Obstetrics Anaesthesia

KEY POINTS
- There has been a substantial rise in recreational drug use amongst the general population within the last three decades. Parturients who abuse drugs are 80% more likely to require the involvement of an anaesthetist for analgesia.
- The most commonly abused drugs include alcohol, opioids, cocaine, amphetamines, marijuana and hallucinogens.
- Illicit drug abuse can result in cardiovascular, respiratory, neurological and haematological adverse effects.
- Anaesthetic agents can interact with illicit drugs.
- Pregnant women with a history of substance abuse are more likely to suffer: poor general health, untreated coexisting disease, and inadequate antenatal care.
- A multidisciplinary team approach with the aim to optimise care includes: obstetricians, general practitioners, anaesthetists, midwives and drug/alcohol services.
INTRODUCTION
There has been a substantial rise in recreational drug use in the developed world within the last three decades. Depending on the population being studied, the incidence of substance abuse during pregnancy ranges from 0.4-27%.1,2,4 The most commonly abused drugs include alcohol, opioids, cocaine, amphetamines, marijuana and hallucinogens.1 Women dependent on illicit drugs place high demands on anaesthetic and obstetric services as parturients who abuse drugs are 80% more likely to require the involvement of an anaesthetist for analgesic purposes.1 The combination of clinical manifestations of drug abuse, physiological changes of pregnancy, and the pathophysiology of pregnancy-related disease can result in poor foetal outcomes and serious maternal morbidity, e.g. placental abruption resulting in foetal distress.2 Achieving effective analgesia post-caesarean section in addicted patients may be challenging.2 There are identifiable interactions between anaesthetic drugs and drugs of abuse. Sedating agents reduce minimum alveolar concentration (MAC), while stimulants increase MAC.3 It is often difficult to predict the exact repercussions in the chemically-dependent patient.2 When drugs are abused intravenously there are other considerations for healthcare providers: venous access may be difficult and there is a higher prevalence of transmissible diseases such as hepatitis (B and C) and human immunodeficiency virus (HIV).1
ALCOHOL
Pregnant patients with a history of alcohol abuse may present in several ways: acute intoxication, withdrawal, or with chronic alcohol abuse.1
Maternal and foetal considerations
Acute alcohol intoxication can cause foetal distress and increases the risk of maternal pulmonary aspiration.1,2 Acute alcohol withdrawal may cause foetal distress, autonomic instability, seizures and maternal cardiac failure. Symptoms can be managed with benzodiazepines or alpha-2-adrenoceptor agonists, however with larger doses the risk of neonatal respiratory depression should be considered. Chronic alcohol abuse is associated with liver disease, coagulopathy, cardiomyopathy and altered drug metabolism.1,2
Neuraxial analgesia and anaesthesia
In patients who abuse alcohol, neuraxial analgesia and anaesthesia is safe and preferable, provided there is no associated synthetic liver dysfunction in the form of coagulopathy.1,2 Consent is challenging in acutely intoxicated and uncooperative patients who may lack capacity.1,2 Attention to assessing and replacing fluid deficits can help to diminish potential adverse effects of sympathetic blockade.2
General anaesthesia
General anaesthesia poses an increased risk of pulmonary aspiration in patients with acute alcohol intoxication. A rapid sequence induction technique is recommended with consideration to a reduced induction dose.1,2 Chronic abuse usually requires higher induction agent doses, although thiopentone dosing is not affected by chronic alcohol intake.1 The presence of liver or cardiac failure will require appropriate adjustment.3
OPIOIDS
Opioid abuse in pregnancy can include the use of heroin (diamorphine), fentanyl and prescription opioid-based analgesic medications.4 The obstetric anaesthetist can be involved in several aspects of care including: analgesia, anaesthesia and the management of overdose or withdrawal.
Maternal and foetal considerations
In chronic untreated opioid-use there are risks to both mother and foetus which may be related to repeated exposure of the foetus and placenta to opioid withdrawal.1 Once physical dependence has developed, a withdrawal syndrome can occur within 4-6 hours of heroin use.4 Recurring placental and foetal opioid withdrawal may result in intra-uterine growth restriction (IUGR), placental abruption, foetal death and preterm labour.2
Maternal overdose can present with respiratory depression, respiratory arrest or aspiration.2 Withdrawal increases sympathetic nervous system (SNS) activity causing tachycardia, hypertension and restlessness.2 There may be associated polysubstance abuse, and infection with hepatitis B, C and/or HIV.5
Neuraxial analgesia and anaesthesia
Prior to providing neuraxial analgesia to patients who abuse opioids it is advisable to exclude cellulitis, coagulopathy, sepsis, endocarditis and septic arthritis as these are associated with an increased incidence of neuraxial and disc-space infections. The National Institute for Clinical Excellence (UK) recommends an intrathecal dose of 300-400 mcg diamorphine (equivalent to 100-150 mcg of morphine) in opioid-naïve patients undergoing caesarean section but this does not account for opioid-tolerant parturients when higher doses may be required to achieve an equivalent analgesia level. Side effects are increased with higher opioid doses.6 Opioid-tolerant patients receiving labour epidural analgesia may require a higher infusion rate and/or dosage (e.g. 4 mcg/ml compared to the standard 2 mcg/ml of fentanyl) which can be supplemented with an initial epidural bolus dose of 75-100 mcg fentanyl.8
General anaesthesia
General anaesthesia induction dose requirements are increased with chronic opioid use and are decreased with acute ingestion, although associated malnutrition may also necessitate dose adjustment.1,2,4 The use of ultrasound to aid peripheral intravenous access may be necessary due to obliterated veins, and central venous access may be required. In an emergency situation intraosseous needle insertion may be a useful alternative.1 Postoperative pain may be exaggerated and difficult to control, therefore a multimodal regimen should be the goal.1 Regular (maintenance) and ‘as required’ opioids should be prescribed for postoperative analgesia. Opioid-sparing techniques should be considered such as multimodal (non-opioid based) analgesia, and transverse abdominis plane (TAP) blocks or catheters.
COCAINE
Cocaine is a recreational drug commonly used in pregnancy in developed countries, is not specific to any particular cohort and is often co-abused.
Maternal and foetal considerations
Cardiovascular sensitivity to cocaine increases in pregnancy which increases myocardial oxygen demand beyond that which already occurs during pregnancy. This predisposes the parturient to myocardial ischaemia, infarction and arrhythmias.1 Respiratory complications include asthma, pulmonary haemorrhage and nasal septal collapse.9 There is a four-fold increase in rates of emergency caesarean section following placental abruption and foetal distress.1 Other complications include teratogenic effects, IUGR and preterm labour.1,2 Acute intoxication can cause serotonin syndrome and may also be misdiagnosed as pre-eclampsia as it can present with hypertension, and/or seizures, hyper-reflexia, thrombocytopenia, proteinuria and oedema.1,3
Neuraxial analgesia and anaesthesia
Neuraxial techniques are considered the ideal method to deliver analgesia and anaesthesia in patients who abuse cocaine. However, neuraxial procedures may be contraindicated in patients with cocaine-induced thrombocytopenia.1,10 Physiological alterations in pain perception may result in inadequate analgesia despite a functioning epidural catheter. Intrathecal opioids may have a reduced duration of action due to pronounced abnormalities in mu and kappa opioid receptor densities as a result of cocaine addiction.1 Phenylephrine is the preferred vasopressor as cocaine use can cause resistance to ephedrine.1
General anaesthesia
Induction
In patients who abuse cocaine, supplemental agents(s) are advised to obtund the hypertensive response to laryngoscopy. Beta-blockers are contraindicated as they cause unopposed alpha-stimulation possibly with subsequent hypertension and coronary vasoconstriction. Labetalol (combined alpha and beta-blocker) is recommended, but it is controversial as unopposed alpha-stimulation may still occur. Glyceryl trinitrate (nitroglycerine), sodium nitroprusside and a combination of intravenous magnesium with remifentanil or alfentanil have all been used successfully.1 Judicious use of benzodiazepines may also reduce sympathetic-mediated hypertension. Hydralazine can be used but may cause reflex tachycardia.1 Propofol and thiopentone can be considered for induction of anaesthesia, ketamine should be avoided due to its sympathomimetic actions.1,3 Effects of succinylcholine may be prolonged as cocaine metabolism depletes pseudocholinesterase.1
Maintenance
Cardiac arrhythmias, hypertension and myocardial ischaemia are all described in the peripartum period in parturients who abuse cocaine.10,11 Avoidance of halothane is advised as it sensitises the myocardium to catecholamines, as is desflurane due to association with an increased sympathetic stimulation.
AMPHETAMINES
Amphetamines are sympathomimetic drugs that structurally resemble noradrenaline (norepinephrine) and are profoundly serotonergic.2,9 Methamphetamine is the most commonly abused drug in this class and can be utilised orally, intravenously or smoked.1,2
Maternal and foetal considerations
As with cocaine, acute intoxication with amphetamines can be mistaken for gestational hypertension or pre-eclampsia with signs of hypertension, and/or seizures and hyperreflexia.1 Foetal and placental complications may be attributable to vasoconstriction and reduced uteroplacental blood flow leading to IUGR, placental abruption and preterm labour.1
Neuraxial analgesia and anaesthesia
Neuraxial techniques are the preferred method to provide analgesia and anaesthesia in patients who abuse amphetamines, although hallucinogenic effects may affect behaviour and prevent the patient’s ability to give informed consent or allow safe and controlled placement of a neuraxial block.2 Cardiovascular response to neuraxial anaesthesia may be unpredictable depending on the competing physiological effects of acute and chronic ingestion. Invasive arterial monitoring and titrated phenylephrine infusion should be considered.
General anaesthesia
Recommendations are similar to those for cocaine abuse, to avoid halothane, desflurane and ketamine due to cardiovascular effects.1,2 Acutely intoxicated patients have increased anaesthesia induction and maintenance requirements, while chronic abusers have decreased anaesthetic requirements.1 In clinical practice anaesthetic drugs should be titrated to effect.1,2 The patient’s temperature should be closely monitored as amphetamines can cause serotonin syndrome-associated hyperthermia resulting in heat stroke fatality.1,3
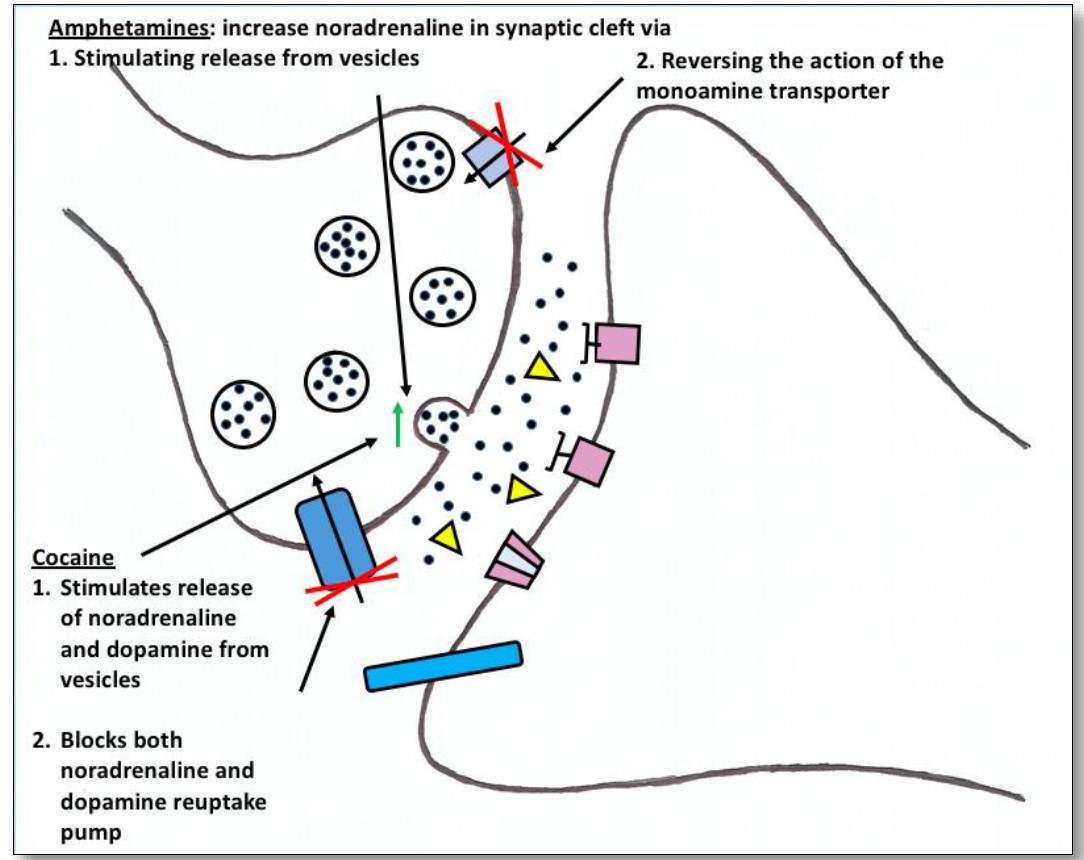
Figure 1: Effects of amphetamines and cocaine at the synaptic cleft. By Harriet Daykin
MARIJUANA
After tobacco and alcohol, marijuana is the most commonly abused drug in pregnancy.1,2 It is commonly available and is now legal in many jurisdictions. It varies in potency.4
Maternal and foetal considerations
Initially sympathetic activity is increased with low doses of marijuana, although at high doses parasympathetic tone predominates and the patient may become bradycardic and hypotensive.1 Acute intoxication affects cognitive and motor performance, as well as causing ST and T wave changes. Life threatening arrhythmias are rare in patients without pre-existing cardiac disease, but there is an increase in supraventricular and ventricular ectopic activity.1,9 Both acute intoxication and chronic use can decrease the ability to give informed consent. Marijuana readily crosses the placenta causing foetal complications such as IUGR and preterm labour.1
Neuraxial analgesia and anaesthesia
Neuraxial techniques are the preferred mode for analgesia and anaesthesia management in patients who abuse marijuana, although the patient may lack capacity to consent.1
General anaesthesia
Respiratory complications from marijuana-use include oropharyngeal and uvular oedema which increase the risk of difficult intubation.1 Upper airway irritability may predispose the patient to bronchospasm and larnygospasm.9 Some have therefore recommended administering intravenous dexamethasone as a prophylaxis for those patients undergoing general anaesthesia.9 Marijuana may potentiate anaesthetic agents affecting heart rate and blood pressure, therefore ketamine, pancuronium, atropine and adrenaline (epinephrine) are best avoided due to their cardiovascular side-effects.1,2 The effects of succinylcholine may be prolonged as marijuana inhibits cholinesterase activity, and it can also cause a cross-tolerance with opioids, benzodiazepines and barbiturates.1,2 When acutely intoxicated, analgesic effect is related to dose of marijuana: low doses do not affect pain levels; moderate doses reduce pain scores; and high doses are associated with increased pain.1
KETAMINE AND OTHER HALLUCINOGENS
Hallucinogens include ketamine, lysergic acid diethylamide (LSD), phencyclidine (PCP) and ‘magic mushrooms’.1 These substances stimulate the SNS which may cause hyperthermia, and cause hallucinations which can provoke anxiety.1,2
Maternal and foetal considerations
Multi-organ complications can occur as a result of ketamine and hallucinogenic drug abuse. There is a risk of associated autonomic dysregulation with ketamine and other hallucinogenic drugs, which can present with labile blood pressure, tachycardia, plus coronary and cerebral vasospasm.2 Overdose can lead to respiratory depression, seizures and coma, whereas water intoxication from LSD induced thirst can cause pulmonary and cerebral oedema with electrolyte abnormalities.1,9 Drug induced hypertension and proteinuria, with or without seizures can be mistaken for pre-eclampsia.1,2 Hyperthermia increases maternal and foetal oxygen demand which can result in foetal heat-induced neurological injury.1 Ketamine readily crosses the placenta but sub-anaesthetic doses are not known to have any adverse foetal effects.1
Neuraxial analgesia and anaesthesia
Neuraxial techniques are the first choice in cooperative patients, however vasopressors should be used with caution to treat cardiovascular instability as an exaggerated response can occur.2,9
General anaesthesia
Haemodynamic instability is a primary concern during the conduct of general anaesthesia in these patients. General anaesthetic effects may also be prolonged as hallucinogens can prolong both the analgesic and ventilatory depressant effects of opioids. MAC requirements are reduced with ketamine abuse while PCP and LSD can prolong the effects of succinylcholine as they inhibit plasma cholinesterase. All hallucinogens can potentially induce postoperative anxiety and psychosis.1,2
BREASTFEEDING
In the United States, women who have established breastfeeding but subsequently relapse into illegal drug abuse are generally counselled not to breastfeed their infant due to lack of data on the correlation between concentrations in breast milk and effects on the infant. Exceptions to this are methadone, buprenorphine and alcohol abusers.12
- Methadone: transfer to breast milk is low, breastfeeding should be encouraged.12
- Buprenorphine: concentration in breast milk is low and unlikely to affect the developing infant.12
- Other opioids: caution is advised with codeine due to CYP2D6 ultra-rapid metabolisers resulting in high morphine metabolite levels.12
- Alcohol: breast milk levels reflect maternal blood alcohol levels. It is advised to avoid breast feeding immediately after ingestion, but that it is safe to do so two hours after an intake of 8 oz of alcohol.12
PSYCHOLOGICAL AND SOCIAL CONSIDERATIONS
Drug abuse is a significant social problem that poses a number of challenges in the peripartum period, and can lead to serious obstetric morbidity and mortality.2 Substance-abusing parturients are more likely to suffer poor general health, malnourishment and untreated coexisting disease. They are also less likely to engage with antenatal care.1,2 There is an association with poverty, domestic violence, physical and/or sexual abuse and mental illness.5,13 These issues increase the risk of criminal activities and the likelihood of social service intervention, including child protection orders.1,5 A multidisciplinary team approach optimises care and includes obstetricians, general practitioners, anaesthetists, midwives and drug/alcohol services.2 Lack of antenatal care results from concern about stigmatisation by medical professionals, fear of mandatory reporting to social services, legal ramifications, and losing custody of baby.13
An early antenatal referral for anaesthetic review is recommended as opioid-dependent women in particular benefit from antenatal pain management planning. A non-judgmental anaesthetic evaluation is essential with management tailored to the individual patient and obstetrical needs.2
SUMMARY
The table below summarises the relevant pathophysiological changes that can occur with substance misuse when considering the anaesthetic and analgesic management of the pregnant woman. Neuroaxial intervention is generally preferred, although consent is an issue when acutely intoxicated.
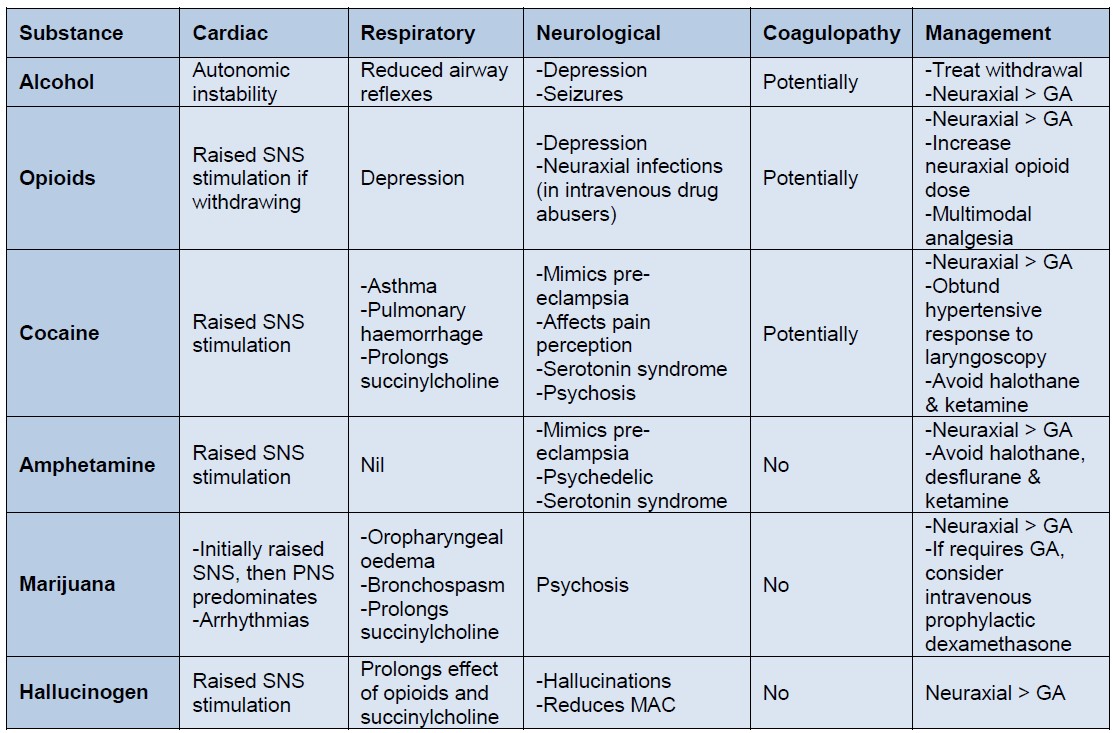
Table 1: summary of pathophysiological considerations and anaesthetic management
GA: general anaesthesia
SNS: sympathetic nervous system
PNS: parasympathetic nervous system
REFERENCES AND FURTHER READING
- McConachie I. Controversies in Obstetric Anesthesia and Analgesia. Chapter 1: Substance abuse in pregnancy. 1st edition. Cambridge: Cambridge University Press 2011
- Ludlow J, Christmas T, Paech M, Orr B. Drug abuse and dependency during pregnancy: anaesthetic issues. Anaesth Intensive Care 2007; 35: 881-893
- Roberts T, Thompson JP. Illegal substances in anaesthetic and intensive care practices. Continuing Education in Anaesthesia, Critical Care & Pain 2013; 13: 42-46
- Joan Keegan DO, Mehdi Parva, Mark Finnegan, Andrew Gerson & Michael Belden. Addiction in Pregnancy. Journal of Addictive Diseases 2010; 29: 175-191
- Committee Opinion. Opioid abuse, dependence and addition in pregnancy. Obstetrics & Gynecology 2012; 119: 1070-1076
- Hindle A. Intrathecal opioids in the management of acute postoperative pain. Continuing Education in Anaesthesia, Critical Care & Pain 2008; 8: 81-85
- Tsai F, Wu G, Lin C, Huang C, Chen S, Chen L. Optimizing epidural fentanyl loading dose for early labor pain. Acta Anaesthesiol Taiwan 2009; 47: 167-172
- Siddick-Sayyid SM, Taha SK, Azar MS et al. Comparison of three doses of epidural fentanyl followed by bupivacaine and fentanyl for labor analgesia. Acta Anaesthesiol Scand 2008; 52: 1285-1290
- Hernandez M, Birnbach DJ, Sundert AAJ. Anaesthetic management of the illicit-substance-using patient. Current Opinion in Anaesthesiology 2005; 18: 315-324
- Wong CA. Anesthesia in High-Risk Obstetrics. http://www.glowm.com/section_view/heading/Anesthesia%20in%20High-Risk%20Obstetrics/item/217 Accessed 21/07/2016.
- Kuczkowski K. Cocaine: a review of anaesthetic considerations. Can J Anesth 2004; 51: 145-154
- Reece-Stremtan S, Marinelli KA, Academy of Breastfeeding Medicine. Guidelines for Breastfeeding and Substance Use or Substance Use Disorder, Revised 2015. Breastfeeding medicine 2015; 10: 135-141
- Kremer ME, Arora KS. Clinical, ethical and legal considerations in pregnant patients with opioid abuse. Obstetrics & Gynecology 2015; 126: 474-478
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/