Patient Safety

KEY POINTS
- The occurrence of critical anaesthesia events poses significant challenges, requiring the physician to have a comprehensive understanding of the factors contributing to these incidents.
- Nontechnical skills encompass a broad range of cognitive, social and personal resource skills that complement technical skills and contribute to safe and efficient task performance.
- Anaesthesia crisis resource management is a scientific approach to managing critical events in medical settings where anaesthesia is administered.
- Simulation-based training in nonclinical settings is an effective way to teach nontechnical skills.
- The simulation session should be followed by debriefing by a trained educator to solidify the learning.
INTRODUCTION
It has been a long-held belief that anaesthesia should carry no risk since it is not a therapeutic intervention but rather a facilitator for surgery.1 However, anaesthetic techniques involve the use of potentially dangerous drugs and high-risk procedures. Moreover, management of these drugs and dealing with difficult situations in the perioperative period are core skills required for the practice of anaesthesiology.
The operating room is a dynamic and high-stakes environment where anaesthesia plays a crucial role in ensuring patient safety and well-being during surgical procedures. The occurrence of critical anaesthesia events poses significant challenges, requiring the physician to have a comprehensive understanding of the factors contributing to these incidents.
NEED FOR NONTECHNICAL SKILLS
Critical anaesthetic events encompass a spectrum of unexpected occurrences during anaesthesia administration that may result in adverse patient outcomes. These events can include medication errors, equipment malfunctions, airway complications, cardiovascular instability and anaesthetic-related allergic reactions. By examining critical anaesthesia events, Cooper et al2 found that human errors were a contributing factor in up to 70% of these events. Factors such as wrong-drug usage, faulty anaesthesia machine use, inadequate airway management and inappropriate use of equipment and monitoring devices played a major role in the occurrence of critical incidents.
Anaesthetic practice can be described as ‘hours of boredom interspersed with moments of terror’. It is in these moments of terror that the physician’s swift performance can be crucial for favourable patient outcome. This ability to deal with unexpected and high-stakes situations are the focus of crisis resource management (CRM) training. Taking into consideration that critical events are rare in modern day practice, maintenance of competence in this area is even more important.
There have been many advances in anaesthetic safety in recent years. One particular change has been the integration and recognition of training in cognitive and social skills, collectively known as nontechnical skills (NTS).3
NTS encompass a broad range of ‘cognitive, social, and personal resource skills that complement technical skills, and contribute to safe and efficient task performance’.4 NTS typically include situational awareness, decision making, teamwork, leadership and the management of stress and fatigue5 (Table). Each workspace has its own unique NTS requirements. These skills are universal, but behaviours associated with them are specific to the context in which they are applied.
The inspiration for NTS in anaesthesia is mainly derived from other high-risk work settings, primarily aviation and nuclear technology.6
This tutorial reflects on the relevance of physicians’ competence on NTS and its use in the operating room. Furthermore, it will address how we can improve anaesthesiologists’ training to increase their NTS.
Numerous studies have highlighted the critical role of NTS on crisis prevention in the operating room (OR). Effective communication and teamwork are crucial factors in minimising errors, promoting early identification of potential crisis and initiating appropriate interventions. Research indicates that deficiencies in NTS, such as poor communication or inadequate leadership, increase the risk of critical incidences in the OR.
CRM CURRICULUM
Anaesthesia CRM (ACRM) is a scientific approach to managing critical events in the medical settings where anaesthesia is administered. It involves a team-based approach to identify and manage a potential crisis to minimise patient harm and optimise outcomes.7 This curriculum was first developed by Dr Gaba and his colleagues at Stanford University.8
ACRM focuses on several key principles, including:
- Communication: Clear, closed-loop communication is essential during critical events. An early ‘call for help’ is the most important determinant of the patient outcome in a crisis. Communication failures entail more than the faulty transfer of information.9 They are an interplay of complex individual, relational and systemic factors. Effective communication is more difficult than it looks. The breakdown of effective communication has resulted in retained foreign objects, wrong-sided nerve blocks, mismatched blood transfusion and medication errors.
- Leadership/teamwork: Strong leadership is crucial during a crisis. The ACRM approach encourages team members to take an active leadership role, irrespective of their rank. The role of a leader is to articulate the patient situation clearly to the team, to create a shared mental model, designate the roles and bring the team together.10 It is also important that the leader can delegate appropriate tasks to the team members according to their capabilities to offload the cognitive burden. The leader usually remains ‘hands-free’ to maintain situational awareness and engages in gathering and integrating information. Team trainings should focus not only on nonroutine situations such as emergencies but also on routine situations (eg, routine anaesthesia induction, routine surgery). The observed relationship between teamwork and performance in simulation settings does not differ from relationships observed in real settings.7 A significant association has also been demonstrated between teamwork and objective patient outcomes (eg, postoperative complications, bloodstream infections).
- Situational awareness: Situational awareness involves actively monitoring the environment and anticipating potential problems.11 The ability to anticipate and adapt to changing circumstances has been associated with a decreased likelihood of critical events. Anaesthesiologists should be able to assimilate and synthesise complex information in a rapidly changing high-stress situation. Physicians establish situational awareness in part through information available from displays, direct observation and communication with the team. Situational awareness also includes having appropriate knowledge of and being able to use all available resources during a crisis, including personnel, equipment supplies and cognitive aids.
- Dynamic decision making: During a crisis, quick and informed decision making is paramount. The ACRM approach encourages a shared decision-making process, in which all team members contribute their knowledge and expertise.12 A complex chain of events with many contributing factors may lead to an adverse patient outcome. Several triggering factors may generate ‘perturbations’ or ‘problems’—deviations from the desired patient state or planned anaesthetic course, which require professional attention.9 Besides the anaesthesiologist’s own actions, triggering factors can include the patient’s underlying disease, actions of the surgical team and equipment failures. Multiple problem chains may occur simultaneously, triggered either by a single initiating event or by the coexistence of multiple medical problems in the patient. The interaction between problem chains can catalyse or accelerate the evolution to an adverse outcome.
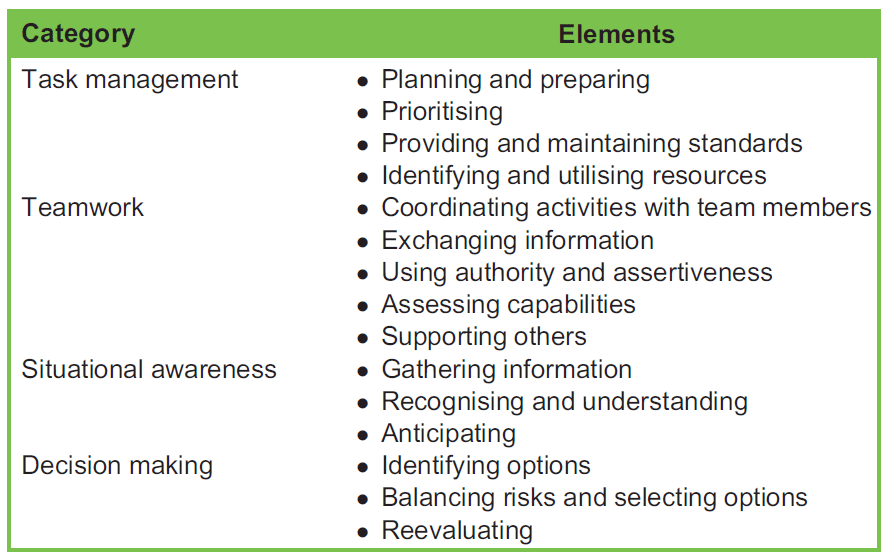
Table. Anaesthetists’ Non-Technical Skills (ANTS) Framework for Nontechnical Skills
Studies have consistently demonstrated that professionals with higher levels of situational awareness and decision-making skills are more likely to detect subtle changes or abnormalities that may indicate an evolving crisis. Moreover, effective communication and teamwork foster an environment where team members feel comfortable speaking up and sharing concerns, leading to prompt recognition of potential crises. Individuals with high NTS proficiency are more likely to implement appropriate interventions, make timely decisions and maintain effective teamwork under stressful conditions. Furthermore, the ability to remain composed, manage stress and prioritise tasks is critical for successful crisis resolution.
Despite NTS having a vital role in anaesthetic practice, these skills have not been part of most anaesthetic training educational curriculums traditionally. In common with other high-reliability industries,6 training programmes are now emerging in medicine. However, properly developed skills frameworks must underpin CRM-style training in medicine.
HOW TO FOSTER NTS EFFECTIVELY IN THE OR TEAMS
Whilst didactic lecture is a traditional way of imparting education in general, the knowledge and use of NTS usually require a more immersive experience. Various training methods can be used for this purpose.
One method to teach NTS is simulation-based training (SBT) in nonclinical settings. SBT is a learner centred, experiential format for fostering the knowledge, skills and abilities needed for highly reliable team interaction. It enables small groups of students to practise in a safe and controlled environment about how to react adequately in a critical patient care situation. Simulations are also useful for creating a reproducible set of examples. This type of training is very valuable for equipping students with technical and NTS before they perform in clinical settings.13 In addition, the use of SBT also has great potential to foster continuing professional education and lifelong learning. Many institutes have created ACRM courses as part of anaesthesia training. The ACRM curriculum usually uses SBT to create a critical event scenario in a lifelike operating room environment that is outside of the actual clinical areas of the hospital. Learners can manage a crisis scenario followed by a debriefing session led by a skilled educator. These sessions can be organised as a part of the curriculum for the anaesthesiology trainees. Common scenarios used in this context include transfusion reactions, undifferentiated shock, laryngospasm, myocardial infarction, arrhythmias, advanced cardiovascular life support management, trauma situations and so forth.
Another effective method of teaching NTS can be creating in situ interdisciplinary OR simulations in actual clinical settings. Regular interprofessional team simulation sessions involving critical OR events are highly recommended.14 The simulated scenarios can address the same crisis as in nonclinical areas simulations. The advantage of delivering in situ simulations as opposed to usual SBT is that it can also help in creating team cohesiveness. Furthermore, training in the in situ setting minimises or removes many of the logistic issues involved in designing and implementing team-based training curricula.8,15
A pivotal part of SBT is debriefing. It is well known that the learning from the simulation sessions must be followed by a debriefing session, ideally immediately after the scenario, to achieve long-term learning. Debriefing is a structured act of facilitated conscious reflection and review of actions taken during the scenario to solidify the learning goals of the simulation scenario. It is a purposeful review of the thought process and actions used and its outcomes. It is a bidirectional, interactive and reflective conversation between the facilitator, participants and, occasionally, observers.15 Various techniques and different frameworks of debriefing are described and have been used in the literature. However, more important than the specific technique used, debriefing should be conducted in a psychologically safe environment.
Despite the demonstrated advantages of the NTS, these skills are not highly valued by many medical professionals. The trainees are imparted with little to no training in these skills. This attitude is now changing because of the increased focus on quality control and the introduction of competency-based training. Education using a simulation modelled on ACRM-type courses followed by debriefing has become widespread among many anaesthesia residency training programs. End-of-residency exams now assess the competency in these skills through the delivery of high-fidelity simulation scenarios. Similarly, most North American anaesthesiology training (residency) programs incorporate simulation-based critical scenarios as an essential educational component and to maintain certification as an accredited anaesthesiology training program.16
The Anaesthetists’ Non-Technical Skills (ANTS) system is a reliable and well-validated tool for measuring NTS.5 It was developed by colleagues at the University of Aberdeen and outlines, in a hierarchical manner, 4 skills categories: task management, team working, situation awareness and decision making. Each skill category is divided into several more specific skill elements that are rated on a scale of 1 (poor) to 4 (good). The scale has demonstrated acceptable interrater reliability and internal consistency, and it has been shown to be sensitive to changes in performance after CRM training.
Ongoing training and education prepare team members for potential crises and to improve overall patient safety. It is necessary to recognise that NTS should not be considered in isolation. Appropriate knowledge of both technical skills and NTS is essential for obtaining the best patient outcomes.
SUMMARY
The literature indicates a strong relationship between NTS and the occurrence or adequate management of crises in the OR. Recognising the importance of NTS and incorporating them into training programs and assessments can contribute to enhanced patient safety, improved outcomes and a culture of continuous improvement in the OR setting. The significance of NTS does not end with residency training. Good NTS are essential to maintain the high standards of patient care in day-to-day practice.
REFERENCES
- Macintosh RR. Deaths under anaesthetics. Br J Anaesth. 1949;21(3):107-136.
- Cooper JB, Newbower RS, Kitz RJ. An analysis of major errors and equipment failures in anesthesia management: consid- erations for prevention and detection. Anesthesiology. 1984;60(1):34-42.
- Flin R, Patey R, Glavin R, Maran N. Anaesthetists’ non-technical skills. Br J Anaesth. 2010;105(1):38-44.
- Flin R, O’Connor P, Crichton M. Safety at the Sharp End: A Guide to Non-technical Skills. Aldershot (UK): Ashgate; 2008.
- Fletcher G, Flin R, Mcgeorge P, Glavin R, Maran N, Patey R. Anaesthetists’ Non-Technical Skills (ANTS): evaluation of a behavioural marker system. Br J Anaesth. 2003;90(5):580-588.
- Crichton MT, Flin R. Identifying and training non-technical skills of nuclear emergency response teams. Ann Nucl Energy. 2004;31(12):1317-1330.
- Holzman RS, Cooper JB, Gaba DM, Philip JH, Small SD, Feinstem D. Anesthesia crisis resource management: real-life simulation training in operating room crises. J Clin Anesth. 1995;7(8):675-687.
- Gaba DM, Howard SK, Fish KJ, Yang G, Samquist FH. Anesthesia crisis resource management training. Anesthesiology. 1991;75(3):A1062.
- Sutcliffe KM, Lewton E, Rosenthal MM. Communication failures: an insidious contributor to medical mishaps. Acad Med. 2004;79(2):186-194.
- Rosenman ED, Fernandez R, Wong AH, et al. Changing systems through effective teams: a role for simulation. Acad Emerg Med. 2018;25(2):128-143.
- Gaba DM, Howard SK, Small SD. Situation awareness in anesthesiology. Hum Factors. 1995;37(1):20-31.
- Gaba DM. Dynamic decision-making in anesthesiology: cognitive models and training approaches. In: Evans DA, Patel VL, eds. Advanced Models of Cognition for Medical Training and Practice. Berlin: Springer; 1992:123-147.
- Issenberg SB, McGaghie WC, Hart IR, et al. Simulation technology for health care professional skills training and assess- ment. JAMA. 1999;282(9):861-866.
- Gros E, Shi R, Hasty B, et al. In situ interprofessional operating room simulations: empowering learners in crisis resource management principles. Surgery. 2021;170(2):432-439.
- Arafeh JM, Hansen SS, Nichols A. Debriefing in simulated-based learning: facilitating a reflective discussion. J Perinat Neonatal Nurs. 2010;24(4):302-309.
- Mcivor W, Burden A, Weinger MB, Steadman R. Simulation for maintenance of certification in anesthesiology: the first two years. J Contin Educ Health Prof. 2012;32(4):236-242.
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/