Covid-19

Self assessment
Consider these questions before reading the tutorial.
- How would you diagnose respiratory failure in a newly-presenting septic patient? What clinical signs would suggest respiratory failure?
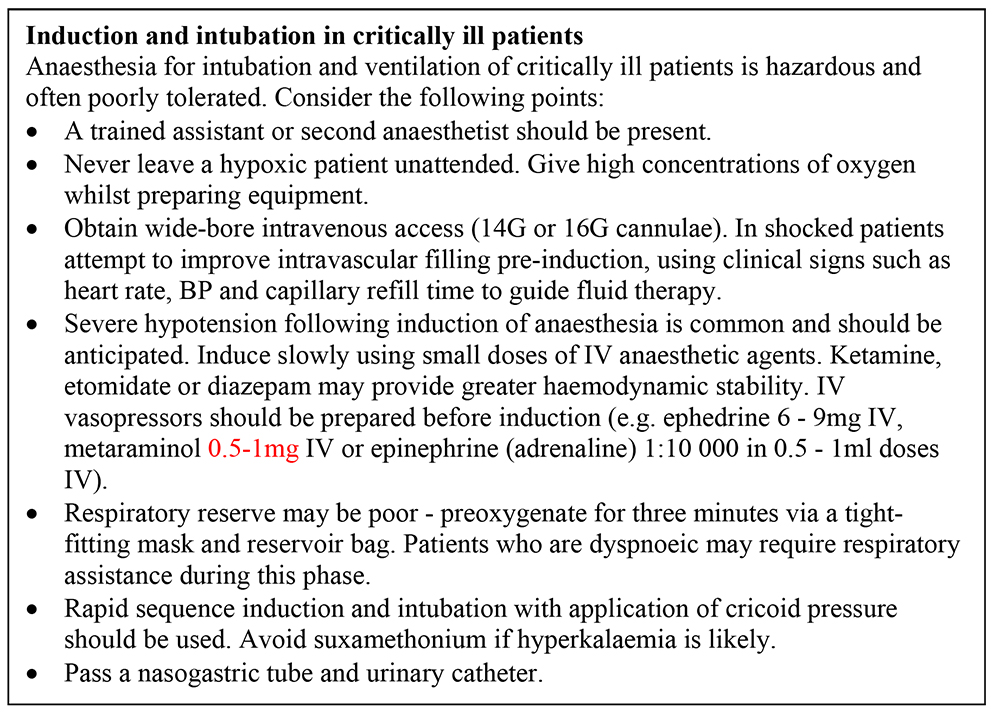
- Describe the preparations you would make to intubate and ventilate a 45-year-old man with severe pneumonia and sepsis. What drugs would you prepare before induction?
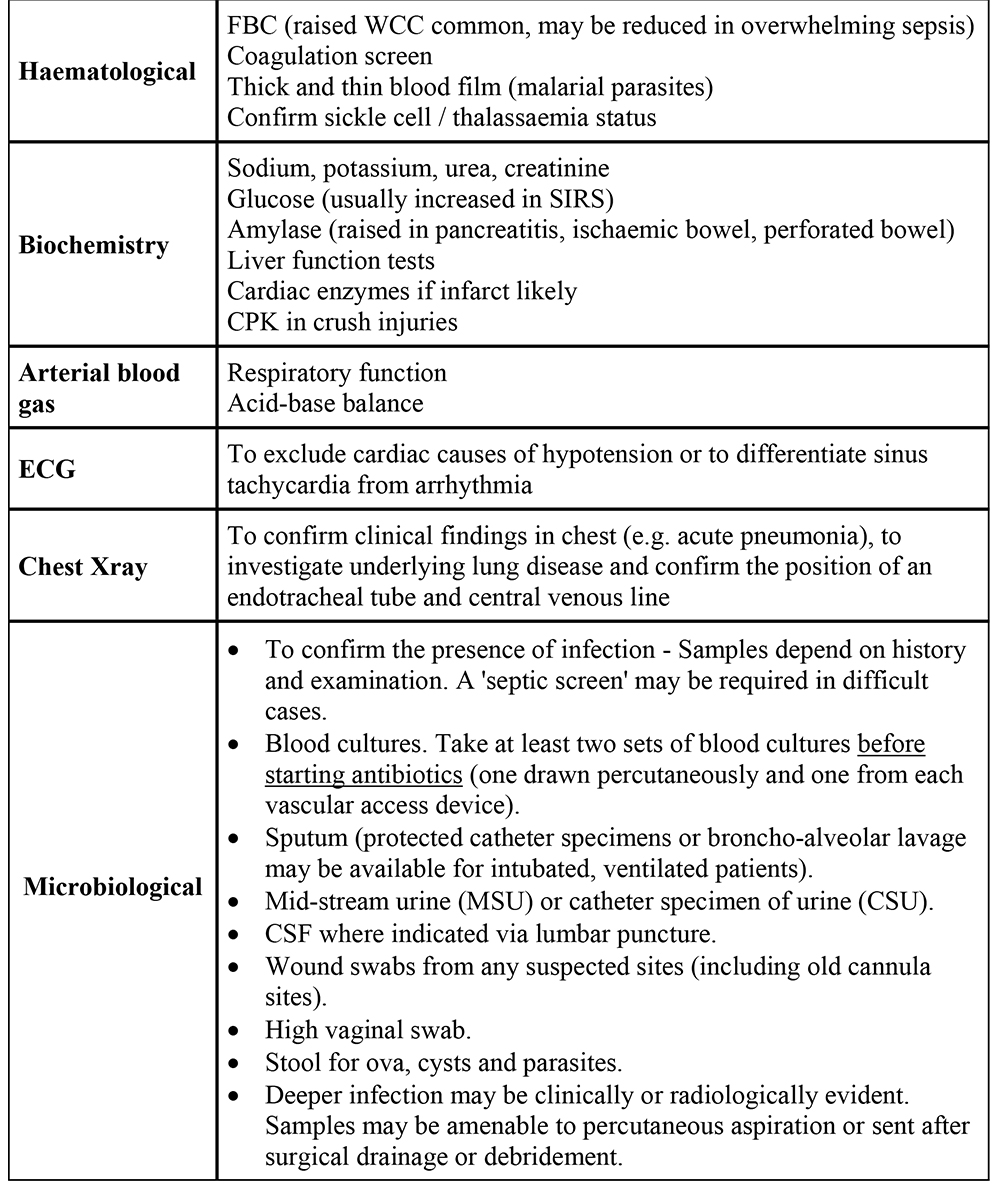
- How do you decide what investigations to do in a septic patient?
- The surgeon has a man of 55 years with necrotising fasciitis of his groin and lower abdominal wall – he wants to take him straight to theatre. The patient is drowsy and confused. His observations are: temperature 39.1°C, pulse 125/min and BP 90/55. His Hb was 8.1 g/dl yesterday and the surgeon thinks there are 2 units of blood available. Do you take him straight to theatre to anaesthetise him or delay surgery to assess and treat him first?
- How would you chose to maintain anaesthesia in a man undergoing laparotomy for a perforated sigmoid volvulus, who has a blood pressure of 80/35 after induction with ketamine 50mg and suxamethonium 100mg?
Introduction
Sepsis describes the host response syndrome to an infectious insult. It is characterised by a pro-inflammatory, pro-coagulant state and is frequently accompanied by organ dysfunction resulting from organ hypoxia.
Definitions
A consensus conference in 1992, formally defined terms such as sepsis and septic shock:1
- Systemic inflammatory response syndrome (SIRS) replaced the previous term sepsis syndrome’. This is the body’s response to a variety of severe clinical insults. It is characterised by the presence of two or more of: temperature >38°C or <36°C, heart rate > 90/min, respiratory rate > 20/min or PaCO2 <4.3kPa, white cell count >12 x 109/l, < 4 x 109/l or greater than 10% immature neutrophils.
- Sepsis is defined as SIRS in response to infection.
- Severe sepsis is sepsis associated with:
- organ dysfunction (altered organ function such that normal physiology cannot be maintained without support)
- hypotension (systolic blood pressure < 90mmHg or a reduction of > 40mmHg from the patient’s normal in the absence of other causes of hypotension)
- organ hypoperfusion (revealed by signs such as lactic acidosis, oliguria, acute alteration of mental status).
- Septic shock describes sepsis with hypotension despite adequate fluid resuscitation.
- Multiple organ dysfunction syndrome (MODS) describes a state where dysfunction is seen in several organs.
Management
Initially resuscitate the patient by assessment of the airway, breathing and circulation (ABC). Seek a brief history and perform a limited examination of the relevant body systems. Then conduct a secondary assessment of the patient, including a more thorough history, detailed examination by system and appropriate investigations.
Initial management
Problems encountered during the initial assessment should be deal with as they are identified
Airway and breathing
- Give oxygen.
- A depressed conscious level is the most common cause of airway compromise. Patients who do not localise to a painful stimulus have inadequate airway protection reflexes. Intubation and mechanical ventilation are indicated, but if unavailable nurse in the recovery position.
- When the airway is patent, assess the patient’s breathing. Respiratory failure is indicated by failure of oxygenation and may be accompanied by ventilatory failure, leading to a hypercapnoea. Arterial blood gas measurement helps in assessment, but if not available clinical diagnosis of respiratory failure is necessary.
- Clinical signs of respiratory failure are increased effort of breathing (dyspnoea, increased respiratory rate, use of accessory muscles, tachycardia and sweating) and signs of ineffective breathing (poor chest expansion, poor air entry, low SaO2, cyanosis and confusion). If respiratory failure does not improve with initial treatment, intubation and respiratory support by mechanical ventilation will be needed.
- In some cases (e.g. postoperative collapse/consolidation of the lung bases) simple manoeuvres such as sitting up, deep breathing and chest physiotherapy may improve the patient’s condition. Non-invasive ventilation or application of continuous positiveairway pressure (CPAP) by face mask is an alternative for some patients.
Circulation
- In early sepsis, patients who have not been adequately resuscitated tend to have a low cardiac output. This is due to low left ventricular preload, caused by hypovolaemia, increased venous capacitance and high pulmonary vascular resistance. Shock oftenpersists after fluid resuscitation and results from a high cardiac output with low peripheral vascular resistance. This is clinically evident as warm peripheries and bounding pulses.2
- Later in sepsis, myocardial dysfunction may contribute to shock by causing a low cardiac output. Even though these patients tend to be peripherally cold, sweaty, with weak pulses, the measured systemic vascular resistance is usually still low due tomaldistribution of the circulation and shunting of blood from some organs. Many patients present with an unclear or mixed clinical picture.2
- Resuscitation should begin as soon as sepsis is recognised. Aim for mean arterial pressure greater than 65mmHg.
- Initially infuse IV crystalloid or colloid rapidly guided by the clinical response. There is no evidence that either type of fluid is superior. Warm, vasodilated patients, with a high cardiac output, may require several litres of fluid to establish adequate intravascular filling. In patients with a mixed clinical picture or cardiac disease (either pre-existing or myocardial dysfunction related to SIRS) clinical assessment may be difficult.
- Measurement of central venous pressure (CVP) can guide fluid resuscitation and provide a route for infusion of vasopressors or inotropes. A one-off reading of CVP may be misleading but following a trend of measurements and their response to fluid challenges is helpful.
- Measure urine output hourly and aim to achieve > 0.5 ml/kg/hour.
- Resuscitation guided by measurements CVP, central venous saturation and serum lactate (‘early goal-directed therapy’) is described in part 2 of this tutorial.
History
The primary insult may be self-evident (eg trauma, burns, recent surgery) or more difficult to diagnose (eg pancreatitis, gynaecological sepsis), particularly in unconscious patients.
Examination
The examination will reflect the severity of the SIRS, the presence of shock or multiorgan failure, the state of intravascular hydration and may reveal the underlying cause. When looking for an underlying source of infection consider:
- Central nervous system: Global (sleepiness, confusion, agitation, coma) or focal (localised abnormality of movement or sensation) neurological dysfunction suggesting meningitis, encephalitis, cerebral malaria or abscess.
- Respiratory system: Mucopurulent discharge from the respiratory tract, dyspnoea, lung consolidation or pleural fluid collection.
- Gastrointestinal tract: Abdominal pain with guarding and rigidity suggesting peritonitis.
- Genital tract: Vaginal discharge or history of termination suggest gynaecological sepsis.
- Skin: Purulent skin wound, signs of inflammation (redness, pain, swelling, heat) or petechial rash (meningococcaemia), cannulation sites.
Consider non-infective differential diagnoses, such as myocardial infarction, pulmonary embolism, diabetic ketoacidosis, poisoning or drug overdose, eclampsia, cerebrovascular event.
Secondary assessment
Continue resuscitation and repeat the initial assessment (ABC) if the patient’s condition changes. The priorities during the next phase are to:
- Fill in the gaps in the patient’s acute and past medical history.
- Perform a full physical examination by system.
- Communicate with the other teams involved in the patient’s management (e.g. general surgeons for intra-abdominal infection, gynaecologists for gynaecological sepsis).
- Perform relevant investigations, governed by their availability in your hospital. Justify each investigation – think whether or not the result will alter your management of the patient. Common initial investigations are shown below.
Monitoring
- Ideally trained nursing staff should be continuous present.
- Clear documentation aids the assessment of subtle changes in the patient’s clinical state. Patients with severe SIRS should have observations recorded hourly. Record body temperature, pulse, blood pressure, urine output, CVP, respiratory rate and SaO2 (if available).
- Accurate fluid balance is essential – insensible losses may be very significant in hot climates. Ideally measure the patient’s temperature centrally (nasopharyngeal or oesophageal).
Treatment of the underlying problem
This depends on the initial insult causing the SIRS, however infection is common either as cause or as a secondary complication.
Treatment of infection may involve:
Antibiotic therapy
- In severe sepsis, start intravenous antibiotics within one hour of recognition of sepsis.
- Initial antibiotic prescription is empirical, depending on the clinical picture of the patient, local patterns of antibiotic resistance and the local availability of antibiotics. One or two drugs should be chosen to cover the most likely pathogens and to penetrate the presumed source of sepsis.
- The advice of a local microbiologist or infectious diseases specialist is recommended.
- Rationalisation of antibiotic use should be considered at 48-72 hours and is guided by microbiological results.
Source control / Surgical debridement
- Pus-filled cavities (abscess, empyema), necrotic tissue, infected tissue or gross tissue contamination (open wounds, peritonitis) will not resolve with antibiotics alone and must be urgent surgical treatment is indicated, after early assessment by the surgical team.
- Remove infected vascular devices if they are potentially the source of infection.
Anaesthesia for the septic patient
The surgical drainage of abscess cavities, laparotomies, debridement of infected wounds or amputation of gangrenous limbs may be central to the successful treatment of a patient with severe sepsis. Surgery and anaesthesia is often required, even in patients in poor clinical condition.
Pre-operative preparation
- The outcome from surgery in high risk patients is improved if the patient’s condition is optimised preoperatively. When surgery can be delayed (even for a few hours), attempts should be made to resuscitate the patient to ensure adequate oxygen delivery, cardiac output and blood pressure. This is often easiest done in theatre, recovery or ICU.
- In a few patients immediate surgery is lifesaving and should be carried out as soon as practical (eg necrotising fasciitis). Time is limited but initial resuscitation (airway, breathing and circulation) should be completed and continuing resuscitation carried out during anaesthesia.
- Common problems to be addressed are anaemia, hypotension, hypovolaemia, coagulopathy, electrolyte disturbance (particularly hyper- or hypokalaemia) and
acidosis.
Method of anaesthesia
- Physiological stability during anaesthesia is compromised by the combined effects of sepsis, anaesthesia, blood loss and surgical stress.
- Close monitoring is required because rapid changes in physiological parameters may occur.
- Induction of anaesthesia in a septic patient is described above. Supplementary analgesia may be needed. Inhalational agents will cause further vasodilation, may cause cardiac depression (halothane) and should be used cautiously.
- Ketamine anaesthesia, by repeated IV administration or infusion, is often appropriate in unstable patients providing anaesthesia and analgesia. In this situation it may be cardiovascularly depressant and does not protect the airway as effectively as an endotracheal tube.
- Anticipate that anaesthesia will compromise cardiovascular status and prepare vasoactive drugs pre-induction.
- Neuraxial blockade (spinal and extradural anaesthesia) should undertaken with extreme caution, since the haemodynamic effects of a these techniques in the setting of cardiovascular compromise may be devastating and hard to reverse. Recent blood tests confirming normal coagulation are essential. A further concern is the risk of epidural abscess complicating epidural haematoma formation.
- Peripheral nerve blockade or regional infiltration may be used and are very effective at minimising the sympathetic response to a painful stimulus, whilst avoiding the systemic effects of opioids.
Further reading
- American College of Chest Physicians/Society of Critical Care Medicine Consensus Conference: Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. Critical Care Medicine 1992; 20: 864-74.
- Dellinger RP. Cardiovascular management of septic shock. Critical Care Medicine 2003; 31: 946-55
- Surviving Sepsis Campaign Management Guidelines Committee. Surviving Sepsis Campaign guidelines for management of severe sepsis and septic shock. Critical Care Medicine 2004; 32: 858-73 Available as pdf file (800kB) at: http://www.survivingsepsis.org/hcp_index2.html
- Oxford Textbook of Critical Care. Editors: Webb AR, Shapiro MJ, Singer M and Suter PM. Oxford University Press 1999. Oxford, New York, Tokyo.
Answers to self assessment
- What clinical signs would suggest respiratory failure in a newly-presenting septic patient?
- The books tell us that respiratory failure is diagnosed by a PaO2 less than 10.6 kPa, but many centres do not have facilities for arterial blood gas analysis. This value corresponds to an oxygen saturation in the low 90s (since the oxygen dissociation curve is still fairly flat at this point) and this is not an uncommon finding in the critically ill. We therefore rely on a clinical assessment of increased effort (or work) of breathing and signs that breathing is ineffective – see text. Respiratory failure can be difficult to diagnose clinically, but repeated assessments over time make recognition of deterioration in a patient’s respiratory function and the need for respiratory support easier to judge. Don’t forget than ventilatory failure (i.e. failure of the lungs as a respiratory pump) may result in hypercapnoea, even if the SaO2 is normal.
- Describe the preparations you would make to intubate and ventilate a 45-year-old man with severe pneumonia and sepsis. What drugs would you prepare before
induction?- See text. Don’t forget to have a wide-bore cannula that is running well, to give a bolus of fluid pre-induction and to have a vasopressor agent drawn up, expecting some haemodynamic compromise after induction. Sometimes a moribund, obtunded patient, who will clearly not be able to tolerate induction can be intubated using a lignocaine spray to the vocal cords under direct vision with a laryngoscope.
- How do you decide what investigations to do in a septic patient?
- See text. Resources are restricted in almost all countries and it is wise always to ask yourself whether the result of the investigation (whether ‘positive’ or ‘negative’) will change the management of your patient.
- The surgeon has a man of 55 years with necrotising fasciitis of his groin and lower abdominal wall – he wants to take him straight to theatre for debridement. The patient is drowsy and confused. His observations are: temperature
- 39.1°C, pulse 125/min and BP 90/55. His Hb was 8.1 g/dl yesterday and the surgeon thinks there are 2 units of blood available. Do you take him straight to theatre to anaesthetise him or delay surgery to assess and treat him first?
There is no completely correct answer to this. He has a condition which is likely to advance quickly and only radical debridement will halt progression of the infection. He will not get better without an operation but he is in a poor condition to tolerate anaesthesia and the operative procedure. The solution is to negotiate a delay of no more than one to two hours with the surgeon. This is enough time to begin aggressive fluid resuscitation, to ensure blood is available and to insert a central venous cannula (if available) to guide fluid administration. If he is still hypotensive after appropriate fluid administration you can prepare an inotrope (see text) to start perioperatively as needed. Radical debridement will result in significant blood loss and your fluid resuscitation will lead to further haemodilution, so blood transfusion will be required early in the procedure.
I would do this resuscitation in the anaesthetic room if available, otherwise in theatre.
It’s always a good idea to check that he is prescribed and has received appropriate antibiotics (here high dose benzylpenicillin and clindamycin is indicated for a likely group A streptococcal infection).
- 39.1°C, pulse 125/min and BP 90/55. His Hb was 8.1 g/dl yesterday and the surgeon thinks there are 2 units of blood available. Do you take him straight to theatre to anaesthetise him or delay surgery to assess and treat him first?
- How would you chose to maintain anaesthesia in a man undergoing laparotomy for a perforated sigmoid volvulus, who has a blood pressure of 80/35 after induction with ketamine 50mg and suxamethonium 100mg?
- If you try a small amount of halothane (0.5% inspired) he drops his blood pressure to 60/25. You turn the halothane off and his blood pressure recovers, with 6mg of ephedrine, which you have sensibly drawn up preinduction. A better anaesthetic technique in this situation is to use intermittent doses of ketamine and although the surgeon grumbles about the poor abdominal wall relaxation, he is well maintained with boluses of 0.5mg/kg given as clinically indicated every 20 minutes or so. We’ve probably under-resuscitated him pre-induction and he is much more stable after 2000ml 0.9% saline and 500ml colloid.
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/