Paediatric Anaesthesia

Self assessment:
Before reading the tutorial complete the following questions:
- Describe the differences between exomphalos and gastroschisis? What are the possible treatment strategies?
- What are the signs of circulatory insufficiency in a neonate?
- How would you assess a neonate for surgery?
- What measures can be taken to maintain a neonate’s body temperature
- Discuss the fluid management of a 1 day old, 3 kg neonate undergoing surgery for gastroschisis.
- What is abdominal compartment syndrome?
Introduction
Neonates have special risks associated with anaesthesia and surgery and present great challenges to the surgical team. Ideally, surgery for neonates should be undertaken in a specialist unit.
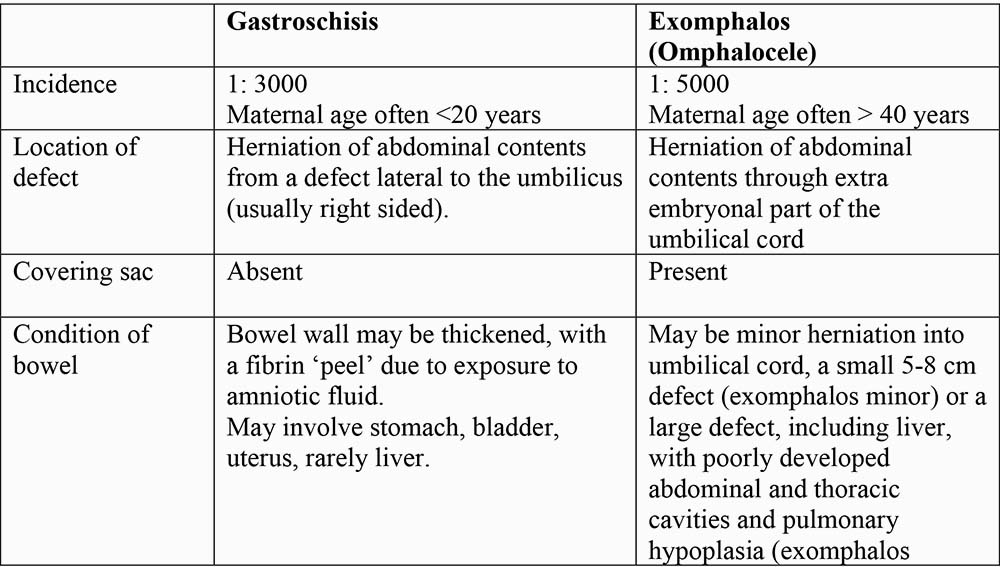
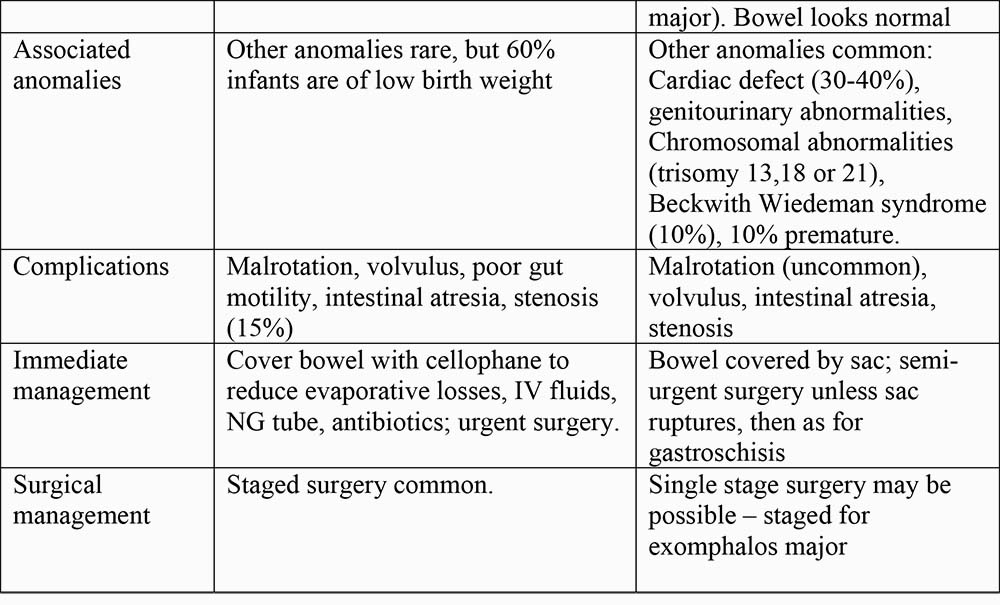
Abdominal wall defects are often diagnosed antenatally and are obvious from birth. Babies should be delivered by elective caesarean section, ideally in a centre where surgery can be performed, or transferred immediately after surgery. Abdominal wall defects may be due to gastroschisis or exomphalos (omphalocele) (see Fig 1). The differences are outlined in the table below:
Surgical Management
- Gastroschisis requires urgent surgery as the bowel is exposed and fluid and heat loss may be significant. There is a risk of fluid and heat loss from the exposed bowel, also of compromised gut circulation with ischaemia and infarction. The initial management involves covering the bowel with wet swabs and occlusive cellophane dressing such as ‘Clingfilm’ to minimise fluid losses and infection.
- Surgery for exomphalos is semi-urgent but ideally should be performed as soon as the neonate is adequately resuscitated. Exomphalos major may be managed conservatively in the developing world, and the abdominal sac allowed to epithelialise. The sac is treated with antiseptic desiccating agents such as silver sulfadiazine ointment or povidone iodine spray (nb may induce hypothyroidism). The sac gradually contracts in size and abdominal wall closure can be attempted at a later stage. Urgent surgery may be required if the covering sac ruptures.
- Single stage surgery with reduction of the bowel and closure of the abdominal wall defect may be possible for exomphalos minor; exomphalos major and gastroschisis generally require staged surgery.
- ‘Abdominal compartment syndrome’ may occur if the abdominal contents are reduced under pressure, particularly in exomphalos major if the abdominal cavity is small. There is an upward shift in the diaphragm interfering with ventilation, and a decrease in abdominal organ blood flow. Reduction in renal perfusion can result in oliguria or even anuria, vascular injury to the intestine may result in gut necrosis and reduction in liver perfusion will result in hepatic impairment. Forceful closure of the abdominal wall will also cause significant tension of the skin resulting in a high incidence of necrosis with secondary infection. If intragastric pressures are > 20mmHg or the inspiratory pressures are > 30cmH2O, staged surgery is required.
- Staged surgery requires application of a ‘silo’ to cover the abdominal contents. The silo is sutured to the edge of the fascial defect. The silo may be made of silastic material or Gortex and must be separated from the bowel contents by interposition of sterile plastic sheeting. Sterile urinary bags and intravenous fluid bags have been used to form an improvised silo. The silo is suspended above the baby and is intermittently ‘tucked’, much as rolling the end of a toothpaste tube. The bowel contents are reduced under gravity over 4-7 days, before definitive abdominal wall closure. The silo is applied under anaesthesia; the child may be extubated soon after surgery and re-anaesthetised for the final abdominal wall closure
- More recently, a preformed, silastic spring loaded silo has been developed for the management of gastroschisis (see Fig 2). The device is inserted and serial reductions are performed on the NICU without any sedation or analgesia and a delayed surgical closure is achieved when the bowel is adequately reduced. This technique prevents the neonate from being exposed to multiple anaesthetics and does not require the baby to be ventilated in NICU. The use of a preformed silo followed by delayed fascial closure in infants with gastroschisis is associated with improved fascial closure rates, fewer ventilator days, more rapid return of bowel function and fewer complications compared with attempts at initial early repair. It would seems to be a technique ideally suited to use for management of gastroschisis in the developing world
Anaesthetic management of a neonate with gastroschisis or exomphalos major.
Preoperative assessment
- Take note of the gestational age, the birth history and whether the baby has had vitamin K. Premature neonates may require surfactant administration. The baby will generally be nil by mouth, but check!
- Airway assessment: difficult intubation in neonates may be associated with micrognathia or abnormal tissues (large tongue in Beckwith Wiedeman syndrome). Babies may be electively intubated for transfer to a specialist centre – check the size and position of the tracheal tube and make sure it is securely fixed.
- Respiratory assessment is essential as respiratory compromise may occur with reduction of the abdominal contents into the abdomen. Exomphalos major is associated with a scaphoid abdomen and small thorax. Respiratory distress may present with signs of increased work of breathing – tachypnoea (normal resp rate 30-40rpm), tachycardia (normal HR 120-180 bpm), and nasal flaring – or apnoea. Check oxygen saturation; distressed infants may desaturate on routine handling. CXR may indicate intrapulmonary shadowing suggesting aspiration of infection; note the position of the tracheal tube and NG tube if present.
- General cardiovascular assessment should be performed. Gastroschisis and ruptured exomphalos major may present with significant fluid loss requiring fluid resuscitation. Assess the baby clinically – skin perfusion, capillary refill (should be instantaneous if the baby is well filled), HR and BP, blood gases if available. Fluid resuscitation may be required – 20ml/kg, reassess and repeat. A baby requiring significant volume resuscitation should be electively intubated.
- Examine the baby for associated abnormalities, especially if an exomphalos is present.
- Cardiac assessment should be performed to exclude associated cardiac defects. Signs to note in the newborn include abnormal pulses (absent femoral pulse in coarctation), low BP, central cyanosis (pulse oximeter), signs of heart failure (poor feeding, excessive weight gain, poor perfusion, tachycardia, tachypnoea, gallop rhythm, hepatomegaly, cardiomegaly on CXR), +/- a heart murmur (but significant lesions may not be associated with a murmur in the neonatal period). Ideally, a cardiological opinion should be sought and a cardiac echo performed.
- Check the weight of the baby
- Check the drug chart and fluid chart. Antibiotic prophylaxis is required (e.g. metronidazole and benzyl penicillin)
Investigations:
- Full blood count and crossmatch of one adult unit of blood.
- Arterial blood gas to assess the adequacy of resuscitation and ventilation. Check u&e.
- Chest X-ray for all infants with cardiorespiratory symptoms
- Echocardiogram
- Renal ultrasound, especially if syndromic
- Head ultrasound scan to exclude intracranial haemorrhage in premature infants prior to surgery.
Preanaesthetic management
- No sedative premedication; consider atropine (may be administered prior to induction)
- Discuss anaesthesia plan with the parents if present – identify any relevant family history and obtain consent for anaesthesia. Parents may be present in the AR, according to local practice.
- There should be a trained anaesthetic assistant.
- Prepare equipment – e.g. size 3.0-3.5 tracheal tube for a term newborn, 2.5 for a premature infant. Straight blade laryngoscope, e.g. Miller blade, infant facemask and Guedel airway. Appropriate breathing system e.g. T-piece and paediatric ventilator. Make sure all drugs drawn up in appropriate dose. A burette should be used for intravenous fluids
- Warm the theatre to 25-26°C – prepare active warming device for the baby (overhead heater, hot air mattress) and for intravenous fluids. Prepare materials to keep the baby well covered. Transfer the baby to theatre in a warmed incubator; minimise exposure of the baby in theatre (remember to keep head covered). Remind the surgeon to keep the bowel covered with warm swabs during surgery.
- Apply monitoring – ECG, BP, saturation, ETCO2 and volatile agent, ventilator alarms, temperature monitoring as minimum; consider intra arterial monitoring, CVP monitoring (baby with gastroschisis usually requires TPN whilst gut function recovers); a manometer line placed in the bladder or stomach if primary closure is contemplated to monitor intra-abdominal pressure.
- Check adequacy of IV access (should be present already). IV access in the upper limbs is preferable as abdominal pressure may restrict venous return temporarily post operatively. Place a second line after induction
Anaesthetic Management
- Induction.
- May sure atropine is drawn up and available. Preoxygenate with 100% oxygen and aspirate the nasogastric tube to decompress the stomach. Use a modified rapid sequence induction with a small amount of an intravenous agent (e.g. thiopentone 2mg/kg); or sevoflurane or halothane. Suxamethonium or atracurium should be used to facilitate intubation. Deep anaesthesia should be avoided.
- Airway management.
- The endotracheal tube needs to be positioned and secured carefully to prevent displacement.
- Maintenance
- Oxygen with air and an inhalational agent is used for maintenance; nitrous oxide is avoided to prevent further bowel distension. Atracurium (0.5mg/kg) is the muscle relaxant of choice as it does not rely on renal or hepatic function for its metabolism. Intraoperative analgesia: fentanyl (3-5mcg/kg) or morphine if postoperative ventilation is anticipated (20- 100mcg/kg). An epidural or caudal catheter requires an experienced anaesthetist but provides very good intra and post operative analgesia and has the added benefit of abdominal wall relaxation. Hepatic clearance of local anaesthetics may be reduced if there is any abdominal compression.
- Intraoperative fluid management.
- Intraoperative fluid should be isotonic – Saline/ Hartmann’s/colloid or blood. Third space losses may be significant – give fluid boluses of 10-20ml/kg and assess clinically – HR, BP, capillary refill, base excess, Hb. Warmed blood should be transfused to maintain the Hb at approx 10-12 g/dl: (4ml/kg packed cells raises the Hb by 1g/dl). Alternatively, transfuse when 10% blood loss has occurred, guided by weighing swabs etc and clinical parameters. The blood volume of a term baby is 80-85ml/kg (90-95ml/kg in preterm). Platelets and FFP are given in 10ml/kg aliquots if the platelet count or coagulation screen is abnormal. Cryoprecipitate is transfused in 5ml/kg aliquots if the fibrinogen levels are low.
- Termination of anaesthesia / emergence
- Some babies with small defects can breathe spontaneously after surgery but the majority require ventilation due to the increased intra-abdominal pressure with compromised respiratory function. All neonates that are able to be extubated should be reversed with neostigmine (50mcg/kg) and atropine (25mcg/kg). Neonates should only be extubated when they are fully awake, with regular spontaneous breathing and vigorous movements of all limbs, well saturated and with stable haemodynamics.
- Postoperative fluid management.
- Fluids should be restricted to 60% maintenance immediately postoperatively – fluid restriction will already be in place if surgery is on the first day of life. Check fluid balance and electrolytes to determine subsequent fluid requirements. 10% dextrose or 4% dextrose 0.18% saline is used initially, but gastrointestinal losses should be replaced with 0.9% saline ml for ml; only isotonic fluids should be used for correction of hypovolaemia. Colloids (gelatins, starch, albumin, depending on local preference) may be used to replace third space losses, including those following placement of an abdominal wall silo.
- Day | Daily maintenance fluid
- 1 | 60ml/kg/day
- 2 | 90ml/kg/day
- 3 | 120ml/kg/day
- 4 | 150 ml/kg/day
- 5 | 150ml/kg/day
- Fluids should be restricted to 60% maintenance immediately postoperatively – fluid restriction will already be in place if surgery is on the first day of life. Check fluid balance and electrolytes to determine subsequent fluid requirements. 10% dextrose or 4% dextrose 0.18% saline is used initially, but gastrointestinal losses should be replaced with 0.9% saline ml for ml; only isotonic fluids should be used for correction of hypovolaemia. Colloids (gelatins, starch, albumin, depending on local preference) may be used to replace third space losses, including those following placement of an abdominal wall silo.
- Glucose control
- Newborn babies less than 48hrs, especially premature, small for gestational age and those born to diabetic mothers are prone to hypoglycaemia. It is important to measure blood glucose levels regularly and to treat hypoglycaemia with 1-2ml/kg of 10% glucose. Some may require a continuous infusion of glucose.
- Continued management in NICU
- Neonates with exomphalos major or gastroschisis may require mechanical ventilation due to temporary deterioration of lung function due to the raised intraabdominal pressure; some may require muscle relaxation for 24hrs. Body temperature needs to be measured and maintained. Analgesia is provided with intravenous morphine or an epidural infusion of local anaesthetic. Paracetamol (10mg/kg) 6 hourly IV/PR should also be administered; note smaller dose in neonates than children.
- A prolonged ileus is expected and total parenteral nutrition is administered until full feeds are established. Despite adequate volume replacement, hypotension may persist, and dopamine infusion is often needed to maintain a normal blood pressure and urine output (if infant severely compromised perioperatively). Early complications include: necrotising enterocolitis, renal insufficiency, pneumonia, patent ductus arteriosus, cellulitis of the abdominal wall, abdominal wall breakdown, gastroesophageal reflux and cholestasis.
Conclusion
Neonates with abdominal wall defects require particular attention to:
- Fluid resuscitation and temperature control
- Overenthusiastic attempts by surgeons to close the defect inevitable causes a decrease in blood pressure and cardiac output and may interfere with ventilation; the surgeon should be alerted and a silo should be placed with a delayed closure.
Further reading
- Berde et al. Anaesthesia and analgesia during and after surgery in neonates. Clin Ther. 2005: Jun; 27(6) 900-21 Review
- Gormky and Crean. Basic principles of anaesthesia for neonates and infants. BJA CEPD Reviews: 2001; (1) 130-133.
- Simon Berg. Paediatric and neonatal anaesthesia. In: Oxford handbook of Anaesthesia Ed Allman K, Wilson I. Oxford University Press, 2nd edition 2006 p757-793
- Ann Black and Angus McEwan. Paediatric and neonatal anaesthesia: Anesthesia in a Nutshell 2005 p64-73.
- Schlatter et al. J Pediatr Surg. 2003 Mar; 38(3): 459-64
Answers to questions
- Describe the differences between exomphalos and gastroschisis? What are the possible treatment strategies? The differences are described in the text. Confusion may arise between gastroschisis and a ruptured exomphalos – but emergency surgery is indicated for both. Treatment strategies include primary closure (small defects), staged closure with silo reduction, use of a preformed silo and staged closure; for exomphalos major with an intact sac, conservative management allowing the sac to epithelialise.
- What are the signs of circulatory insufficiency in a neonate? Tachypnoea, tachycardia, cold peripheries, poor skin perfusion – pale or mottled, with delayed capillary refill; low blood pressure is a late sign. Blood gas analysis may show negative base excess or lactic acidosis.
- How would you assess a neonate for surgery? Described in the text – as for any preoperative assessment but include gestational age, birth history, presenting complaint, associated anomalies, examination of ABC and adequacy of resuscitation.
- What measures can be taken to maintain a neonate’s body temperature. Heat loss may occur by evaporation, convection, conduction and radiation. Evaporative heat loss may be significant. Keep the baby well covered at all times, including during surgery; the head represents a large surface area for heat loss. Cover exposed bowel with warm, saline soaked swabs – use active methods to warm the baby, anaesthetic gases (humidifier) and fluids. Warm the theatre and avoid drafts. Avoid placing the baby on a cold gel pad on the theatre table (huge conductive heat loss).
- Discuss the fluid management of a 1 day old, 3 kg neonate undergoing surgery for gastroschisis. Isotonic fluids are given intraoperatively, giving fluid boluses of 30-60ml saline or Hartmann’s initially, followed by Gelofusine or blood to maintain cardiovascular stability (assess HR, BP, cap refill, base excess) and Hb around 10-12g/dl. Allowable blood loss will depend on the starting Hb. Blood glucose should be measured intraoperatively; if BmStix <3 mmol/l, dextrose should be added to intravenous crystalloid infusion (add 25ml 50% dextrose to 500ml Hartmann’s to give approx 2.5% solution). Fluids should be restricted to 60ml/kg/day postoperatively, and given as 10% dextrose initially – monitor fluid balance and electrolytes. Third space losses should be replaced with colloid (losses may be significant if silo formed), NG losses should be replaced with 0.9% saline ml for ml. TPN is likely to be required from day 2, especially in gastroschisis as gut function may return slowly.
- What is abdominal compartment syndrome? Abdominal compartment syndrome occurs as a result of closure of the abdominal wall defect under pressure – ventilatory insufficiency due to splinting of the diaphragm, reduction in venous return and cardiac output, bowel ischaemia, acute renal failure, acute hepatic failure and skin necrosis. It is associated with high mortality and staged reduction is preferable. Abdominal compartment syndrome is likely with exomphalos major involving the liver, a scaphoid abdominal cavity, and a rise in intragastric or intravesical pressure to >20 cmH2O, or excessive rise in inspiratory pressure.

Figure 1 A. Gastroschisis: bowel bathed in amniotic fluid in utero; thickened fibrin ‘peel’ present

B. Exomphalos minor: bowel covered by sac

C. Exomphalos major involving liver: bowel covered by sac

Figure 2. Traditional surgical silo with sequential tucks

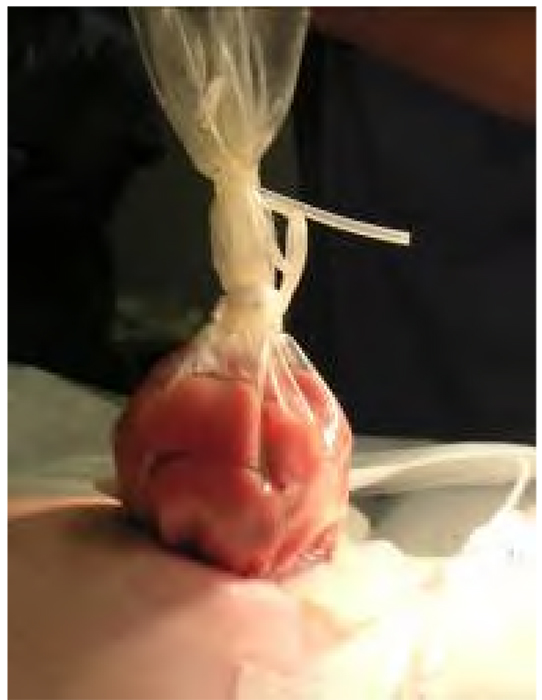
Preformed silo
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/