Covid-19

This tutorial follows on from Management of Sepsis – part 1 (TOTW 27/06/2005). For more detailed discussion of current strategies in the management of sepsis visit the Surviving Sepsis website at http://www.survivingsepsis.org/hcp_index2.html
MCQ self assessment
State whether the following statements are true or false:
- Strategies proven in randomised controlled studies to reduce mortality in sepsis include:
- Administration of activated protein C
- Administration of low dose steroids
- Managing the patient in the semi-recumbent position
- Maintenance of the patient’s blood sugar level between 4.4 and 6 mmol/l
- Liberal transfusion to maintain a haemoglobin level above 10 g/dl
- Regarding enteral nutrition (EN):
- It should be commenced on admission to the ICU in almost all patients
- Total parenteral nutrition (TPN) is safer than EN
- EN should ideally be established within 72 hours of admission to ICU
- EN protects against peptic ulcer disease
- EN may reduce the incidence of sepsis
- A lung-protective ventilation strategies includes:
- High positive end-expiratory pressure (PEEP)
- Use of volume-controlled ventilation (VCV), which achieves a lower peak airway pressure than pressure-controlled ventilation (PCV) for the same tidal volume
- A large (10-12 ml/kg) tidal volume to avoid atelectasis
- Maintenance of strict PaCO2 control to avoid acidosis
- An inspiratory to expiratory (I:E) ratio of greater than 1:2
- Renal replacement therapy (RRT) is indicated in the following situations:
- Pericardial effusion caused by uraemia
- Acidosis
- Hyperkalaemia
- Oliguria
- pH 7.05 in a septic patient with oliguria
- Activated protein C:
- Should be given to all patients with sepsis
- Is cost-effective
- May cause coagulation abnormalities
- Is effective in patients with APACHE II scores less than 25
- Lowers mortality by 6.5% if given to appropriate patients
Therapeutic strategies for improve oxygen delivery and preserving organ function.
Organ failure results from inadequate organ oxygenation caused by poor perfusion. In addition utilisation of oxygen is compromised by impaired mitochondrial function. Strategies to maintain or restore organ function are general, aimed at improving delivery of oxygen and nutrients to all tissues, or organ-specific (e.g. the kidney and gut). Oxygen delivery to the tissues (DO2) is defined as:
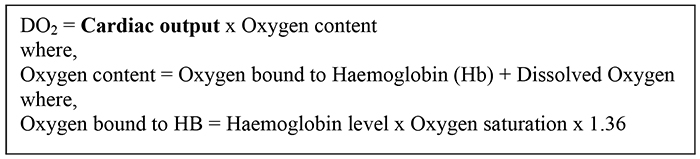
In order to improve oxygen delivery, the cardiac output and the oxygen content of the blood (i.e. the Hb level and the oxygenation of haemoglobin) should be optimised.
General strategies
Optimising cardiac output
- In Systemic Inflammatory Response Syndrome (SIRS) the cardiac output may be low, high or normal.
- A normal or supra-normal cardiac output maintains oxygen delivery, however some organs (particularly the kidney and brain) require maintenance of a minimum perfusing blood pressure. Most organs are capable of some autoregulation but this mechanism cannot always compensate for the circulatory disturbance in sepsis. For this reason a vasodilated patient with a high cardiac output but a low blood pressure usually needs intervention to elevate their blood pressure.
- The main treatments for maintaining cardiovascular function are correction of hypovolaemia with fluid therapy, inotropes and vasopressor agents. This should be instituted promptly as soon as sepsis is diagnosed.
Correction of hypovolaemia (fluid therapy).
- Vasodilation causes blood to pool in the periphery (relative hypovolaemia) and abnormal capillary permeability results in fluid leak into the tissues (absolute hypovolaemia).
- Monitor progress clinically: a satisfactory response to fluid therapy is suggested by a falling heart rate, increase in the blood pressure, decrease in the capillary refill time and improvement in organ function.
- A central venous catheter may be helpful to guage the response to fluid administration. However in many situations central venous pressure measurements are poor indicators of intravascular ‘filling’, and should be interpreted in light of the patient’s clinical assessment.
- Clear benefits of colloid over crystalloid have not been demonstrated, but crystalloid redistributes rapidly into the whole extracellular volume (about 14 litres in a 70 kg man) and so larger volumes must be given for intravascular resuscitation.1
- In anaemic patients blood is often required, but current evidence suggests that haemoglobin levels down to 7g/dl are well tolerated in the critically ill.2
Use of inotropic and vasopressor (vasoconstrictor) agents
- If the blood pressure remains low after the patient is judged to be adequately intravascularly filled, the patient has septic shock.
- This results from either inadequate myocardial ‘pump’ function or from a degree of vasodilation which cannot be overcome by fluid therapy alone, or commonly an element of both.
- If the patient appears vasodilated with a hyperdynamic circulation an agent with vasopressor properties (i.e. an α-adrenoreceptor agonist), such as noradrenaline (norepinephrine), is appropriate to elevate the blood pressure.
- If the patient is cool peripherally (has a large core to peripheral temperature difference), has signs of poor organ perfusion and/or a low blood pressure then an agent with more positive inotropic properties is the best choice. Examples are adrenaline (epinephrine), dobutamine or dopamine.
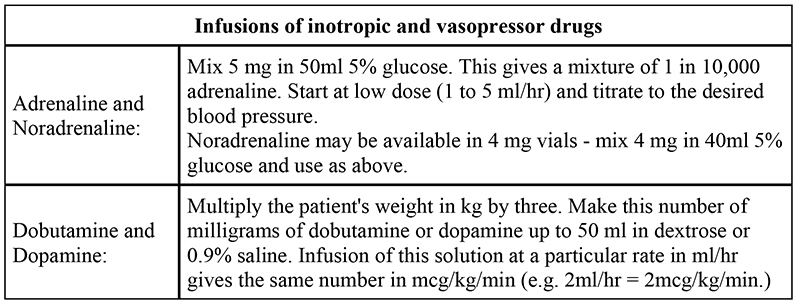
- Inotropes should be given through a central venous catheter and direct intra-arterial blood pressure measurement is preferable for accurate, continuous readings. Proposed regimens for use of these drugs are shown below. In practice few of these drugs have ‘pure’ effects. Noradrenaline also has positive inotropic effects via stimulation of β1- adrenoreceptors, which gives it advantages over pure vasopressors such as phenylephrine, which may reduce stroke volume and cardiac output by increasing the afterload of the heart. Combinations of vasopressor and inotropic drugs (e.g. dobutamine and noradrenaline) are often used.
- If the clinical picture is difficult to interpret, other means of investigation are available in some centres. Pulmonary artery flotation catheters (Swan-Ganz catheters) indirectly measure the left atrial pressure, which may be a more accurate measure of intravascular volume status. The saturation of blood sampled from the pulmonary artery gives the mixed venous blood oxygen saturation which can be used to assess adequacy of oxygen delivery. Use of trans-oesophageal doppler is increasing. Other non-invasive guides to organ perfusion include blood lactate and the saturation of central venous blood (SCVO2).
Oxygen content and gas exchange
- Up to 40% of patients with severe sepsis develop problems with gas exchange, namely ‘Acute Lung Injury’ (ALI).
- ‘Acute Respiratory Distress Syndrome’ (ARDS) describes the most severe form of ALI. Capillary leak causes pulmonary oedema which compromises oxygenation and CO2 elimination. ALI may resolve with treatment of the underlying cause of the SIRS, or progress to a stage where lung fibrosis occurs.
- Steroids may have a role in the treatment of late refractory ALI / ARDS, but are thought to be ineffective in the early stages.3
- Mechanical ventilation may exacerbate lung damage since excessive inflation pressure may cause over-distension and damage of the alveoli (‘volutrauma’). In patients with ALI, a ‘protective’ ventilation strategy should be employed:4,5
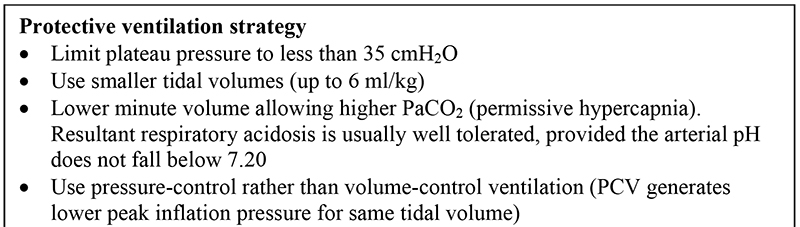
- Ventilator-associated pneumonia (VAP) is a frequent complication of ventilation. This is thought to arise from contamination of the respiratory tract by micro-aspiration of material regurgitated from the stomach around the endotracheal tube cuff. Techniques which are thought to reduce the incidence of VAP include:
- Aseptic technique when suctioning patients
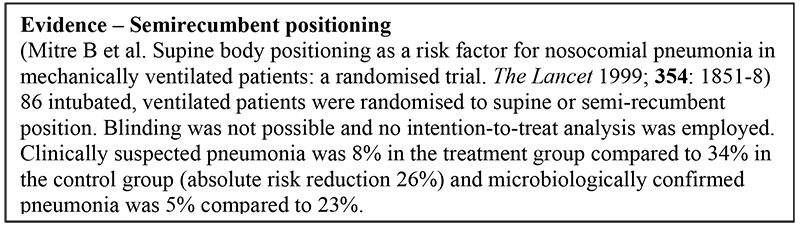
- Nursing the patient semi-recumbent (sitting at 30-45°) instead of completely flat (see box)
- Avoiding the use of proton-pump inhibitors or H2- antagonists which encourage bacterial growth in the stomach due to loss of acidity. Early nasogastric feeding helps to prevent gastric mucosal damage.
- Ensuring that the cuff of the endotracheal tube is correctly inflated
- Avoiding re-intubation or manipulation of the airway circuit
Treatment of anaemia
- Studies show that transfusion of blood to critically ill patients to maintain a haemoglobin level of greater than 10 g/dl does not alter the patient outcome.1
- With the multiple potential problems associated with blood transfusion, in the absence of ischaemic heart disease, it is reasonable to allow the haemoglobin to remain at 7 to 9 g/dl.
Organ-specific strategies
Gastrointestinal tract
- The bowel may act as the ‘motor’ for multiorgan dysfunction syndrome (MODS), by the mechanism of bacterial translocation across damaged mucosa, whose integrity has been damaged by hypoxia. As described above, early enteral feeding is the main preventative measure to counter this.
- H2-antagonists (e.g. ranitidine) and proton pump inhibitors (e.g. omeprazole) have been used to reduce mucosal damage in patients who cannot be fed enterally. The disadvantage is that by reducing gastric acidity these drugs allow bacterial overgrowth and may increase the likelihood of ventilator associated pneumonia and bacterial translocation. Sucralfate is a cheaper alternative which gives some mucosal protection without reducing gastric acidity.
Liver
- In the acute phase of sepsis (within the first 24 or 48 hours) the liver may be damaged by periods of low blood pressure, reflected in sharp rises in circulating liver enzymes (lactate dehydrogenase and both aspartate and alanine transaminase). With adequate resuscitation this damage is self-limiting and reversible.
- Maintenance of liver function depends on effective resuscitation, rapid removal of the septic focus, appropriate antibiotic treatment, early nutritional support and the avoidance of further damage. Hepatic damage may cause encephalopathy, coagulapathy and hypoglycaemia.
Renal function
- The ion channels in the tubular epithelium of the renal medulla are energy (and therefore oxygen) dependent and so particularly sensitive to episodes of hypotension and hypoxia.
- Up to 65 % of patients with sepsis develop abnormalities of renal function and if renal replacement therapy (haemofiltration, haemodialysis or peritoneal dialysis) is required the mortality is above 50%.
- Indications for renal replacement therapy include severe or refractory hyperkalaemia, severe metabolic acidosis, low or absent urine output or symptomatic uraemia (e.g. pericardial effusion).
- If a patient is oliguric, consider the following:
- Exclude obstructive causes – flush the urinary catheter, consider urethral damage in trauma.
- Fluid resuscitation. Reduction in blood volume stimulates the release of renin, anti-diuretic hormone and activation of the sympathetic nervous system, reducing the volume of urine produced by the kidney. These effects may be reversed by adequate fluid resuscitation, guided clinically and, if necessary, using a central venous catheter. 0.9% saline is the fluid of choice since sodium containing solutions increase the glomerular filtration rate – distal tubule sodium concentration feeds back to glomerulus causing increased filtration.
- Blood pressure. The kidney autoregulates the filtration pressure in the glomerulus by altering the resistance of afferent and efferent arterioles. Autoregulation fails if the mean arterial blood pressure falls below about 60 mmHg and urine flow decreases or stops. Correction of hypovolaemia may not restore the blood pressure. Use an inotrope or vasopressor as described above.
- Nephrotoxic agents. Stop non-steroidal anti-inflammatory drugs, angiotensin-converting enzyme (ACE) inhibitors and avoid radiographic contrast media. Levels of aminoglycoside antibiotics (gentamicin, netilmicin) and vancomycin should be monitored.
- Diuretics. Loop diuretics such as frusemide may establish a diuresis but should only be used after optimal restoration of intravascular volume. By inhibiting the active transport of ions in the loop of Henle loop diuretics may offer some protection to tubular cells from hypoxic damage.
- If these strategies do not restore urine flow, then acute renal failure has occurred. In the absence of specific nephrotoxic agents the cause is likely to be acute tubular necrosis, which in most cases is reversible.
- In impending renal failure, dopamine infusion does not affect mortality or the likelihood of progression to acute renal failure.6
- The time to return of renal function is variable (from a few days to several weeks) and in the interim some form of renal replacement is necessary to control hypervolaemia, acidosis, hyperkalaemia and uraemia. The choice is largely dependant on local availability and transfer to another centre may be necessary. Monitor the patient using daily weight, and measurement of electrolytes, urea and creatinine.
Hormonal changes and glucose control
- Insulin secretion is reduced with the stress of severe illness whilst cortisol and growth hormone secretion both increase. Patients are prone to hyperglycaemia due to the insulin-antagonism of these hormones, endogenous catacholamines and drugs such as adrenaline (epinephrine).
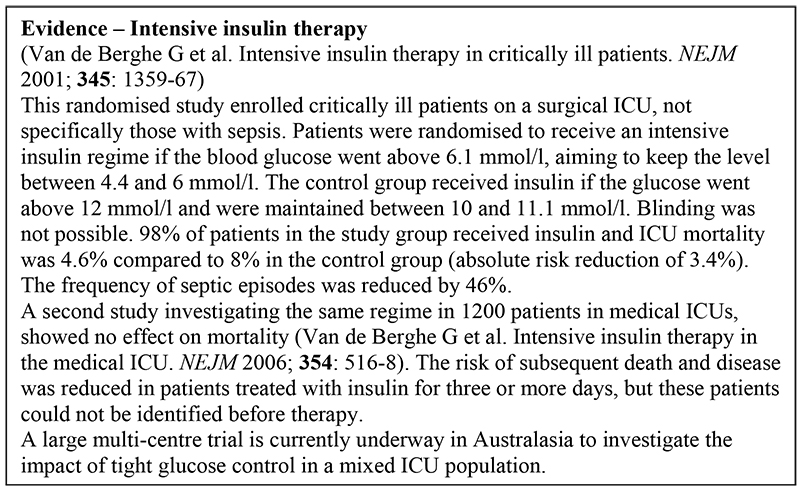
- Ideally an intravenous infusion of short-acting insulin (1 unit per ml) should be used to maintain blood sugar levels between 4.4 and 6 mmol/l. In some settings this may not be achievable and a goal of 5 to 9 mmol/l may be necessary.
- Where IV infusion is not possible use intermittent subcutaneous injections of insulin (e.g. Actrapid 4-6 hourly). Check the blood sugar at regular intervals.
Nutrition
- Under the influence of the hormone changes of the stress response critically ill septic patients become catabolic, breaking down their own tissues (especially muscle) to use as metabolic fuel. This process cannot be reversed, but can be limited to some extent by supplying the patient with appropriate quantities of energy (in the form of fat and carbohydrate), nitrogen (in the form of protein, peptides or amino acids), minerals and vitamins.
- Feeding via the enteral route (e.g. via a nasogastric tube) is easier and cheaper than parenteral (intravenous) nutrition; further proposed benefits of enteral feeding include reduced ‘stress’ ulceration in the stomach, preservation of bowel mucosal function and reduction of bacterial translocation from the bowel lumen into the circulation.
- However, there is still no definitive evidence showing clear outcome advantages for enteral nutrition (EN) above total parenteral nutrition (TPN).
- Early (within 72 hours of admission) compared to late enteral feeding is widely advocated, but again there is not clear evidence for this.
- Some conditions preclude enteral feeding (recent bowel resection) but other problems may be overcome (e.g. nasojejunal tube for pancreatitis or percutaneous gastrostomy for oesophageal disease).
- TPN may be used if EN is not possible, but is expensive and associated with a number of significant complications (most notably infection).
Anti-inflammatory agents in sepsis
- Evidence from animal models suggests that death in sepsis occurs due to over- stimulation of the immune system. It was thought that blocking the immune response would reduce mortality, however early attempts to utilise anti-inflammatory agents in sepsis were unsuccessful (high dose corticosteroids, antiendotoxin antibodies, tumour necrosis factor (TNF) antagonists, interleukin-1–receptor antagonists).
Coagulation homeostasis and sepsis
- There are areas of overlap between the homeostatic mechanisms controlling coagulation and inflammation, with certain of the endogenous modulators of coagulation also having anti-inflammatory actions.
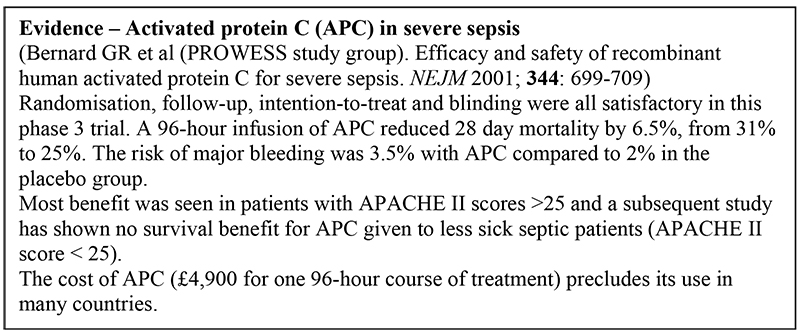
- One such modulator, activated protein C, is the first anti-infammatory agent shown to reduce mortality in sepsis.
Monitoring the patient’s progress
- Failure to improve or deterioration at any stage should prompt thorough reassessment of the patient (ABC, history, examination etc).
- Consider whether the original diagnosis is correct, a new diagnosis has evolved, the current treatment is appropriate and correctly instigated, or whether a complication has developed.
- Signs of deterioration may include:
- Persistent or worsening tachycardia
- Persistently elevated or swinging temperature
- Rising white cell count, C-reactive protein
- Fall in blood pressure, or increased requirement for vasopressor drugs to maintain the same blood pressure
- Deteriorating renal output
- Deterioration in conscious level
- Deterioration in respiratory function
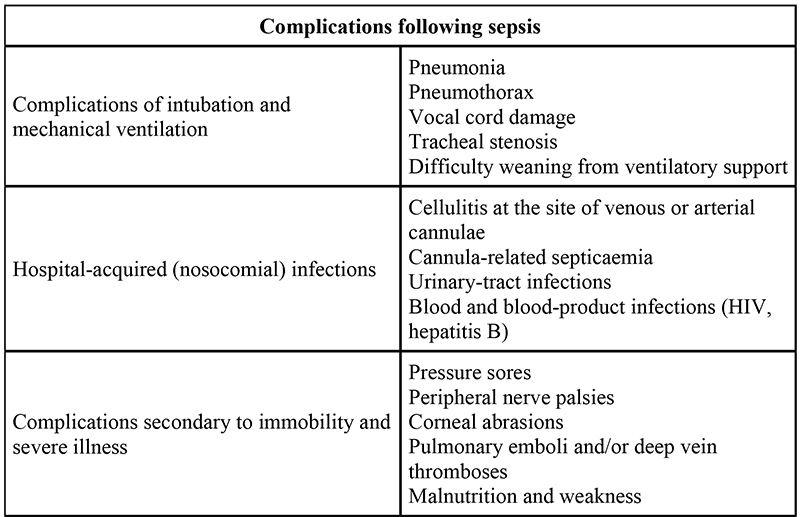
Preventing complications
- Patients with SIRS may suffer depression of immune function and many of the procedures performed on intensive care units breach the body’s natural defences (e.g. orotracheal intubation, peripheral cannulae and central venous cannulae) and leave the patient prone to secondary infections. These and other complications are listed below.

Prevention of Infection
- Medical staff have been implicated in the spread of infectious agents between patients. All staff must wash their hands before and after attending to a patient. Equipment (such as thermometers, stethoscopes, bed pans) should not be shared between patients if possible, but where this is necessary the equipment should be thoroughly cleaned between patients.
- Staff should protect themselves and their clothes from becoming contaminated with biological material by wearing (ideally disposable) aprons and gloves.
- Visitors should be discouraged from moving between patients.
- Patients should be washed daily and never be left in soiled bed linen. Wounds, including drain sites and intravenous cannulae sites, should be inspected, cleaned and dressed at regular intervals.
- Intravenous cannulae and central lines should be removed as soon as practical. Some units have strict protocols governing the replacement of in-dwelling cannulae after a set number of days, whilst other units replace the cannula when clinically indicated.
Immobility and Severe Illness
- Patients immobilised by sedation or severe illness are vulnerable to complications that can be prevented by good nursing care.
- Pressure damage can be prevented by re-positioning the patient every two to four hours, and by replacing wet linen. Particular attention should be paid to the skin over bony prominences, such as the heels and elbows, by padding these areas with cotton- wool, lint or sheep’s wool.
- Eye damage can be prevented by taping the eyes shut or application of protective gel. Joint stiffness and peripheral oedema may both benefit from passive movement of both the legs and arms.
- If there is a severe shortage of nursing staff all of these activities can be carried out by the patient’s relatives if they are given the appropriate training and encouragement. In longer stay patients physiotherapy is essential to minimise muscle wasting and maintain good active and passive range of movement.
- Critical illness neuropathy and myopathy are common complications of SIRS.
Ethical issues and resource allocation
- There is no predictive scoring system which gives accurate predictions of outcome for individual patients. Survival from an episode of severe SIRS/sepsis is dependent on the severity of the acute illness, the patient’s age and previous health and the time delay before the onset of medical intervention, as well as the appropriateness and quality of medical care.
- Few countries have limitless resources, and so difficult decisions face all intensive care doctors when deciding between the potential benefits for one critically ill patient and need for provision of healthcare to several less critically ill patients.
Further reading
- Finfer S et al. A comparison of albumin and saline for fluid resuscitation in the intensive care unit. New England Journal of Medicine 2004; 350: 2247-56
- Hebert PC et al. A multicenter, randomised controlled clinical trial of transfusion requirements in critical care. New England Journal of Medicine 1999; 340: 409-17.
- Meduri GU. Levels of evidence for the pharmacological effectiveness of prolonged methylprednisolone treatment in unresolving ARDS. Chest 1999; 116: S116-118.
- Amato MB et al. Effect of protective-ventilation strategy on mortality in the acute respiratory distress syndrome. New England Journal of Medicine 1998; 338: 347-54.
- ARDS Network. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. New England Journal of Medicine 2000; 342: 1301-8
- Bellomo R et al. Low-dose dopamine in patients with early renal dusfunction: a placebo-controlled randomised trial (ANZICS Clinical Trial Group). Lancet 2000; 356: 2139-43
Answers to self assessment
- Proven strategies in sepsis:
- True – see text
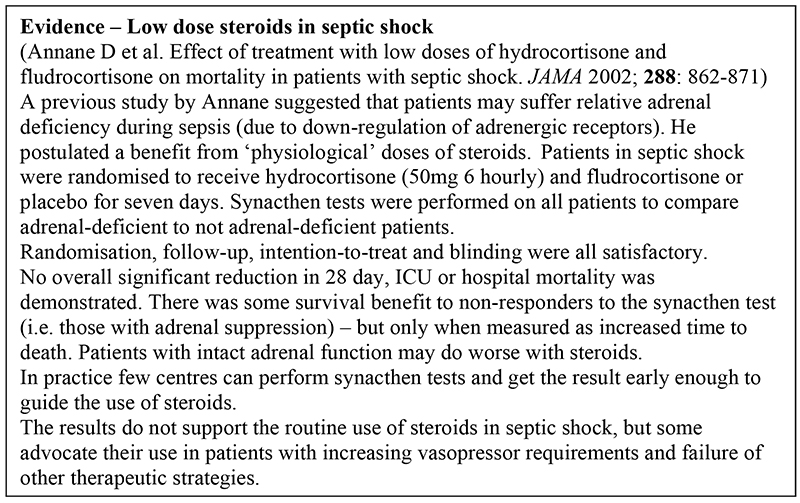
- False – low dose steroids may have a role in the management of severe sepsis and septic shock, but the evidence is not clear-cut. (See Annane paper above).
- False – however this strategy does reduce the incidence of nosocomial pneumonia and all critically ill patients should be managed in the semi- recumbent position
- True – there is good evidence that mortality is improved in surgical intensive care patients, but not in medical ICU patients. A large multi-centre trial is currently underway in Australasia to investigate the impact of tight glucose control in a more general ICU population.
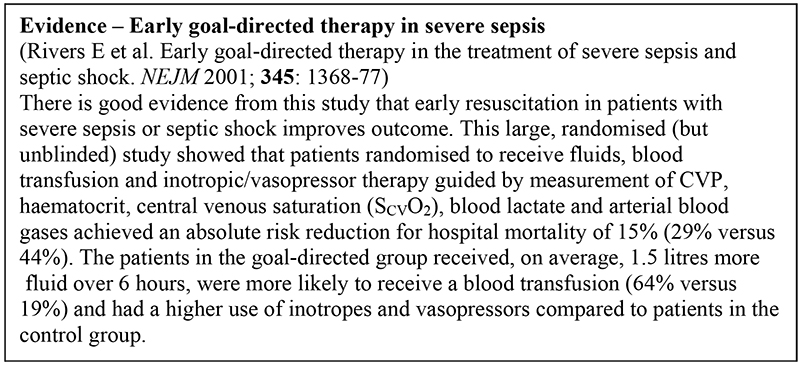
- False – it is acceptable to maintain a haemoglobin level of 7 g/dl or greater. (Reference 2). It is worth noting that early goal-directed therapy in severe sepsis, advocated by Rivers (see text) includes a more liberal attitude to transfusion.
- Enteral nutrition:
- True – see text
- False
- True (probably) – this is a widely-held view, but is currently unproven
- True
- True
- Lung-protective ventilation:
- True
- False – PCV generally achieves a higher tidal volume whilst generating a lower peak pressure than VCV. In addition PCV achieves a higher mean airway pressure and therefore may achieve better oxygenation
- False – use a tidal volume of 6 ml/kg
- False – respiratory acidosis is tolerated (permissive hypercapnoea) as long as the pH remains above 7.20
- True – prolong inspiration to achieve a greater mean airway pressure (I:E ratio of 1:1 or 2:1) which enhances oxygenation.
- Renal replacement therapy:
- True
- True
- True
- False – Oliguria alone is not and indication for RRT, The general condition of the patient will determine whether RRT is commenced – see part e.
- True
- Activated protein C (APC):
- False – Only those with APACHE II scores above 25 have been shown to benefit from APC
- True – according to the National Institute of Clinical Excellence in the UK (www.nice.org.uk)
- True
- False – see part a
- True
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/