General Topics

INTRODUCTION
The neuromuscular disorders are a heterogeneous group of diseases effecting skeletal muscle via abnormalities of the motor nerves, neuromuscular junction, cellular matrix, ion channels and metabolic derangements. They are often grouped together in relation to anaesthesia due to common considerations in the perioperative period. An understanding of these disorders is especially helpful in paediatrics where the first presentation of a subclinical myopathy may be under general anaesthesia. Infants presenting for repair of clubfoot, for example, have a high incidence of myopathic changes on muscle biopsy, but may be asymptomatic.
This review will discuss the broad implications of anaesthesia for patients with neuromuscular disease (NMD) and then visit the six main categories of NMD to highlight any specific issues. PLEASE NOTE: Myaesthenia gravis is not discussed in depth in this tutorial as it is covered in detail in aToTW 122 (http://totw.anaesthesiologists.org/2008/12/14/anaesthesia-and-myasthenia-gravis-122/ )
MULTIPLE CHOICE QUESTIONS (True/false; Answers are at the end.)
- Question 1 Common associations with neuromuscular disorders include:
- obstructed sleep apnoea
- autonomic dysfunction
- reduced creatinine kinase levels
- hypothermia
- Question 2 Myotonic spasms may be precipitated by:
- suxamethonium
- change in osmolality
- anticholinesterases
- opioids
- Question 3 At preassessment:
- premedication with benzodiazepines should be avoided due to respiratory depression
- all patients should have a bed in either HDU or ITU
- an ECG is necessary
- a baseline creatinine kinase may be useful
- Question 4 When anaesthetising patients with neuromuscular disorders:
- suxamethonium should always be avoided
- peripheral nerve stimulators precipitate muscle spasm and should be avoided
- inhalational induction is the technique of choice
- masseter spasm is an indication for dantrolene
PREASSESSMENT
Box 1 categorises the NMD into 6 groups and clearly with such varied pathophysiologies one anaesthetic technique does not fit all these conditions. However, some basic principles can be applied to any anaesthetist faced with the challenge of anaesthetising these patients:
- Precise diagnosis. Not always possible as occasionally anaesthesia is required for diagnosis.
- Full discussion with the patient and family members regarding potential risks and benefits of all treatment options
- Thorough preassessment of function and associated conditions
- Anaesthetic strategies and preparation
- Planning post-operative care
It is important to get full functional assessment. Many patients presenting for surgery may appear deceptively healthy having learnt to function within their capabilities. Cardiorespiratory reserve may not be tested with a limited exercise tolerance. Many NMD are associated with cardiac, respiratory, renal and metabolic disorders and these must be actively sought.
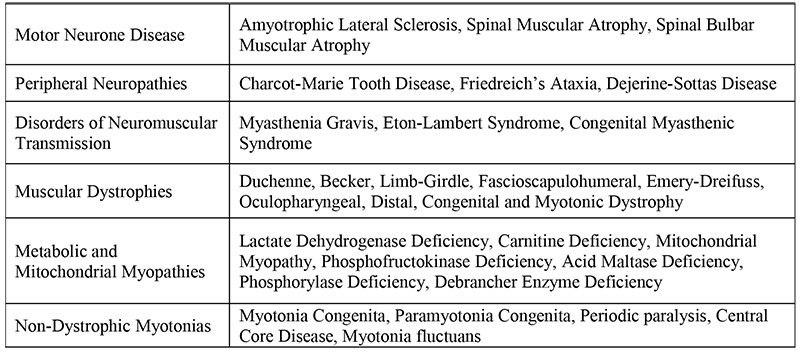
Table1. Classification of Neuromuscular disease
Respiratory
- Dysmorphic features suggesting a difficult airway
- Obstructive sleep apnoea
- Restrictive lung disease from scoliosis
- Respiratory insufficiency secondary to respiratory and pharyngeal muscle involvement
Cardiovascular
- Autonomic dysfunction
- Cardiomyopathy
- Conduction abnormalities due to abnormal conducting tissue or metabolic derangements.
Metabolic
- Na, K, Mg, Cl, Ca may be deranged
- Sustained muscle contraction may cause rhabdomyolysis and a pre-operative baseline urine myoglobin is useful to ascertain postoperatively if there has been any increase.
Investigations
Arterial blood gases, pulmonary function tests, chest X-ray ECG, and an echocardiogram are all extremely helpful in this population.
Premedication
Many of the commonly used premedicating drugs should be used with caution in patients with NMD. Anxiolytic agents can be advantageous in those patients in whom crying and fear can precipitate muscle spasm due to release of catecholamines. If administered, agents causing central respiratory depression or reduce respiratory muscle tone should be given at a reduced dose with close, continuous monitoring.
PERIOPERATIVE MANAGEMENT
The aim when anaesthetising patients with NMD, is a stress free anaesthetic. Increased neuromuscular and catecholamine activity can trigger myotonic reactions and decompensate a dysfunctional cardiorespiratory system.
Monitoring
Oxygen saturation, NIBP, ECG, capnography, minute ventilation, peripheral nerve stimulator and temperature monitoring are all mandatory. Invasive blood pressure monitoring is invaluable in those with an element of autonomic dysfunction and enables regular blood gas analysis for patients with electrolyte disturbances.
Temperature
Patients with NMD are susceptible to both hyperthermia and hypothermia. A predisposition to hypothermia is due to the decrease in heat production by dystrophic or atrophic muscle. However, hyperthermia can also occur due to increased muscle activity as seen in myotonias. There are many well- documented, undesirable consequences of hypothermia but those specific to NMD include triggering of muscle spasms, increased sensitivity to muscle relaxants and aggravation of rhabdomyolysis. Careful monitoring of temperature, both peripheral and core, and the use of forced air blankets, fluid warmers and overhead heating can minimise these complications.
Regional techniques
After a thorough neurological assessment has been documented, regional anaesthesia may be invaluable in this patient population in whom respiratory depression with opiates is disadvantageous. In rapidly progressive disorders however, many will avoid the use of regional techniques as complications of the procedure may be difficult to distinguish from progression of the disease process. In those with cardiovascular complications and autonomic dysfunction, severe hypotension may result from neuroaxial blockade.
Intravenous or Volatile Agents
Intravenous anaesthetic agents can facilitate intubation without the use of neuromuscular blocking drugs and the use of TIVA with short acting agents and opioids can accelerate recovery and reduce postoperative respiratory failure. Some patients with NMD are very sensitive to these drugs and prolonged apnoea and respiratory depression may occur.
Volatile anaesthetics have a cardiodepressant effect by decreasing release of calcium from the sarcoplasmic reticulum, reducing availability of calcium in the myoplasm and decreasing the responsiveness of the contractile filaments to calcium. The sensitisation of the myocardium to catecholamines caused by halothane can precipitate arrhythmias as can the prolonged QT interval caused by isoflurane. These agents have been used widely but should be used with caution.
Neuromuscular blocking drugs
The effect of neuromuscular blocking agents depends on the disease process but, on the whole, suxamethonium should be avoided in all NMD except myasthenia gravis, in whom the dose may need to be doubled. The use of non-depolarising muscle relaxants can often be avoided by judicious use of intravenous induction agents. However, if required, it should be given in reduced doses (10 – 20%) due to increased sensitivity. Atracurium is a popular choice due to its spontaneous Hoffman degradation but the key to muscular blockade is careful titration and close monitoring with a peripheral nerve stimulator (PNS). Neuromuscular block should be checked with a PNS before administration of any muscular relaxants.
COMPLICATIONS
Rhabdomyolysis
Depolarising muscle relaxants can lead to rhabdomyolysis and hyperkalaema in almost all neuromuscular diseases, especially in denervated, dystrophic and metabolically altered muscle. Extrajunctional or foetal isoforms of the acetylcholine receptor lead to widespread membrane depolarisation, hyperkalaemia, rhabdomyolysis and potentially cardiac arrest. Sustained release of calcium from the sarcoplasmic reticulum can also cause hypermetabolism and muscle cell damage and this may be potentiated by volatile anaesthetic agents. Myotonias may spontaneously induce rhabdomyolysis due to sustained muscle contraction and it is wise to measure serum creatinine kinase (CK) and myoglobinuria preoperatively if this is suspected. Features consistent with rhabdomyolysis are: frothy urine, metabolic acidosis, hyperkalaemia, myoglobinuria, CK > 10,000 U/l.
Treatment includes:
- cessation of potentially causative drugs
- correction of life threatening hyperkalaemia
- aggressive volume resuscitation to maintain a urine output > 1ml/kg/hr
- urine alkalinisation with sodium bicarbonate
- monitoring of liver enzymes, coagulation, blood gases, electrolytes and glucose.
- occasionally Dantrolene may be helpful in hypermetabolism, especially if hyperthermia is present
Respiratory Complications
Respiratory failure is the most common cause of death in patients with NMD. Complications are related to:
- involvement of bulbar muscles causing repeated aspiration and chronic insufficiency
- respiratory and pharyngeal muscle involvement
- higher incidence of OSA in affected children
- progressive spinal deformities causing restrictive defects
Pulmonary function tests and arterial blood gases may be very useful preoperatively to assess the level of dysfunction. Administration of respiratory depressants in the perioperative period can lead to acute decompensation and respiratory insufficiency in recovery is not uncommon. Premature extubation must be avoided, especially in those with a difficult airway secondary to anatomical abnormalities. Intensive care may be required postoperatively to allow time for respiratory depressants to be eliminated.
A careful balance between prolonged postoperative intubation to protect the airway and the inherent loss of respiratory muscle tone during this period is difficult. Effective postoperative physiotherapy and CPAP are invaluable tools in this group with low lung volumes and in whom avoidance of atelectasis, poor cough and respiratory infection are paramount.
Cardiac Complications
Cardiomyopathy and cardiac conduction abnormalities are common in many neuromuscular disorders, with death secondary to cardiac arrest being the second most common cause of death in this patient group. Dysfunction is often silent as the patient often has a very limited exercise tolerance. Identification of conduction abnormalities or limited reserve may warrant preoperative treatment or alteration of the anaesthetic plan.
Perioperative stresses or anaesthetic agents may precipitate cardiac dysrhythmias or cardiac failure. Echocardiograms are helpful but awareness of unpredictable responses to fluid boluses, vasopressors and ionotropes are still possible and careful titration of these drugs is required.
Autonomic Dysfunction
Autonomic dysfunction is not uncommon in NMD and can be responsible for severe hypotension on induction or after regional anaesthesia. Gastric stasis may also present as aspiration if not anticipated.
Diagnosis may be difficult but the possibility of autonomic impairment must be suspected and sympathomimetic drugs available. Response to these agents may be exaggerated due to sensitisation of alpha and beta adrenoreceptors.
Myotonic Reactions
Myotonic contraction is caused by repetitive action potentials leading to a permanent sodium influx or reduced chloride efflux across the muscle membrane. This then renders the membrane hyperexcitable. Myotonic reactions can be caused by:
- suxamethonium
- anticholinesterases
- opioids
- alterations in temperature
- acidosis
- shivering
- change in osmolality
Preventative measures for myotonias may include maintaining a serum potassium of 4.0 – 4.5mmol/l and a diet generous in complex carbohydrates to lessen stiffness. In hyperkalaemic periodic paralysis thiazides, acetozolamide and sodium restriction may be therapeutic .In the event of a myotonic reaction the precipitant should be sought and corrected. Drugs that cause a use- dependent block of sodium channels (class one antiarrhythmics) are the treatment of choice: mexiletine, tocainide.
Masseter spasm is an example of a common myotonic reaction that can occur in patients with NMD. Spasm of muscles may be caused by increased electrical stimulation as in myotonia, by uncontrolled release of calcium from the sarcoplasmic reticulum as in Malignant Hyperthermia (MH) or impaired reuptake of calcium as in Brody’s Disease. Although masseter spasm does not always herald the onset of MH, all children that present with this sign should be treated as if a MH crises may follow.
Malignant hyperthermia
There has long been a hot debate as to whether patients with NMD have an increased susceptibility to MH. Some suggest that just three myopathies; Evans myopathy, King Denborough syndrome and Central Core Disease are predisposed to MH, while others believe all myopathies are at increased risk. It is possible that the tests used in the diagnosis of MH may be affected by the electrical after-activity in myotonia, and increased resting myoplasmic calcium in myotonic dystrophy interfering with the diagnosis. However,there have been cases of increased muscle injury and metabolism after prolonged inhalational anaesthesia in patients with myopathy and it is therefore advisable to have a low threshold for suspicion of MH. Irrespective of the pathophysiology of the muscle injury, close monitoring as described earlier is recommended in all patients with NMD and prompt treatment of electrolyte disturbances, acidosis, hyperthermia and myoglobinuria is essential. Dantrolene has been used for hypermetabolism not associated with MH to good effect.
Postoperative Care
Extubation should not occur until the patient is able to maintain adequate tidal volumes and airway reflexes have returned, as respiratory failure and aspiration are common. Post-operatively careful monitoring must be continued and there is a low threshold to manage these patients in a high dependency or intensive care environment.
Hypoxia, hyperkalaemia, rhabdomyolysis, electrolyte disturbance, hypothermia can all have catastrophic consequences in the post-operative period and should be monitored closely. A urine dip for myoglobin or serum CK may be sent to assess level of muscle injury.
SPECIAL CONSIDERATIONS
Motor Neurone Disease
Motor Neurone Disease (MND) is a degenerative impairment of the motor neurones. It is most commonly sporadic, but can also be hereditary or infectious in origin. MND can affect the lower motor neurones, upper motor neurones or both. The result is denervation of the skeletal muscle leading to spasticity or atrophy depending on the location of the abnormality.
The main problems for the anaesthetist involve respiratory insufficiency, poor cough and bulbar dysfunction leading to aspiration. Over-expression of the extra-junctional or foetal acetylcholine receptor can then occur over the surface of skeletal muscle resulting in life threatening hyperkalaemia is suxamethonium is used. There may also be increased sensitivity to non-depolarising muscle relaxants. Baclofen, diazepam and dantrolene have all been used perioperatively to control spasticity. Baclofen should not be withdrawn abruptly as it may precipitate a MH- like crisis.
Peripheral Neuropathies
These are an extremely diverse group of NMD and may be associated with a number of conditions such as diabetes mellitus, autoimmune disorders such as Guillian Barre, critical illness, toxic substances, infections and hereditary disease. Characterised by flaccid paralysis, sensory dysfunction and spread of symptoms as in polyneuropathy, a precise diagnosis is the key to planning an anaesthetic in this group.
Cardiac and autonomic dysfunction is common in peripheral neuropathy and cardiovascular lability may be augmented by the use of cardiodepressant anaesthetic agents. A higher degree of atrio-ventricular blocks may require temporary pacemaker insertion perioperatively. Specific associations in this group include the high sensitivity to thiopentone in Charcot-Marie-Tooth-Syndrome and the high incidence of cardiomyopathy in Friedreich’s Ataxia.
Due to the progressive nature of these disorders it may be difficult to distinguish the natural manifestation of the disorder from a complication of regional anaesthesia and for this reason some anaesthetists will avoid regional blocks in some of these patients. Meticulous documentation of preoperative disability and discussion with the patient is mandatory if a regional technique is used.
Disorders of Neuromuscular Transmission
Myasthenia Gravis is the subject of another TOTW and will not be discussed at length here. Suffice to say that uniquely among the NMD, Myasthenia patients can receive suxamethonium, and may in fact need up to double the normal dosage. However, the sensitivity of the motor end plate to non-depolarising agents is elevated. Volatile anaesthetic agents also appear to be safe.
Eaton Lambert Syndrome, however, exhibits the more familiar reaction to muscle relaxants and the dosage of depolarising and non-depolarising agents should be reduced. Drugs reducing neuromuscular transmission such as antibiotics and beta-blockers may enhance muscle weakness and should be avoided.
Muscular Dystrophies
Myotonic disorders
There are three syndromes: Myotonic Dystrophy, Myotonic Congenita and paramyotonica. The most common is Myotonic Dystrophy which is a disorder of chloride conductance characterised by incomplete muscle relaxation; myotonia. Extramuscular features include cardiomyopathy, conduction abnormalities, restrictive lung disease, OSA, delayed gastric emptying, dysphagia, hypothyroidism, and diabetes mellitus.
Muscular Dystrophies
Muscular dystrophies are a group of progressive genetically determined degenerative myopathies. There are several different types, the most commonly known being Duchennes muscular dystrophy.
The basis of the dystrophies is an abnormality (as in Becker Muscular Dystrophy (BMD) ) or absence (as in Duchenne Muscular Dystrophy (DMD)) of the dystrophin gene, leading to a progressive deterioration of the muscle. Dystrophin is a protein that conducts the force of muscle contraction by the anchoring the cytoskeleton to the extracellular matrix. It is also involved in cellular signalling.
Scrupulous attention must be paid to functional assessment in all these patients as respiratory and cardiovascular symptoms correlate poorly with muscle symptoms. There are commonly intra-atrial conduction abnormalities in patients with disorders of dystrophin with 90% have an abnormal ECG. By the age of 14, around one third of patients with Duchenne Muscular Dystrophy have cardiomyopathy. Cardiac arrhythmias may require a temporary pacemaker perioperatively.
Respiratory insufficiency due to weakness of the respiratory muscles is aggravated by the hypersensitivity to respiratory depressant drugs. Fascioscapulohumeral dystrophy affects the accessory muscles of ventilation significantly decreasing vital capacity. Hypoventilation can also be a feature of Limb Girdle Dystrophy where the diaphragm may be affected. Some patients have also shown a reduced compensation to hypoxia and hypercapnia.
Smooth muscle involvement results in dysmotility of the stomach and oesophagus increasing the risk of aspiration. Disturbed glucose metabolism is also common.
In DMD there is over-expression of extrajunctional acetylcholine receptors that can lead to hyperkalaemia and rhabdomyolysis if suxamethonium is used. Similarly anticholinesterases are not recommended due to the potential to causes severe hyperkalaemia. Inhalational anaesthetic agents have also been implicated as a cause of rhabdomyolysis and malignant hyperthermia-like reactions.
Smooth muscle and platelet dysfunction are suggested by some, to cause increased blood loss. Hypovolaemia is poorly tolerated due to stiff myocardium that compensates with an increased heart rate and not increased force of contraction. Attention to perioperative volume status is important and may necessitate the use of invasive monitoring in prolonged procedures and intensive care postoperatively.
Female carriers of mutations to the dystrophin gene show signs of mild myopathic changes and cardiomyopathy and should be treated with caution.
Metabolic and Mitochondrial Myopathies
The pathophysiologies behind the multiple metabolic and mitochondrial myopathies are manifold. In those patients with metabolic disorders, muscle metabolism should be supported by the administration of substrates depending on the disorder such as glucose or amino acids. Aggressive metabolic monitoring in the perioperative period is essential and the generic considerations for all NMD should be applied.
- Acid maltase deficiencies can cause respiratory insufficiency, aspiration pneumonia, pulmonary hypertension, macroglossia, cardiomegally and hepatomegally.
- Lipid storage myopathies are susceptible to hypoglycaemia, acidosis, rhabdomyolysis and cardiac failure.
Mitochondrial myopathies are a similarly diverse group. Most anaesthetic drugs have a depressant effect on the mitochondria and all should be used with care. All patients with a mitochondrial myopathy should have tight glycaemic control in the perioperative period to avoid lactic acidosis. Suxamethonium should be avoided and atracurium appears to be safe at low doses.
Risk of third degree heart block is such that preoperative pacemaker implantation may be advisable and external pacemakers should be available in the theatre. Some mitochondrial myopathies are associated with seizures and require anticonvulsant therapy.
Non-Dystrophic Myotonias and Periodic Paralyses
As with other myotonic conditions depolarizing muscle relaxants are contraindicated. Inhalational or intravenous induction with thiopentone are both acceptable followed by non-depolarising neuromuscular agent. Reversal with acetylcholinesterases should be avoided due to the danger of triggering muscle spasms in patients with myotonic disease. Preoperative stressors and postoperative shivering should also be avoided.
Paramyotonia Congenital and Hyperkalaemic Periodic Paralysis require meticulous attention to avoid hypoglycaemia, which can cause hyperkalaemia and precipitate paralysis. On the contrary, hyperglycaemia, release of catecholamines, fluid infusions and mild hypothermia can all cause hypokalaemia and paralysis in Hypokalaemic Periodic Paralysis.
MCQ Answers
- Question 1
- T
- T
- F (raised)
- T (decreased metabolic rate due to muscle atrophy)
- Question 2
- T
- T
- T
- T
- Question 3
- F (BDZ can be useful with adequate monitoring)
- F (HDU or ITU is not mandatory)
- T (cardiac disease is common)
- T (allows a more informed assessment of a raised postoperative level)
- Question 4
- F (can be used in myasthenia)
- F (PNS are invaluable for guiding muscle relaxant dosage)
- F (induction technique should be weighed up for each individual patient)
- F (suspicion of MH with masseter spasm but dantrolene not automatically indicated)
REFERENCES
- Hayes J, Veyckemans F, Bissonnette B, Duchenne muscular dystrophy: and old anaesthesia problem revisited. Paediat Anesth. 2008 Oct;18(10):1007-8
- Khan Joad A.S, Saxena M.V. Anaesthesia For Myotonic Dystrophy J Anaesth Clin Pharmacol 2005; 21(2): 199-201
- Klinger W, Lehmann-Horn F, Jurkat-Rott K Complications Of Anaesthesia In Neuromuscular Disorders Neuromuscular Disorders 15 (2005) 195-206
- Sambrook P, Schreiber L, Taylor T, Ellis A. The Musculoskeletal System. Churchill livingstone. 2001.
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/