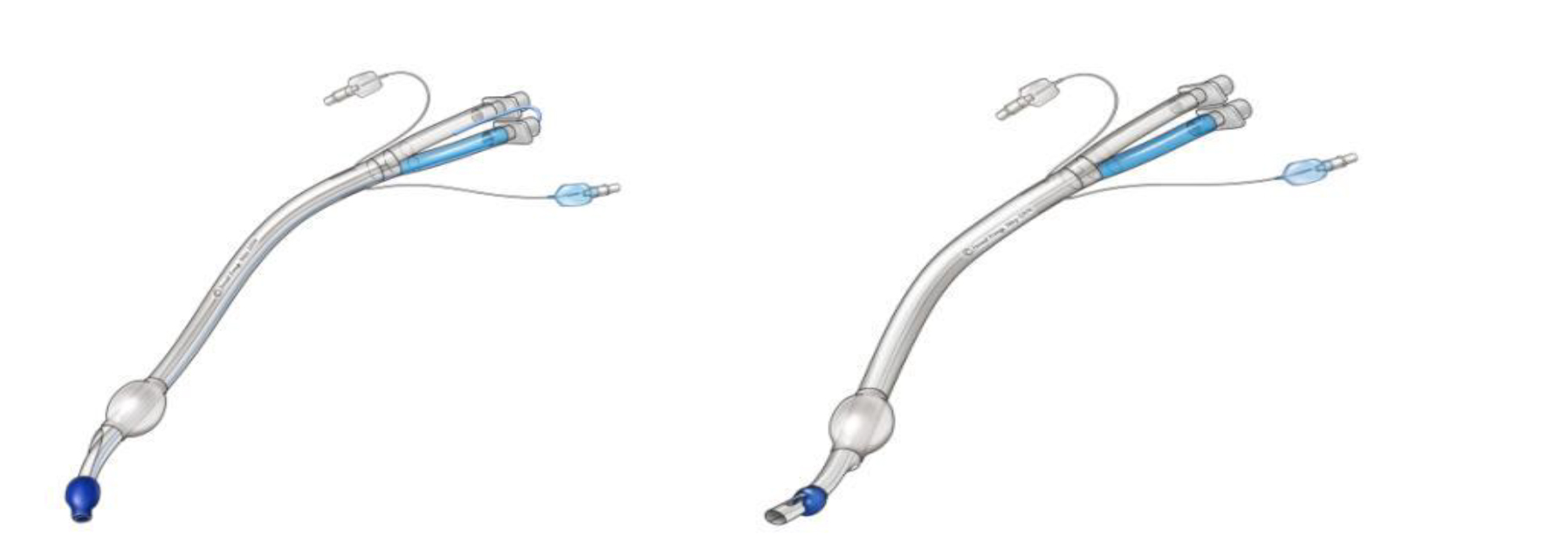
Figure 2. Left and right-sided double lumen endobronchial tubes.
The orifice for ventilating the RUL bronchus can be difficult to align correctly, especially in a bleeding emergency.
Reproduced from www.aic.cuhk.edu.hk © Janet Fong
Option 3
If adequate oxygenation cannot be achieved by this means or brisk bleeding is ongoing despite suction, then transfer to theatre for rigid bronchoscopy allowing suction of clots and easier passage of surgical instruments is probably the preferred choice. The rigid bronchoscopic approach requires anaesthesia with either TIVA or intermittent oxygenation via a Manujet or the use of an anaesthesia circuit attached to the bronchoscope. Rigid bronchoscopy can utilise therapy as described below. A major disadvantage of the rigid bronchoscope is that its reach is to the level of the main bronchi only and more distal bleeding may not be best managed.
Control of bleeding
Multiple approaches have been described. These can be divided into:
Tamponade
Either the bronchial balloon of a DLT or a 4 F 100cm Fogarty embolectomy catheter or Arndt endobronchial blocker, inserted via a single lumen tube, can be used for tamponade and left inflated for 24 hours before deflation and observation.
There is a theoretical risk of mucosal ischaemia with this approach.
Lavage
Lavage with saline cooled in ice in 50 ml aliquots down the bronchoscope with volumes up to 1 litre is well described, and can arrest bleeding due to vasoconstriction.
Adrenaline or other vasoconstrictor
Adrenaline 1:20,000 can be instilled into the bleeding segment until bleeding stops.
Topical coagulants
Thrombin and fibrinogen concentrates have been topically instilled, with anecdotal success.
Laser, diathermy, or cryocautery
These are possible through a rigid bronchoscope and can be applied to, for example, a bleeding endobronchial tumour.
Further investigation-CT
CT can be useful for delineation of abnormal anatomy. It can reliably identify bleeding sites in over 60% of cases. The findings, together with those from fibreoptic bronchoscopy, are useful in planning which vessels to cannulate first in angiography. Diagnostic findings suggestive of bronchiectasis, tuberculosis, bronchial neoplasms and aspergillosis may also be detected.
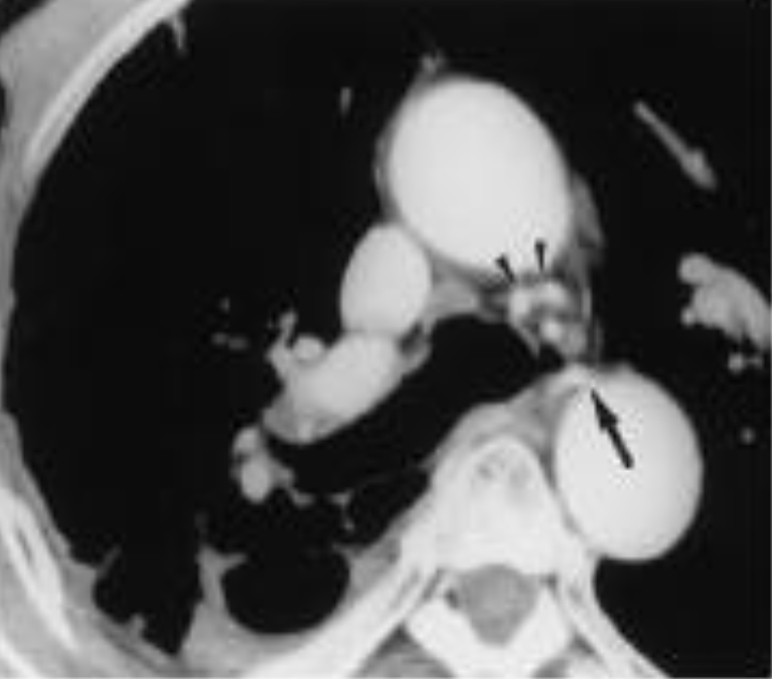
Figure 3. CT close-up showing pathological right and hypertrophic left bronchial arteries Reproduced with permission from Yoon et al: Radiographics. 22;6, 2002
Bronchial angiography and embolisation
Angiography and embolisation has a high success rate in expert hands in arresting haemoptysis. It can be a good alternative to surgery, especially in those who are unfit, or it can stabilise a patient as a bridge to surgery. The high success rate is tempered by a significant incidence of re-bleeding within months. Descending aortography is often performed first, looking for abnormal bronchial vessels; abnormal areas seen on CT can be targeted initially. The major problems can be due to collaterals from arteries other than the bronchial, e.g intercostal, internal mammary or subclavian. Embolic material can comprise polyvinyl alcohol, trisacryl gelatin, microcoils or others.
Embolisation of the anterior spinal artery causing paraplegia is a rare but devastating complication as, rarely, the ASA arises from the bronchial supply. Using embolic material larger than 250-300 micrometers in diameter is said to be protective against it entering small vessels.
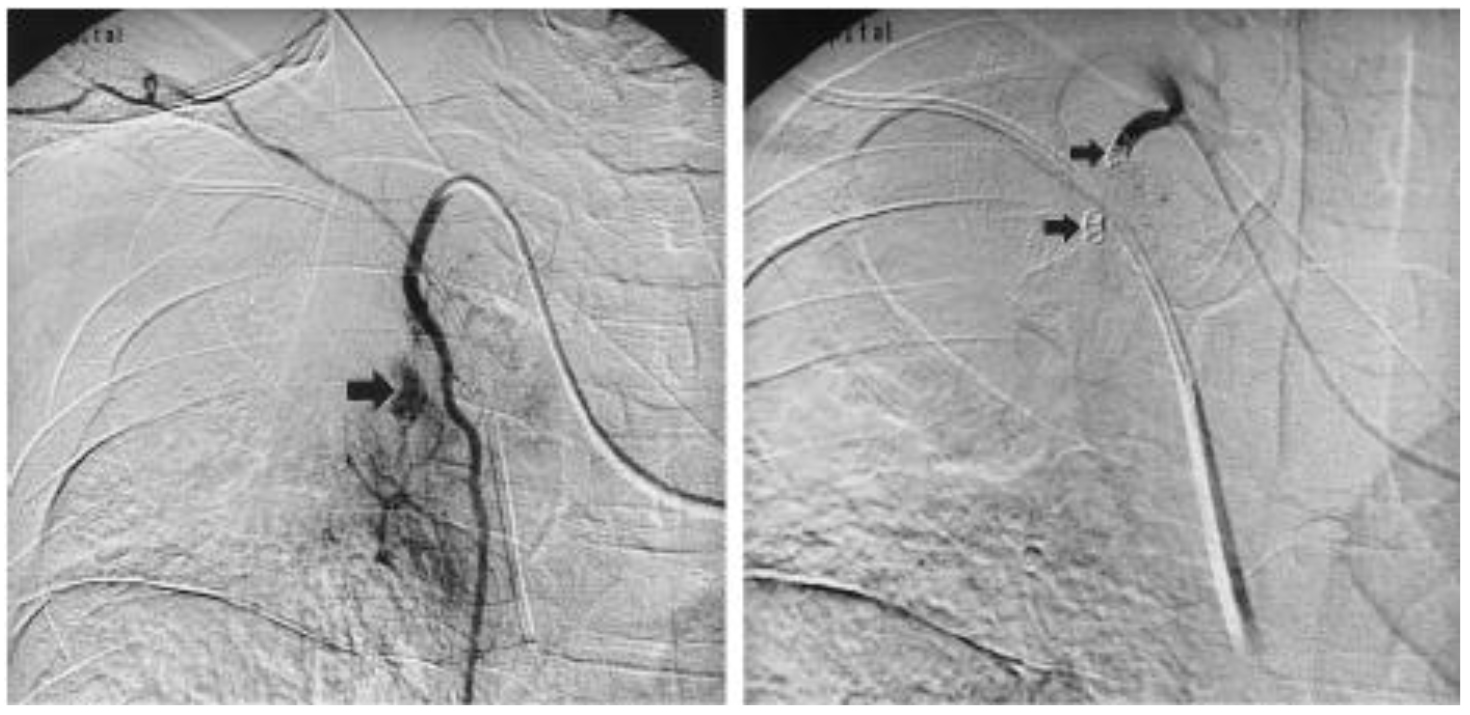
Figure 4. Pre- and post- embolisation angiogram appearances (a) Selective right internal mammary angiogram shows small branches supplying a hypervascular staining lesion in the right upper lobe, as well as a pseudoaneurysm (arrow). (b) After deposition of two coils (arrows) and additional polyvinyl alcohol particles, neither is visualized. Reproduced with permission from Yoon et al: Radiographics. 22;6, 2002
Role of Surgery
Patients with unilateral difficult to control bleeding should be seen by a thoracic surgeon, and a decision about suitability for surgery made early. The usual preoperative workup is not possible in this cohort. Patient selection is key to good outcome – severe underlying lung disease, diffuse alveolar haemorrhage, bilateral haemorrhage or active tuberculosis are relative contraindications.
CAUSES OF HAEMOPTYSIS
Cavitating lung disease
Tuberculosis
The commonest cause worldwide, TB can cause haemoptysis by erosion of primary cavities or cavities secondarily infected with Aspergillus into bronchial blood vessels or through vessel changes consequent on post-tubercular bronchiectasis.
Lung abscess
Most commonly occurring after aspiration, lung abscesses are usually caused by anaerobic bacteria, particularly gram negative bacilli such as Bacteroides. However, this is dependent on whether the infection was community or hospital acquired and mixed aerobic and anaerobic infection is very common. Blood and sputum should be obtained for culture to guide appropriate antibiotic therapy. Bronchoscopy may be useful to obtain samples but also to exclude a proximal obstructing lesion such as a tumour or foreign body. In addition to usual bacteria, lung abscesses may be caused by mycobacteria and fungi so specific cultures should be requested on samples obtained.
Mycetoma
A mycetoma is a mass of fungal material growing in a cavity and is usually caused by Aspergillus fumigatus (and therefore referred to as an aspergilloma). Severe haemorrhage occurs in up to one quarter of patients and causes death in about 5%. Severe haemoptysis is usually preceded by recurrent episodes of smaller volume haemoptysis. Surgical resection is high risk due to the likelihood of haemorrhage intraoperatively and the chance of causing bronchopleural fistulae. Bronchial artery embolisation may be a viable alternative in massive haemoptysis or pre-operatively to reduce the bleeding risk.
Lung malignancy
Lung carcinomas may cavitate due to central necrosis, typically producing a cavity with a wall thickness of 5mm or more. The differential diagnosis of similar size cavities includes lung abscesses, pulmonary infarcts and rarely rheumatoid nodules and Wegener’s granulomatosis. They are most commonly of squamous cell origin but can occur in other tumour types.
Bronchiectasis
Bronchiectasis, a permanent dilatation of one or more bronchi, is most often acquired as a result of childhood infection (pertussis, measles, TB) but is also associated with congenital conditions such as cystic fibrosis and primary ciliary dyskinesia. Inherited or acquired immunodeficiency syndromes, such as hypogammaglobulinaemia, are also associated. Bronchial arteries can become tortuous and hyperplastic in association with bronchiectasis and as they are under systemic pressure can be a source of massive haemoptysis. Bleeding can occur spontaneously or be triggered by infection.
Vasculitis
Pulmonary-renal syndromes are defined by the presence of diffuse alveolar haemorrhage and glomerulonephritis. The underlying pulmonary pathology is small vessel vasculitis, affecting arterioles, venules and capillaries leading to disruption of the alveolar-capillary membrane and causing leakage of blood into alveoli. Within the kidneys there is usually a focal, proliferative glomerulonephritis associated with extensive crescent formation. Diffuse alveolar haemorrhage can present with massive haemoptysis, although in other cases it presents with diffuse opacification on chest x-ray, anaemia and detection of an increased carbon monoxide transfer factor (DLCO) on pulmonary function tests. Pulmonary-renal syndromes require urgent treatment and have been associated with a high early mortality of 25-50%. It is therefore essential to establish the diagnosis as soon as possible to allow treatment to be commenced.
Goodpasture’s Syndrome
This is a rapidly progressive glomerulonephritis associated with diffuse alveolar haemorrhage and the presence of antibodies directed against the glomerular basement membrane (Anti-GBM antibodies). These can be seen on immunofluorescence of a renal biopsy sample as IgG deposition along glomerular capillaries. The binding site for the antibody is present on the alpha3 chain of type IV collagen and is found in the basement membranes of renal glomeruli, renal tubules, alveoli, the choroid plexus, retinal capillaries and Bruch’s membrane. Treatment is immunosuppression to control the immune response and in some cases plasma exchange to remove circulating antibodies.
ANCA-associated vasculitides
Wegener’s Granulomatosis is associated with the presence of cANCA (cytoplasmic antineutrophil cytoplasm antibodies) targeted against proteinase 3 (PR3). Renal biopsy typically shows a focal necrotising glomerulonephritis. Necrotising inflammation is also found within the upper and lower respiratory tracts leading to ENT symptoms such as sinusitis, otitis media, epistaxis and saddle nose deformity alongside dyspnoea, cough and haemoptysis. The systemic vasculitis leads to fever, arthralgia, malaise, anorexia and weight loss.
Microscopic polyangiitis is associated with pANCA (perinuclear) antibodies to the myeloperoxidase antigen. The small vessel vasculitis leads to skin and joint symptoms in addition to the pulmonary-renal syndrome.
Rheumatological autoimmune disease
Systemic lupus erythematosus and systemic sclerosis have been associated with the pulmonary-renal syndrome. The vasculitis is caused by immune complex deposition in the pulmonary and renal vessels.
Treatment of pulmonary vasculitis
Management is with pulsed IV methylprednisolone in the majority of cases or high dose oral prednisolone in more stable patients. This is given over approximately 3-5 days then tapered to 1mg/kg prednisolone for about one month before weaning slowly and monitoring for signs of recurrence. Additional immunosuppressive therapy may also be required (e.g cyclophosphamide), depending on the severity and response to prednisolone treatment. After induction of remission, maintenance therapy usually includes azathioprine or methotrexate. Prophylaxis against pneumocystis jiroveci pneumonia should be given when a second immunosuppressive drug is used in initial therapy. This is usually co-trimoxazole, or if there is a contraindication to this, Atovaquone as an alternative. It should be continued until the patient is well established on maintenance therapy with a CD4 positive T-cell count of >300 per microlitre.
Plasma exchange is used for diffuse alveolar haemorrhage associated with Goodpasture’s disease to speed clearance of antibodies, alongside immunosuppressive therapy (glucocorticoids and cyclophosphamide) to reduce further anti-GBM production. The role of intravenous immunoglobulin (IVIg) infusion is not clear.
On initial presentation it will not be clear as to the cause of the pulmonary infiltrates, which may resemble pneumonia. Therefore all patients should be treated with broad-spectrum antibiotic therapy.
Tracheo-innominate fistula
This is a rare cause of haemoptysis in critical care. It is almost invariably fatal without prompt treatment and surgery. The innominate (or brachiocephalic) artery is the first branch of the aortic arch which divides soon after its origin into the right subclavian and right common carotid arteries. It lies posterior to the 6th to 9th rings of the trachea with a rather variable position. It is vulnerable to pressure exerted from within the tracheal lumen causes by the balloon of a low-lying tracheostomy, which can cause erosion and pressure necrosis of the posterior tracheal and vessel walls. Tall thin patients can have unusually high-lying arteries which can make even tracheostomy tubes inserted at appropriately higher levels prone to this complication. Local sepsis, steroid or radiation treatment, malnutrition, rigid and “right-angled” tubes can also predispose to fistula formation.
Bleeding occurs any time from a week to a few months after insertion of the tracheostomy. A torrential bleed is often preceded by a “sentinel bleed” from or around the tracheostomy tube. Management involves, in addition to appropriate circulatory support, “buying time” by:
- (a) Initial overinflation of the tracheostomy balloon, which may arrest bleeding by compressing the artery against the manubrium sterni.
- (b) Controlling distal airway soiling by inserting a cuffed endotracheal tube through the larynx distal to the tracheostomy stoma and removing the tracheostomy (or a small ETT could be inserted through the tracheostomy).
- (c) Digital insertion through the stoma of the removed tracheostomy, and manual compression of the innominate artery artery against the posterior surface of the manubrium.
Urgent surgical exploration, debridement and ligation of the artery is necessary through a sternotomy incision. Prevention of this dreaded complication is assisted by bronchoscopic control during percutaneous tracheostomy and placement between the first and second or second and third rings. Monitoring cuff pressures, as is now routine on most units, is also helpful. A high index of suspicion for sentinel bleeds may direct early management including bronchoscopy.
Miscellaneous
Drug causes
Multiple drugs can cause pulmonary haemorrhage. Propylthiouracil and hydralazine have been associated with an ANCA positive vasculitis. Pulmonary-renal syndrome has been seen with penicillamine and carbimazole. Diffuse alveolar haemorrhage has been reported with amiodarone, nitrofurantoin, methotrexate and phenytoin as well as Cocaine use.
Recurrent episodes of diffuse alveolar haemorrhage may occur without a specific cause being established despite appropriate investigation. This is termed idiopathic pulmonary haemosiderosis. Lung biopsy will show pulmonary haemorrhage without evidence of immune complex deposition or vasculitis.
INVESTIGATION OF THE UNDERLYING CAUSE OF MASSIVE HAEMOPTYSIS
Even after appropriate investigation the aetiology of haemoptysis may not be determined in up to 25% of cases. The most common causes of massive haemoptysis are chronic inflammatory conditions and lung malignancies. After stabilising an acutely unwell patient as described above, investigations to establish the cause of the haemoptysis can begin. If not performed already, baseline blood tests including full blood count, urea and electrolytes, clotting screen and a group and save sample for blood transfusion should be taken. These are helpful to establish the extent of anaemia and need for transfusion, to evaluate the degree of renal impairment and to detect any clotting abnormality that would require correction.
A chest x-ray may show the distribution of pulmonary haemorrhage, a lung cavity, abscess or tumour, or signs of bronchiectasis such as peribronchial thickening. There may also be evidence of co-existent pneumonia, which could have triggered a vasculitis or caused an exacerbation of bronchiectasis. Blood and sputum samples should be taken for culture.
Further imaging with CT is valuable, provided the patient is stable enough, to further clarify the nature of any chest x-ray abnormality and may even detect vascular malformations.
More specific blood tests should include anti-GBM antibodies, ANCA and anti-nuclear antibodies if vasculitis is a possibility.
Urinalysis is helpful in detecting renal involvement, which in vasculitis would show haematuria, proteinuria and red cell casts. Pulmonary function tests are unlikely to be possible in an acutely unwell patient but may show an increased DLCO in pulmonary haemorrhage.
More invasive tests should then be considered. A bronchoscopy will already have been performed in the course of urgent management to stabilise the patient and this may still need to be repeated to allow a more detailed examination of the bronchial tree and for relevant samples to be taken. Bronchoscopy may reveal an obvious cause such as an endobronchial tumour. If the bronchial tree appears grossly normal, broncho-alveolar lavage may be helpful to exclude infective causes or may suggest vasculitis if a progressively more blood-stained aspirate is obtained. Samples should be sent for routine culture, mycobacterial and fungal culture and cytology. Renal or lung biopsy will be useful in the evaluation of possible vasculitis but often patients are not stable enough to allow this and this should not delay commencing treatment if a pulmonary-renal syndrome is suspected
ANSWERS TO QUESTIONS
- F T F F F
- F T T T T
- F (c-ANCA) T F F T (but additional immunosuppression or plasma exchange may be needed)
- T (but rebleeding is common) T T T T (if the vertebral or anterior spinal arteries respectively are inadvertently embolised)
- F T F (a herald or sentinel bleed often precedes) F T
REFERENCES AND FURTHER READING
- Papiris SA, Manali ED, Kalomenidis I, Kapotsis GE, Karakatsani A, Roussos C. Bench-to-bedside review: Pulmonary-renal syndromes – an update for the intensivist; Critical Care 2007;11:213
- Lordan JL, Gascoigne A, Corris PA. The pulmonary physician in Critical Care. Illustrative case 7: Assessment and management of massive haemoptysis; Thorax 2003;58:814-819
- Yoon Woung, Kim Jae Kyu et al. Bronchial and nonbronchial systemic artery embolization for life-threatening hemoptysis: a comprehensive review. Radiographics 2002;22:1395-1409
- Grant, C.A. et. Al. Tracheo-innominate artery fistula after percutaneous tracheostomy: three case reports and a clinical review. BJA 2006; 96: 1127-31.
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/