Obstetrics Anaesthesia

KEY POINTS
- Despite formulation of failed intubation drills and equipment advances, the incidence of failed tracheal intubation remains higher in the obstetric population compared with the general adult population.
- Obstetric airway management embraces airway assessment, pharmacologic aspiration prophylaxis, optimal patient positioning, preoxygenation, provision of a secure airway, and contingency planning.
- Failed tracheal intubation should be managed using well-rehearsed algorithms, which include optimisation of rescue techniques to maintain adequate oxygenation.
- Human factors and poor decision making contribute to adverse airway-related events, and measures to acknowledge and mitigate these risks should be incorporated into obstetric airway training.
INTRODUCTION
Obstetric patients are at increased risk of failed tracheal intubation during obstetric general anaesthesia (GA) because of a number of unique clinical, situational, and human factors. Despite widely publicised ‘failed intubation drills’ and advances in airway equipment and techniques, the incidence of failed and difficult obstetric intubation has not changed for more than 40 years and remains higher than in the nonobstetric population.1 While there are no standardised definitions of failed or difficult intubation, a recent literature review, using differing definitions, found an incidence of failed tracheal intubation of 2.6 per 1000 obstetric general anaesthetics (1 in 390) and associated maternal mortality of 2.3 per 100 000 general anaesthetics (1 death for every 90 failed intubations).1 Difficult intubation, also variably defined, has been reported to occur in 1 in 21 obstetric intubations compared with 1 in 50 nonobstetric intubations.2 Consequently, there has been a shift in focus away from efforts to primarily reduce rates of failed intubation toward a greater appreciation of measures to maintain oxygenation and to control associated human factors that may affect delivery of safe airway management. These approaches are described in obstetricspecific airway guidelines published by the Obstetric Anaesthetists’ Association (OAA) and Difficult Airway Society (DAS).3
WHY IS OBSTETRIC AIRWAY MANAGEMENT MORE DIFFICULT?
Anatomical and Physiological Factors
Maternal anatomical and physiologic changes of pregnancy can contribute to airway-related adverse events, with advanced maternal age and associated comorbidities further exacerbating the impact of these changes (Table 1). A 2-year case-control study of failed obstetric intubation found age, body mass index, and Mallampati score >1 to be significant independent predictors of failed obstetric tracheal intubation.4
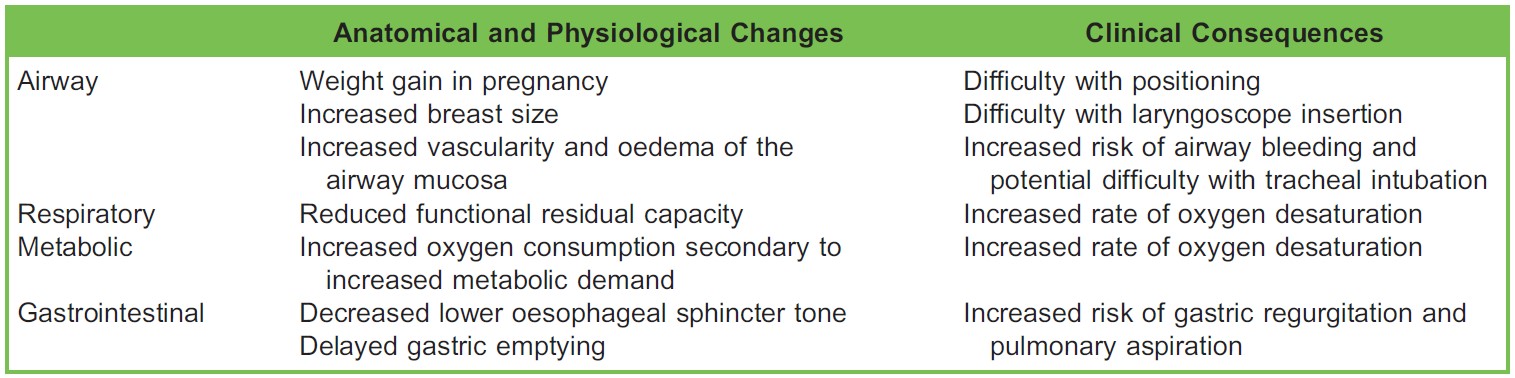
Table 1. Pregnancy-Related Maternal Anatomical and Physiological Factors That May Contribute to Airway Difficulties and Adverse Airway-Related Events
Human Factors
There is increasing awareness of the contribution of situational and human factors to complications encountered during airway management.5 Cognitive load may be increased in the obstetric setting by the unique emotional environment and dual demands of managing maternal and foetal well-being. The declining frequency of obstetric GA in several parts of the world has led to many anaesthetists obtaining limited experience with the technique. Time constraints in the emergency setting may lead to inadequate airway assessment and patient positioning. Knowledge of the increased risk of difficult and failed intubation in this patient group may further heighten anxiety and erode confidence.
PRACTICAL APPROACH TO OBSTETRIC AIRWAY MANAGEMENT
Planning and Preparation for Safe Obstetric GA
Important components of safe obstetric airway management include adequate and timely airway assessment, consideration of fasting status, pharmacologic aspiration prophylaxis, optimal patient positioning, adequate preoxygenation, and provision of a secure airway (typically with an endotracheal tube following rapid sequence induction [RSI] of anaesthesia; Figure 1).
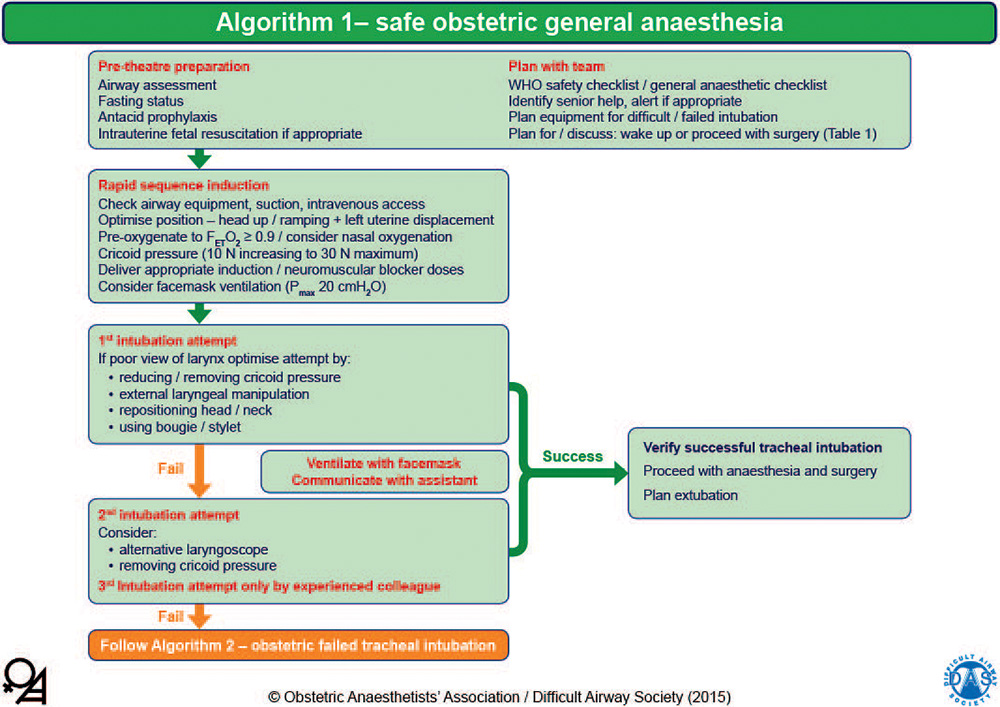
Figure 1. OAA/DAS algorithm 1: safe obstetric general anaesthesia. WHO, World Health Organization; FET O2, end-tidal fraction of oxygen; Pmax, maximal inflation pressure. This algorithm is reproduced with permission from the OAA and DAS and is available online in pdf and PowerPoint formats.2
Airway Assessment
Every woman undergoing obstetric surgery should have a documented airway assessment. This should highlight potential difficulties with tracheal intubation as well as potential difficulties with face mask and supraglottic airway device (SAD) placement and front-of-neck access. Several factors have been identified that may predict airway difficulties in this population (Table 2).
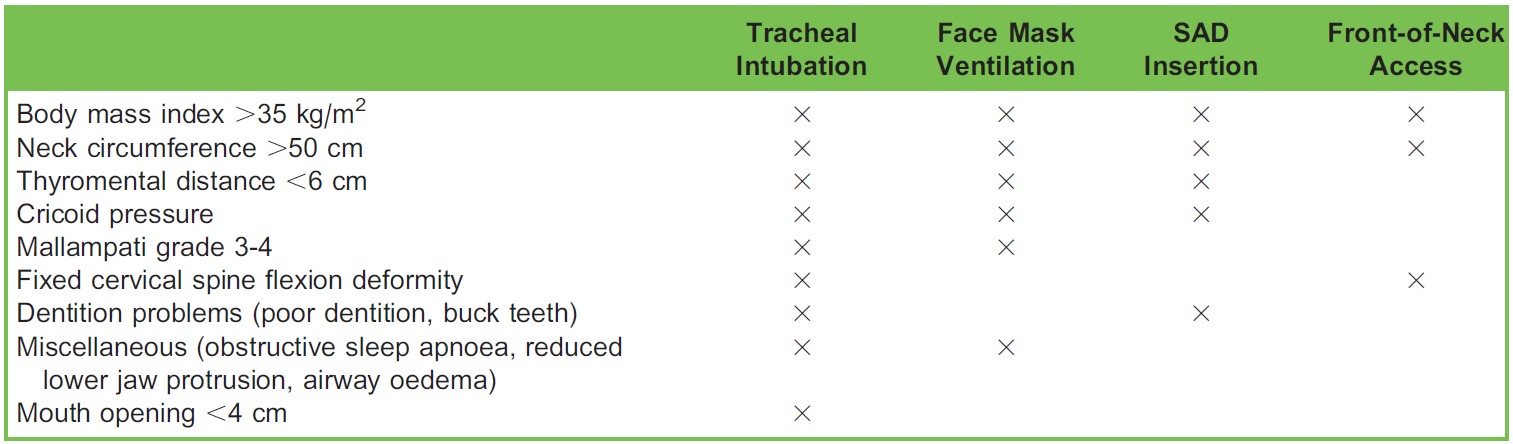
Table 2. Factors That Predict Problems With Tracheal Intubation, Mask Ventilation, Insertion of a Supraglottic Airway Device (SAD), and Front-of-Neck Airway Accessa
Pulmonary Aspiration Risk Reduction
Measures to reduce the incidence of pulmonary aspiration of gastric contents, and to avoid or reduce harm if it does occur, are key components of obstetric GA. Gastric emptying in a nonlabouring pregnant woman is similar to that in a nonpregnant woman; however, gastric emptying is delayed by labour and opioid analgesia. The combination of an H2-receptor antagonist (eg, ranitidine) and an antacid (eg, sodium citrate) has been shown to increase gastric acid pH, thereby reducing the potential harm should pulmonary aspiration occur. The use of point-of-care ultrasound (US) assessment of gastric contents to individualise the risk of regurgitation in obstetric patients has recently been described, but further investigation is required in this patient group.6
Patient Positioning
Optimal patient positioning is essential prior to induction of GA in all patients but especially in pregnant patients. A 20° to 30° head-up position may facilitate insertion of the laryngoscope, improve the view of the glottis, increase functional residual capacity (FRC), and reduce the risk of gastric regurgitation. Aligning the external auditory meatus with the suprasternal notch may be superior to the typical ‘sniffing’ position and is particularly helpful in the obese patient. This ramped position can be achieved with the use of specific equipment (eg Oxford HELP Pillow; Alma Medical, London, UK) or by pillows placed under the patient’s shoulders and head7 (Figure 2).

Figure 2. Head elevated ‘ramped’ position. Reproduced with permission from Oxford University Press: Rucklidge M, Hinton C. Difficult and failed intubation in obstetrics. Contin Educ Anaesth Crit Care Pain. 2012;12:86-91.
Preoxygenation
Effective preoxygenation delays desaturation following induction of GA, especially in the pregnant patient with an already decreased FRC. Denitrogenation is best indicated by end-tidal oxygen fraction (FETO2), and ensuring an FETO2 of ≥0.9 prior to induction is recommended.3 Fresh gas flows of more than 10 L/min and a tight-fitting face mask are required for effective preoxygenation. In an emergency situation, 3 to 4 maximal capacity breaths of 100% oxygen may be as effective as the more commonly adopted 3 minutes of normal tidal breathing.
Currently, there is interest in alternative techniques to provide preoxygenation and/or apnoeic oxygenation during tracheal intubation in both nonobstetric and obstetric patients. Insufflation of oxygen at 5 L/min via nasal cannula may prolong the apnoeic time by maintaining bulk flow of oxygen during intubation attempts. Delivery of high-flow humidified nasal oxygen (also referred to as transnasal humidified rapid insufflation ventilatory exchange; THRIVE) may provide an alternative method of preoxygenation and/or apnoeic oxygenation.8,9 While reports of the effective use of THRIVE in critical care and perioperative settings are increasing, limited data exist in the obstetric population. Gastric insufflation and epistaxis are potential complications of this technique, and further investigation is required prior to recommendations in obstetric GA practice.
It is advisable to palpate and confirm the position of the cricothyroid membrane during preoxygenation in the event supraglottic attempts to secure the airway fail and front-of-neck access is required. US of the neck has recently been shown to accurately aid identification of the cricothyroid membrane and is an emerging skill anaesthesia providers should acquire.10
Cricoid Pressure
The use of cricoid pressure (CP) is controversial. The OAA/DAS airway guidelines recommend application of CP during RSI for an obstetric GA.3 However, because of the limited evidence of its effectiveness in decreasing aspiration and the potential for making airway management more difficult if incorrectly applied, the use of CP has been questioned. Consequently, many guidelines recommend a low threshold to reduce or release CP if it impairs the laryngoscopic view or insertion of the endotracheal tube or if ventilation via a face mask or SAD is impeded.3 If a SAD is required after tracheal intubation fails, CP should be temporarily released during insertion and then reapplied.
Face Mask Ventilation Prior to Tracheal Intubation
Face mask ventilation following RSI has traditionally been avoided because of the fear of gastric insufflation and risk of regurgitation. However, gentle face mask ventilation (maximal inflation pressure <20 cm H2O plus CP) has been recommended in recent guidelines because it may reduce the risk of desaturation and provide an indication of ventilation ability in the event of failed tracheal intubation.3
Elective Use of SADs for Caesarean Section
Tracheal intubation following RSI is generally recommended in the obstetric patient. However, there are a number of reports of the elective use of SADs in fasted patients undergoing elective caesarean section.11 While significant airway-related complications have not been reported in such studies, high-risk women (including those with obesity) were generally excluded.
Direct and Indirect (Video) Laryngoscopy
Direct laryngoscopy using a standard laryngoscope (eg, Macintosh blade) is commonly performed. A short-handled laryngoscope should be available for pregnant women because enlarged breasts may impede insertion of a laryngoscope with a standard-length handle. In recent years, there has been widespread adoption of videolaryngoscopy in many areas of anaesthesia and critical care because these devices usually provide a more optimal view of the glottis than direct laryngoscopes. Consequently, current guidelines recommend that a videolaryngoscope be immediately available for all obstetric GAs.3 Videolaryngoscopy also enables the view to be visualised by the supervising anaesthetist and anaesthetic assistant, and this may improve teamwork and communication. However, tracheal intubation using a videolaryngoscope may sometimes be difficult despite an adequate glottic view, especially when using a device with a hyperangulated blade. There are several types of videolaryngoscopes currently available, and experience with one type does not equate to skill with all. The optimal device is currently unknown.12
MANAGEMENT OF THE ANTICIPATED DIFFICULT AIRWAY
If a patient is identified with predictors of a potentially difficult airway (Table 2), the patient should be reviewed as soon as possible by an anaesthetist so that an airway management plan can be formulated and necessary equipment obtained. If a plan is made for a specific airway intervention performed under controlled conditions (eg, awake fibre-optic intubation [AFOI] prior to elective caesarean section under GA), contingency plans should be considered in the event the woman presents in the after-hours period requiring an emergency intervention or if a labouring patient requires urgent surgery. The plan should be discussed with the obstetric team so that they are fully informed with regard to the anticipated difficulties associated with specific interventions.
A detailed discussion of techniques of AFOI in the pregnant woman is beyond the scope of this article. The oral route for tracheal intubation is recommended over the nasal route because the risk of bleeding from the nose is increased in this patient group. AFOI is more easily performed in a controlled environment with a cooperative patient; therefore, attempting this technique in the often chaotic and stressful setting of an emergency caesarean section can be challenging.
MANAGEMENT OF THE UNANTICIPATED DIFFICULT AIRWAY
If a poor view of the larynx is obtained during the first intubation attempt, measures to improve the view should be performed, which include changing the position of the patient’s head and neck and decreasing, readjusting, or releasing CP. If passage of the endotracheal tube is problematic, then a bougie or stylet and/or an endotracheal tube of smaller diameter should be considered. To decrease the risk of airway trauma, the most experienced anaesthetist present should perform the second intubation attempt. A third intubation attempt can be considered and attempted by an experienced provider only.3 Should these attempts fail, a ‘failed intubation’ should be clearly communicated and further help sought.
Failed Intubation
Following declaration of a failed intubation (verbal communication to all personnel in the operating room including the neonatal team), oxygenation via face mask or SAD should be prioritised with simultaneous consideration of measures to avoid awareness and aspiration, both of which are increased in this patient group. If face mask ventilation is inadequate despite a two-handed (plus oropharyngeal airway) technique, then insertion of a second-generation SAD is recommended because these devices enable drainage of gastric contents and allow for higher inflation pressures.3 CP should temporarily be released during SAD insertion (and then reapplied after placement), which may be facilitated by a laryngoscope. A maximum of two attempts at SAD insertion are recommended to avoid oropharyngeal trauma such as bleeding and/or oedema, which may impair subsequent airway management (Figure 3).
Can’t Intubate, Can’t Oxygenate
If adequate oxygenation cannot be achieved via face mask or SAD, then a ‘can’t intubate, can’t oxygenate’ situation should be clearly communicated (Figure 4). If transitioning to front-of-neck airway access, specialist help should be sought (eg, ear, nose, and throat surgeon and/or intensivist), but their availability should not delay attempts at reestablishing oxygenation. If front-ofneck access is unsuccessful, then cardiac arrest is likely, and maternal advanced life support should be commenced. If return of spontaneous circulation is not achieved in the pregnant woman with a fundal height at or above the umbilicus, then a perimortem caesarean section should be performed.13
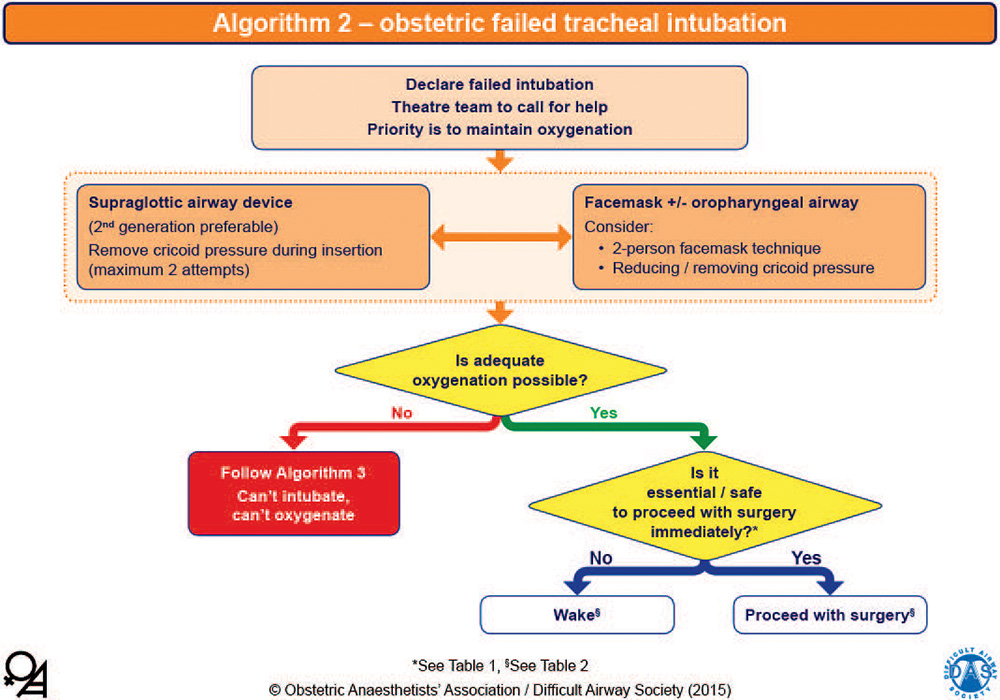
Figure 3. OAA/DAS algorithm 2: obstetric failed tracheal intubation. The yellow diamonds represent decision-making steps. This algorithm is reproduced with permission from the OAA and DAS and is available online in pdf and PowerPoint formats.2
Front-of-Neck Access Techniques
Emergency front-of-neck access can be achieved by either cannula cricothyroidotomy or placement of a wider-bore tube using a scalpel technique. The OAA/DAS obstetric airway guidelines recommend a scalpel cricothyroidotomy technique using the scalpel to make a transverse stab incision through the skin and cricothyroidotomy membrane before placing a bougie into the trachea over which a tracheal tube can be passed. Authors of the DAS nonobstetric guidelines consider this to be faster and more reliable than a cannula technique in the emergency setting.14 However, several cricothyroidotomy techniques have been described, and other guidelines support the initial use of a cannula technique followed by a scalpel technique should the former fail.15 While definitive evidence supporting one technique over another is lacking, performing this procedure in the context of an evolving life-threatening emergency is undoubtedly challenging. Suitable equipment should be immediately available, and all anaesthetists should be trained and competent in this emergency procedure.
To Wake or Proceed With Surgery
Waking the obstetric patient following failed intubation may not always be the optimal course of action if maternal and/or foetal life is at risk should the operation be abandoned. However, in the elective setting, with no risk to either mother or foetus, waking and subsequently proceeding with an alternative anaesthetic technique may be the correct decision. There are a number of factors that influence this decision (Figure 5). Ultimately, the decision will depend on the clinical judgment of the anaesthetist in discussion with the obstetric team, the anaesthetist’s individual skills and confidence, and the evolving situation.16
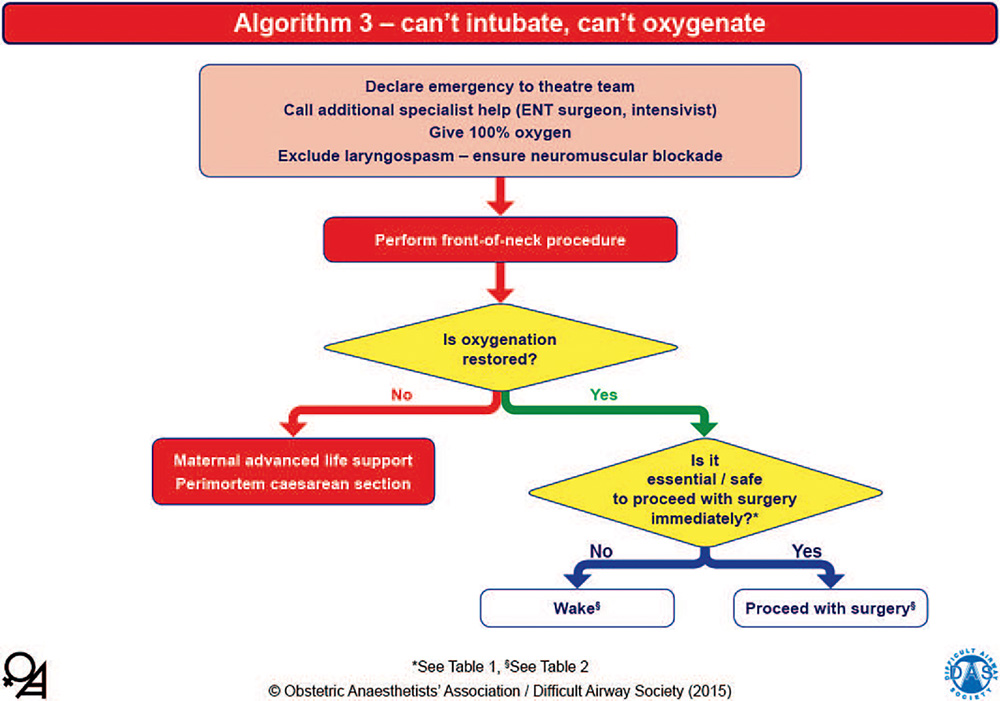
Figure 4. OAA/DAS algorithm 3: can’t intubate, can’t oxygenate. The yellow diamonds represent decision-making steps. ENT, ear, nose, and throat. This algorithm is reproduced with permission from the OAA and DAS and is available online in pdf and PowerPoint formats.2
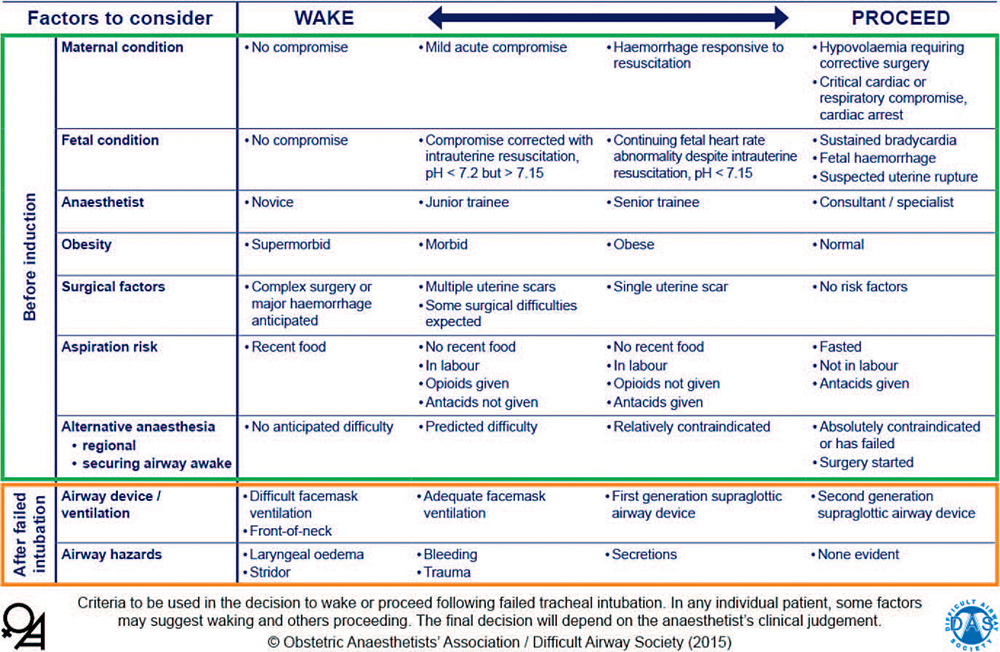
Figure 5. Wake or proceed with surgery? Criteria to be used in the decision to wake or proceed following failed tracheal intubation (table 1 from the OAA/DAS guidelines). This algorithm is reproduced with permission from the OAA and DAS and is available online in pdf and PowerPoint formats.2
Waking a pregnant woman following failed intubation may not be straightforward. In transitioning from the anaesthetised, paralysed state to emergence, there is a risk of airway complications including laryngospasm and pulmonary aspiration. Waking the patient in the supine head-up position is favourable to increase the FRC and improve oxygenation. Subsequent anaesthetic management will depend on several factors, including the urgency of surgery and patient suitability for other anaesthetic techniques such as neuraxial anaesthesia or GA with an AFOI technique.
If the decision is made to proceed with the caesarean section, surgery should be performed by the most senior member of the obstetric team and fundal pressure minimised at delivery to reduce the risk of gastric emptying and/or impairment of ventilation. There are several factors to consider if proceeding with surgery in the nonintubated obstetric patient, including whether to use positive pressure or spontaneous ventilation, maintain neuromuscular blockade, maintain CP throughout the procedure, continue with the current airway device or attempt to intubate the trachea using a SAD as a conduit, and the ideal agent to maintain anaesthesia. Airway management may become easier once the foetus has been delivered because of the decrease in maternal oxygen consumption and reduced intra-abdominal pressure leading to higher pulmonary compliance. It is prudent to use a nonirritant volatile agent such as sevoflurane. The decision to attempt tracheal intubation with a fibre-optic scope using the SAD as a conduit demands careful consideration of whether the benefit of securing the airway with an endotracheal tube outweighs the risk of potentially worsening the clinical situation.
EXTUBATION AND POSTOPERATIVE CARE
Focus on airway management must continue until the patient has recovered from GA and is able to maintain their own airway. The anaesthetist should remain vigilant, and the obstetric patient should be extubated awake in the left lateral or head-up position with full reversal of neuromuscular blockade (if a nondepolarising muscle relaxant has been administered).
TRAINING
Trainee anaesthetists have minimal exposure to obstetric GA in many parts of the world; therefore, simulation-based training is recommended to acquire and maintain skills for difficult obstetric airway management and other high-stakes clinical situations. Cognitive aids and other novel approaches that help clinical teams perform in life-threatening situations have been described.
The vortex approach, designed for use in a developing, time-critical airway emergency, aims to provide a simple and consistent mental model and implementation tool for real-time management of an airway emergency and may be valuable if faced with an evolving obstetric airway emergency.17
SUMMARY
- General anaesthesia in an obstetric patient is often uneventful, but it is associated with a higher rate of difficult and failed tracheal intubation and associated adverse events.
- Greater focus on oxygenation via alternative airway devices and techniques is recommended along with an appreciation of the situational and human factors that commonly accompany an obstetric airway emergency.
- Widespread adoption of videolaryngoscopy is likely to reduce future rates of failed intubation in this patient group.
REFERENCES
- Kinsella SM, Winton AL, Mushambi MC, et al. Failed tracheal intubation during obstetric general anaesthesia: a literature review. Int J Obstet Anesth. 2015;24:356-374.
- McKeen DM, George RB, et al. Difficult and failed intubation: Incident rates and maternal, obstetrical, and anesthetic predictors. Can J Anesth. 2011;58:514-524.
- Mushambi MC, Kinsella SM, Popat M, et al. Obstetric Anaesthetists’ Association and Difficult Airway Society guidelines for the management of difficult and failed tracheal intubation in obstetrics. Anaesthesia. 2015;70:1286-1306.
- Quinn AC, Milne D, Columb M, Gorton H, Knight M. Failed tracheal intubation in obstetric anaesthesia: 2 yr national casecontrol study in the UK. Br J Anaesth. 2012:110:74-80.
- Flin R, Fioratou E, Frerk C, Trotter C, Cook TM. Human factors in the development of complications of airway management: preliminary evaluation of an interview tool. Anaesthesia. 2013;68:817-825.
- Van de Putte P, Perlas A. Ultrasound assessment of gastric content and volume. Br J Anaesth 2014;113:12-22.
- Collins JS, Lemmens JM, Brodsky JB, Brock-Utne JG, Levitan RM. Laryngoscopy and morbid obesity: a comparison of the ‘‘sniff’’ and ‘‘ramped’’ positions. Obes Surg. 2004;14:1171-1175.
- Mir F, Patel A, Iqbal R, Cecconi M, Nouraei SAR. A randomised controlled trial comparing transnasal humidified rapid insufflation ventilatory exchange (THRIVE) pre-oxygenation with facemask pre-oxygenation in patients undergoing rapid sequence induction of anaesthesia. Anaesthesia. 2017;72:439-443.
- Tan PCF, Dennis AT. High flow humidified nasal oxygen in pregnant women. Anaesth Intensive Care. 2018;46:36-41.
- Kristensen MS, Teoh WH, Rudolph SS. Ultrasonographic identification of the cricothyroid membrane: best evidence, techniques, and clinical impact. Br J Anaesth. 2016(suppl 1):117:i39-i46.
- Halaseh BK, Sukkar ZF, Hassan LH, Sia AT, Bushnag WA, Adarbeh H. The use of ProSeal laryngeal mask airway in caesarean section—experience in 3000 cases. Anaesth Intensive Care. 2010;38:1023-1028.
- Kelly FE, Cook TM. Seeing is believing: getting the best out of videolaryngoscopy. Br J Anaesth. 2016;117(suppl 1):i9-i13.
- Jeejeebhoy FM, Zelop CM, Lipman S, et al. Cardiac arrest in pregnancy: a scientific statement from the American Heart Association. Circulation. 2015;132:1747-1773.
- Frerk C, Mitchell VS, McNarry AF, et al. Difficult Airway Society 2015 guidelines for management of unanticipated difficult intubation in adults. Br J Anaesth. 2015;115:827-848.
- Heard AM, Green RJ, Eakins P. The formulation and introduction of a ‘can’t intubate, can’t ventilate’ algorithm into clinical practice. Anaesthesia. 2009;64:601-608.
- Rucklidge MW, Yentis SM. Obstetric difficult airway guidelines—decision-making in critical situations. Anaesthesia. 2015;70:1221-1225.
- Chrimes N. The Vortex: a universal ‘high-acuity implementation tool’ for emergency airway management. Br J Anaesth. 2016;117(suppl 1):i20-i27.
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/