General Topics

Introduction
Anaesthetists are involved in resuscitation in the Emergency Department (ED), the operating room, the intensive care unit and during pain consultations.
The highest death rates are in children younger than 5 years and adults older than 65 years. Most injuries occur in the home, particularly children with scalds and adults injured by direct flame burns.
Only 37% of burned patients return to their same job. The percentage total body surface area burn (TBSA) is the best predictor of time off work for adults.
The factors that decrease wound infection rate and mortality are resuscitation without fluid overload, securing the airway, and prompt debridement and grafting of the burn.
Assessment and Treatment in the ED
Airway Assessment
Always remember to stabilise the cervical spine if there is any suggestion of cervical injury.
Features of an airway burn may include upper airway swelling, inhalational injury and carbon monoxide poisoning.
Tracheal intubation may be required if the patient is unable to protect their airway.
Clinical features suggesting that tracheal intubation is likely to be needed are:
- a score of 8 or less on the Glasgow Coma Scale (impaired mental status) facial burns
- singeing of facial or nasal hair
- oropharyngeal carbon deposits
- carbonaceous sputum
- hoarseness
- stridor
- wheezing
- burns greater than 30% TBSA carboxyhaemoglobin levels greater than 10%
In burns >30% TBSA there is potential for swelling of the soft tissues of the oropharynx and subcutaneous oedema in the face and neck. If you are unsure whether to intubate or if transfer to another centre is planned, have a low threshold for intubating early, before oedema makes tracheal intubation difficult or impossible.
Intubation
Difficult bag-mask ventilation, laryngoscopy and intubation should be anticipated and where possible should be dealt with by an experienced anaesthetist.
Massive upper airway oedema may preclude the use of the laryngeal mask airway or combitube.
Awake intubation may be the safest approach.
Emergency cricothyroidotomy or tracheostomy is indicated in failed intubation or where an impossible intubation is predicted. These are not ideal since infection may spread to surrounding skin, but equipment should be available.
When an endotracheal tube is placed it should be uncut and its position regularly checked during the development of maximal oedema over a 12-24 hour period.
Breathing
Inhalation injury is a very significant contributor to mortality. Lung damage occurs from direct inhalation injury:
- Smoke inhalation is usually only hot enough to injure the larynx and upper trachea.
- Chemical irritation or toxic inhalation affects the small airways causing severe bronchospasm.
- Steam has a high enough heat content to injure alveoli directly, resulting in ARDS (acute respiratory distress syndrome).
Inhalation injury and carbon monoxide poisoning should be suspected in patients exposed to fires in a closed space. The clinical consequences include impaired gas exchange, reduced lung and chest compliance and increased pulmonary vascular resistance.
- Carbon monoxide has 200 times greater affinity for haemoglobin than oxygen. This reduces oxygen carriage in the blood. Treatment is to administer 100% oxygen, if necessary by intubation and ventilation. Severe cases require hyperbaric oxygen.
- Non-fire-resistant synthetic fabrics and foams release cyanide and other toxic substances. Cyanide inactivates the enzyme cytochrome oxidase, leading to uncoupling of mitochondrial oxidative phosphorylation and inhibition of cellular respiration. Cyanide poisoning should be considered in the presence of severe unexplained metabolic acidosis. Treatment includes 100% oxygen, sodium nitrite (which induces methaemoglobin in red blood cells, and combines with cyanide to free the cytochrome oxidase enzyme) and thiosulfate (which has a higher affinity to cyanide than methaemoglobin and produces thiocyanate, which is renally excreted).
- Some plastics release chlorine on combustion. Administration of the _2-agonist terbutaline combined with the inhaled corticosteroid budesonide produces considerable improvement in lung function in these cases.
Circulation – Fluid resuscitation
The inflammatory cascade is activated immediately and the release of histamine, complement factors and cytokines causes marked vascular permeability and vasodilatation. Profound tissue oedema occurs both at the burn site and throughout the body tissues. The localised tissue swelling around the site of the burn is usually at its worst within 12 hours of resuscitation, but after 24 hours generalised oedema in unburned tissue is often encountered in patients with more than 30% TBSA burns.
A delay in fluid resuscitation increases renal failure and mortality, and inhalational injury increases fluid requirements. The most common volume restoration regime uses the Parkland formula. In this 4mls of Hartmann’s solution (lactated Ringer’s solution) per kilogram of body weight, per percentage total body surface area burn is given in the first 24 hours. The first half of this volume is given over eight hours and the second half given over the following sixteen hours.
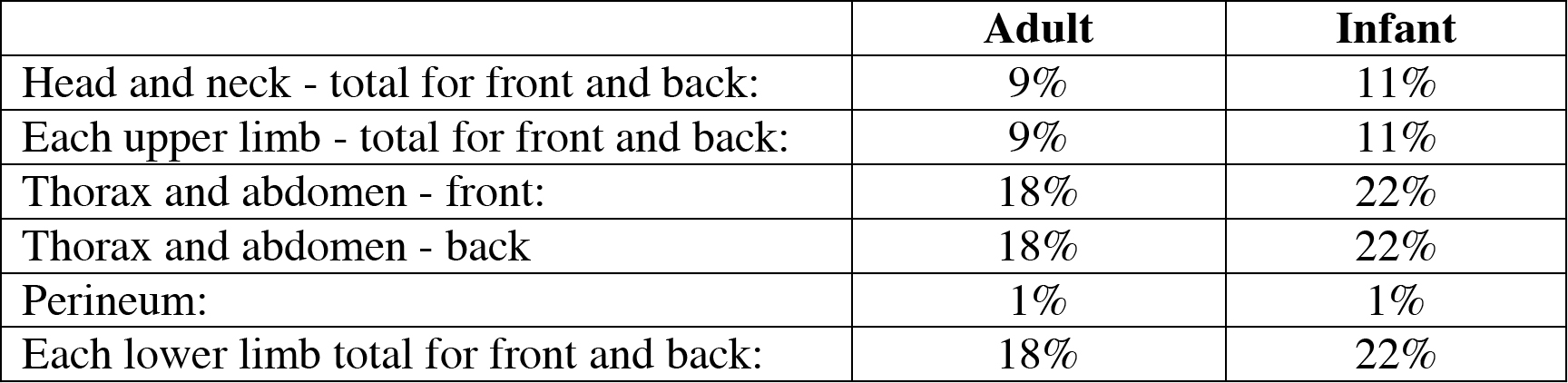
In order to work out how much fluid to give the percentage total body surface area burn must be estimated. In adults a diagram dividing the body into areas of 9% surface area can be used to approximate the size of burn. In infants there is a similar diagram using areas of 11% surface area:
Percentage surface area of body parts for adults and children
Classification of burns:
- Superficial – superficial epidermal burns are red, painful and blisters are not present. They heal by epithelisation.
- Partial thickness – these are superficial dermal burns that are blistered, painful and also heal by epithelisation without scarring.
- Full thickness – these areas have lost all adnexal structure and heal by secondary intention with scarring. They are subdivided into deep dermal burns (blistered with a blotchy red appearance, no capillary return on pressing and absent sensation to pin prick) and full thickness burns (white or charred appearance, ‘escar’ with loss of sensation.
When calculating total burn surface area you should count all areas of burn except areas of erythema.
Studies show that the percentage burn is often overestimated (by nearly 25%) in inexperienced hands. Estimation is often difficult, particularly in females and obese patients. Remember that this is only a guide – fluid resuscitation will routinely exceed calculated needs.
Clinicians tend to be wary of massive fluid resuscitation in burns, concerned about causing lung oedema and worsening tissue oedema, which will cause poor tissue perfusion or even compartment syndrome. However, studies show that in the first 48 hours extravascular lung water (a measure of the tendency to develop pulmonary oedema) rarely increases, even if the volume administered exceeds the Parkland formula by 400%. Respiratory compromise may, in fact, be a result of small airway closure, ventilation-perfusion mismatch and pulmonary shunting rather than pulmonary oedema.
Studies measuring circulating blood volume in severe burns show that the intravascular volume is often about two-thirds that of healthy controls; this persists for at least four days and is not corrected by additional fluid administration. A comparison of the Parkland formula and pulmonary artery catheter guided resuscitation reveals no difference in mortality and morbidity despite the second group receiving substantially more fluid.
A more usable resuscitation goal is accepted as a urine output of 0.5-1 ml/kg per hour. The role of lactate and base deficit to reflect resuscitation is being evaluated.
Secondary Survey (a full review of the patient from head to toe)
Do not be distracted by the burn alone but look for other injuries. Fractures are the most frequent associated injury. Explosions can result in a tension pneumothorax or pulmonary contusion. As in any trauma, the cervical spine must be considered to be at risk especially if a fall or trauma is involved. A brain CT scan is indicated if there has been a significant fall or the Glasgow Coma Scale is reduced.
Management in the Operating Room
General anaesthesia may be required for:
- Initial excision of damaged tissue.
- Later excision of granulation tissue and skin grafting.
- Changes of dressings.
- Plastic surgery to relieve contractions, improve limb function or deformity and cosmetic.
In major burns when insufficient donor skin is available for grafting ‘BioBrane’ or ‘Integra’ may be used.
- Biobrane is a biosynthetic skin substitute which is constructed of an outer silicone film (an epidermal analogue) with a nylon fabric partially imbedded into the film. Collagen is incorporated in both components, binding to the wound surface. Small pores are present in the structure to allow for drainage of exudate and also provide permeability to topical antibiotics.
- Integra is a bilayer skin replacement system that helps the body to grow new skin. It is used for the immediate treatment of severe burn injuries and the surgical replacement of scar tissue to improve function or mobility (scar contracture release).
The problem with these coverings is that infection can spread under them rapidly. Previous donor sites can be re-used and in some centres skin can be cultured.
Airway
- Burned skin may make a face mask painful to apply.
- Fibrosis and contactures may reduce movements of the jaw and neck.
- Securing the endotrachial tube may be difficult.
- Oedema may develop in the tissues around the endotracheal tube, which may cause obstruction when the tube is removed.
Use of suxamethonium
Depolarising muscle relaxants cause hyperkalaemia by release of potassium into the circulation from damaged muscles. This can occur between a few days after the injury until about 10 weeks after the injury. Suxamethonium is best avoided but may be considered immediately after the injury, when the risks of use are weighed against the expected difficulty of intubation.
Ventilation
For major burns intermittent positive pressure ventilation is preferred to spontaneous ventilation, since the metabolic rate, and therefore oxygen consumption, is increased in significant burns. Ventilation perfusion mismatch is likely and a higher FiO2 and PEEP are recommended.
Circulation
Excision of damaged tissue, granulation tissue and grafting is accompanied by extensive fluid and blood loss. Large-bore venous access and availability of cross-matched blood are essential for all but the most minor procedures. Extensive debridement often retriggers the inflammatory response and oedema and cardiovascular instability will often worsen during and after surgery.
Hypotension should be treated with fluid or, where indicated, blood administration. Use of noradrenaline infusions may impair blood flow to grafts and is unpopular with burns surgeons. Use should be limited to cases where end-organ perfusion cannot be achieved by fluids alone.
Heat Loss
Evaporation from the burned area and inability to constrict vessels increases heat loss. The ambient theatre temperature should be elevated, the patient’s temperature monitored and, where available, a warming blanket and fluid warmer should be used.
Management in the Intensive Care Unit
- Mortality can be estimated using the abbreviated burn severity index (ABSI) in which sex, age, inhalation injury, depth of burn and TBSA correlate with survival. For patients over 75 years of age the Baux score (age + % TBSA burned) is approximately equal to the percentage mortality.
- The major predictor of morbidity and mortality after burn injury is the presence of inhalation injury.
Airway
As facial swelling occurs the endotracheal tube may migrate out of the trachea. There is a risk of inadvertent extubation and tube position is best assessed by chest Xray.
Breathing and ventilation
Barotrauma (or volutrauma), resulting from excessive excessive airway pressure or tidal volume may cause secondary injury to the lungs. Many patients progress to develop ARDS with an associated high morbidity and mortality.
Most advocate use of a protective ventilation strategy, with limited plateau pressure (<35 cmH2O), smaller tidal volumes (up to 6 ml/kg), lower minute volume allowing higher PaCO2 (permissive hypercapnia), pressure-control rather than volume-control ventilation (PCV generates lower peak inflation pressure for same tidal volume) and higher PEEP (10 or 12 cmH2O instead of 5 or 6 cmH2O).
Pneumonia occurs in 48-56% of burn patients, with double the risk in those with inhalation injury. Half will have developed their primary infection by day 3. Most bacterial agents responsible arise from the patients’ oropharyngeal and gastrointestinal flora, and are often community-acquired bacteria including Staphlococcus aureus, Streptococcus pneumoniae, and Haemophilus influenzae. Secondary pneumonia usually occurs by day 16 and is commonly caused by methicillinresistant S. aureus, Pseudomonas, or Enterobacter. Antibiotic therapy is guided by microbiological tests, local species sensitivities and the availability of antibiotics.
Nutrition and enteral feeding
Initially, there is an acute decrease in metabolic rate and cardiac output decreases to 5060% of the normal resting value. However, within hours, the metabolic rate increases to peak at 7-12 days post-injury. This hyper-metabolic state triggers severe catabolic protein loss and results in impaired immune function and delayed wound healing.
The metabolic surge is attenuated and the consequences controlled by early closure of the wound (by debridement and grafting) and early enteral feeding (nasogastric or nasojejunal).
Enteral feeding helps to maintain intestinal barrier function and prevent bacterial and fungal translocation from the bowel lumen, reducing the incidence of infective complications. For this reason, enterally-fed patients may have higher survival rates than those fed parenterally. However it is important that patenteral feeding is instigated early when enteral feeding fails or is not possible.
Immune function and sepsis
Patients should be treated as immunocompromised. In burns over 40% TBSA, virtually all specific (cell-mediated and humoral) and non-specific (polymorphonuclear leukocyte, macrophage) immune function is deranged.
The first 48 hours of burn injury are usually free from infection, although hypermetabolism often causes hyperpyrexia. Blind antibiotic use should be avoided over this period, unless microbiological specimens confirm bacteraemia.
Reactivation of herpes simplex virus can be detected in 53% patients in the first week. Facial herpetic infection is found in 15% of intubated patients with severe burns during the second week. Herpes viruses are associated with increased mortality, extensive visceral involvement, and necrotising tracheobronchitis. Treatment with acyclovir may result in reduced severity of infection.
Blood transfusion
Increased blood loss is influenced by older age, male sex, larger body size, full-thickness burns, high wound bacteria counts, operative time and delay to primary burn excision. Haemostasis is aided by tourniquet use and subcutaneous infiltration of adrenaline and saline solution prior to debridement and grafting. Blood transfusion may contribute to non-specific immune dysfunction.
Pain management
Burns cause intense and prolonged pain, that is exacerbated by the need for frequent dressing changes to prevent infection and aid healing. Skin grafting requires the debridement of non-viable tissue and the application of skin grafts; this will often decrease the duration of a patient’s pain. The donor sites are likely to be painful for 48 to 72 hours. Donor-site dressings should be left in place until they peel away of their own accord.
Simple analgesics
Background pain can be managed with paracetamol, non-steroidal anti-inflammatory drugs (NSAIDs) and oral opioids (oramorph or morphine sulphate).
Opioids
Pain due to procedures can be controlled by administration of intravenous opioids (morphine, fentanyl or alfentanil); awake patients may be able to use patient controlled analgesia (PCA) with morphine, pethidine or fentanyl. Patients with severe burns, treated over a long period of time may continue to experience pain despite an escalation in opioid dose requirement (this may be opioid tolerance or increased pain sensitivity).
Ketamine
Intravenous ketamine can be used, but sites for IV cannulation may be limited and these are best saved for trips to theatre. IM ketamine is also an option but requires relatively large painful IM injections.
Ketamine can be given orally: for an adult give 500mg of ketamine + 5mg diazepam. For children use 15mg/kg ketamine + 0.2mg/kg diazepam. The IV preparation can be used but its taste must be hidden in juice. Responses can sometimes be unpredictable, but the dressing change can usually start after 20-30 minutes.
Ketamine is a potent NMDA antagonist and can reduce the pain transmission pathway implicated in the development of central sensitisation (secondary hyperalgesia or ‘windup’ pain).
Nitrous oxide/oxygen mixture (Entonox)
Entonox is safe, has rapid onset analgesia and can be used for the duration of the procedure. However the potency of analgesic is limited and may be insufficient for requirements.
Long-term consequences
Long-term consequences include disfiguring, scarring, skin retraction and functional disability. Depression scores correlate with burn size, trait anxiety and general patient well-being. Early identification of depression enhances recovery and rehabilitation. Dysphagia often develops after prolonged endotracheal intubation and can persist for up to 2 months. Neuropathy is common in the elderly and the critically ill. It is particularly frequent in patients with electrical injuries where the neuronal lipid membrane is damaged and a polyneuropathy can result.
Further reading
- Walton and Manara. Burns and smoke inhalation. Anaesthesia and Intensive Care Medicine; 6: 317-321
- Burn Injuries. Marko et al. Current Opinion in Anaesthesiology; 16: 183-191
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/