Obstetrics Anaesthesia

KEY POINTS
- The physiological changes of pregnancy have practical implications which can influence the management of an emergent obstetric retrieval.
- Women who require retrieval from remote locations often have a higher risk of adverse obstetric events.
- The most common indication for obstetric retrieval is preterm labour.
- Management of obstetric emergencies in the austere environment may differ significantly from in-hospital treatment and senior advice should always be sought if possible.
- A multidisciplinary approach to obstetric retrieval is mandatory, ideally including a specially trained retrieval nurse or midwife.
INTRODUCTION
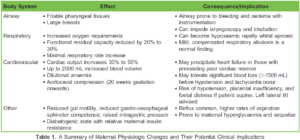
Pregnancy induces significant physiological changes which enable the healthy gestation and birth of the newborn in most women. These changes must be thoroughly understood when providing obstetric care. A summary of changes and potential clinical implications is presented in Table 1.1
Despite these physiologic adaptations, over 800 women die daily from pregnancy and childbirth-related causes, with 94% of deaths from lower- and middle-income countries. A key reason for this is distance to adequate facilities2 which necessitates the need for long-distance transfer of obstetric patients. In some areas of the world, this can be done by aircraft, which adds complexity to already challenging situations.
A recent study on pregnancy-related aeromedical retrievals in Australia indicated that over 90% of patients were retrieved from remote locations with the most common reasons cited as preterm labour (PTL), premature rupture of membranes (PROM), and antepartum haemorrhage.3 The study highlights that many of the women retrieved are more likely to have conditions such as diabetes and preeclampsia with subsequent impact on morbidity, mortality, and requirement for surgical intervention. This demonstrates the importance of timely, pragmatic decision-making in transporting these high-risk patients.3
To help inform these difficult decisions, the authors will use case-based examples of common obstetric problems and their management in the field of retrieval medicine.
CASE 1: PRETERM LABOUR
There is no single internationally acknowledged definition of PTL; however, preterm birth is generally considered to be a live birth before 37 weeks gestation. Threatened PTL is the most common obstetric reason for aeromedical retrieval, and is defined as regular uterine contractions (at least 1/10 minutes) alongside effacement and/or dilatation of the cervix under 37 weeks gestation.3 A suitably skilled and experienced labour and delivery nurse or midwife is an essential member of the retrieval team due to their experience in evaluating PTL.
Rachael, a 27-year-old primigravida with unknown past medical history or antenatal care is approximately 29 weeks pregnant. She has had contractions for 24 hours which are becoming more frequent and painful. She felt a gush of clear fluid presumed to be premature rupture of amniotic membranes earlier that day. She lives in a remote community 400 km from the nearest hospital with obstetric services. The sole clinic nurse is unable to perform a vaginal examination. The retrieval team, based in a city, is 45 minutes away by flight.
PREDEPARTURE MANAGEMENT
The retrieval team, including the coordinating consultant and a senior obstetrician, should discuss Rachael’s case. It is essential to include a nurse or midwife in the retrieval team, and ideally an experienced paediatrician or neonatologist. Rachael may be in active PTL, and the foetus may be more premature than estimated as the gestational age is approximated.
It must be assumed that Rachael could deliver at any stage of the retrieval process. Given the gestational age, evidence suggests it would be preferable to transport the baby in utero, as this increases neonatal survival rates and reduces hospital stays.4 Intravenous (IV) access should be attained, tocolytics administered, and the patient and foetus appropriately monitored while awaiting retrieval team arrival.
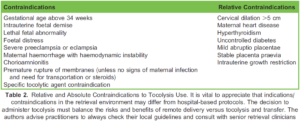
Tocolysis (the use of medications to delay foetal delivery in those with premature labour) could be considered an option assuming no contraindications (Table 2);5 however, numerous factors must be considered when making this decision (Figure). According to a recent meta-analysis, indomethacin appears to be the most effective agent; however, nifedipine was the safest choice and is current first-line therapy.6
The retrieval team should prepare for an emergent delivery at the clinic or in flight. Warming the aircraft cabin, preparing a neonatal resuscitation space, and assembling medications should ideally be completed before meeting the patient. In-flight births are a frightening prospect for everyone involved but fortunately remain extremely rare.7
MANAGEMENT BY RETRIEVAL TEAM
On arrival the nurse performs a vaginal exam on Rachael. She confirms that Rachel is contracting regularly and has ruptured membranes. Her cervix is 5 cm dilated. The foetal heart rate is 150 beats/min.
A multidisciplinary decision is made to initiate tocolysis and transfer to the tertiary centre. Rachael receives 20 mg nifedipine orally alongside a 500-mL fluid bolus to counteract a potential drop in blood pressure that can follow calcium channel blocker administration.6 Betamethasone 11.4 mg intramuscularly (IM) is administered to aid foetal lung maturation as the gestational age is less than 34 weeks.6,7,8 Prophylactic antibiotics are also administered as Rachael’s membranes have ruptured.7 Foetal heart rate is frequently monitored and recorded en route alongside maternal uterine contractions, blood pressure, oxygen saturation, and heart rate.
Rachael safely arrives at the hospital and undergoes a spontaneous vaginal delivery later that evening. The baby is preterm at 30 weeks and is admitted to the neonatal intensive care unit for routine care.
NEONATAL RESUSCITATION
This is beyond the scope of this article. Readers should be aware of and follow their local or national neonatal resuscitation guidelines.
CASE 1: LEARNING POINTS
- PTL is the most common obstetric reason for transporting pregnant women via aircraft.
- An experienced labour and delivery nurse or midwife is an essential part of the retrieval team.

- Liaison with paediatric and senior obstetric staff is highly recommended, especially when deciding whether to deliver remotely or transfer to a hospital.
- The authors’ tocolytic agent of choice is nifedipine and this has been supported by recent evidence. 6 If the administration of a tocolytic is indicated, the following is the suggested regimen:
- Nifedipine 20 mg orally (at least 20 minutes apart) for up to 3 doses can be given within the first hour if contractions persist and the systolic blood pressure is >100 mm Hg.
- Thereafter, nifedipine 20 mg orally may be administered once every 3 hours up to a maximum of 160 mg in 24 hours.
- Steroids and antibiotics may be administered alongside tocolytic agents if deemed clinically appropriate and in consultation with obstetric services, if available.
- Retrieval teams should be familiar with up-to-date neonatal resuscitation guidelines and equipment.
CASE 2: OBSTETRIC HAEMORRHAGE
Obstetric haemorrhage accounts for 25% to 30% of all-cause maternal deaths and is the leading cause of worldwide maternal mortality.9,10 It is classified as antepartum haemorrhage or postpartum haemorrhage (PPH).
ANTEPARTUM HAEMORRHAGE
Antepartum haemorrhage is defined as vaginal bleeding after 24 weeks gestation.9,11 Approximately half of antepartum haemorrhage is caused by either placental abruption or placenta praevia with no clear cause found in the other half.11
Placental abruption is the premature separation of the placenta from the uterine wall, which occurs in about 1 in 80 deliveries. Risk of recurrent abruption in a subsequent pregnancy is increased as much as 10-fold.11 Bleeding from placental abruption may be occult, which can make it difficult to estimate blood loss.11
Placenta praevia describes a placenta that lies partly or completely within the lower uterine segment, potentially covering the cervical os, and occurs in 4 to 5 per 1000 pregnancies. Painless and often mild vaginal bleeding in the second and third trimester is a classical symptom of placenta praevia. The diagnosis is confirmed by ultrasound, and lower-segment caesarean section is the recommended mode of delivery.9
POSTPARTUM HAEMORRHAGE
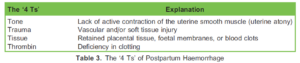
PPH is excessive bleeding following either vaginal or operative delivery. There are 4 main causes of PPH and can be remembered as 1 or more of the ‘4 Ts’ (Table 3).9,12
Normal blood loss has been estimated at up to 500 mL for vaginal delivery and 1000 mL for lower-segment caesarean section.10 While numerous definitions of PPH are described, the World Health Organization defines PPH as blood loss greater than 500 mL in the first 24 hours following all modes of delivery.9 As blood loss can be difficult to quantify, PPH can also be considered as bleeding that produces signs or symptoms of haemodynamic compromise.10 Table 4 categorises blood loss by various clinical parameters.
As obstetric haemorrhage is the leading cause of maternal death,9,10 prompt identification, mobilisation of resources, and treatment is vital to reduce the risk of maternal morbidity and mortality. It is important to note that normal clinical signs in maternal haemorrhage should not be reassuring. The maternal physiology can often tolerate blood loss up to 1000 mL prior to demonstrating signs of hemodynamic compromise. Ongoing bleeding or large volume loss should be promptly identified and treated, to prevent patient deterioration, with treatment escalated if required.
MANAGEMENT OF OBSTETRIC HAEMORRHAGE IN A RETRIEVAL ENVIRONMENT
In the prehospital or austere environment, management options for PPH may be limited. Uterotonics and rapid transfer to a tertiary centre are often the only viable choices. The retrieval specialist may also be involved in delivering blood and expert help to smaller centres.

Alice is a 29-year-old with a history of severe PPH and has just delivered a healthy term baby in a remote clinic. The clinic nurse is concerned as the placenta remains in situ. Alice remains haemodynamically stable but there is ongoing blood loss. Two large-bore IV cannulae have been inserted and an oxytocin bolus has been given. The closest hospital is 1 hour away via fixed- wing aircraft. The retrieval team is activated.
PREDEPARTURE MANAGEMENT
Whilst the retrieval team mobilises, the clinic is instructed to give 1 g tranexamic acid, start an oxytocin infusion at 10 units per hour for 4 hours, start rapid IV crystalloid resuscitation, and ensure body temperature is kept above 36°C.
As with any obstetric retrieval, a multidisciplinary approach is strongly advised, involving members of the retrieval team, remote clinic, and appropriate specialist hospital staff. The retrieval team should include a labour and delivery nurse or midwife.
O-negative blood should be brought on transport, if available, as remote clinics are unlikely to have their own. Excessive crystalloid should be avoided if possible due to the risk of dilutional coagulopathy, oedema, and hyperchloraemic metabolic acidosis secondary to 0.9% saline administration.12 Uterotonic drugs should be considered, drawn up, and clearly labelled whilst in transit (Table 5).12 The WOMAN study demonstrated that tranexamic acid reduces death due to bleeding and advocates its routine use in PPH.13 Uterine massage and bimanual compression may be enough to arrest or delay bleeding in uterine atony but requires the continuous attention of a skilled operator.12
MANAGEMENT BY RETRIEVAL TEAM
As the retrieval team lands, the clinic calls to say Alice is still bleeding and feels unwell. She is pale, tachycardic, but normotensive. The baby is in good condition. As Alice is unstable, the retrieval team decides upon a ‘clinic meet’. A ‘tarmac meet’ is when the patient is brought to the airstrip to await retrieval team collection. This is an approach commonly reserved for stable patients, or time-critical patients who require specific treatment unavailable to the retrieval team. There are risks and benefits to tarmac meet and clinic meet and the decision is not always clear-cut. The decision is best made by multidisciplinary discussion with the retrieval team and other stakeholders such as obstetrics and paediatrics.
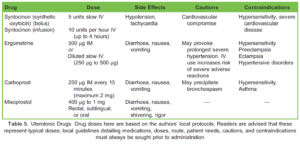
On arrival, they alert the hospital and coordinating clinicians that this is a significant and ongoing PPH. Controlled cord traction to deliver the placenta is attempted by the retrieval team but is unsuccessful. Alice is given a further 5 units IV oxytocin, 250 μg IM ergometrine, and 4 mg IV ondansetron due to the emetogenic effects of ergometrine.12
Controlled cord traction is a viable technique for retained placental removal. A Cochrane review has shown that controlled cord traction reduces the mean blood loss, duration of the third stage of labour, and the risk of requiring an operative, manual removal of the placenta. Despite this, there was no significant effect on maternal mortality and severe morbidity.14 It should, however, be noted that this review looked at in-hospital studies and conclusions drawn may not accurately reflect the inherently hazardous prehospital environment.
Alice is becoming increasingly unwell. Her placenta remains in situ, which is the most likely cause of the haemorrhage, and therefore uterotonics may be of limited use. This austere environment is inappropriate for managing a PPH of this severity and aetiology. The most appropriate decision for Alice is to expedite transfer to hospital.
Two units O-negative blood are administered via a blood warmer during transport to the airstrip. The retrieval team calls to arrange for blood to be brought to the destination airstrip for administration on landing. Members of the obstetric team are alerted and arrange direct access to the operating theatre.
CASE 2: LEARNING POINTS
- Blood loss can be difficult to estimate.
- PPH can occur without warning; uterotonics and O-negative blood should be readily available for all deliveries.
- A tarmac meet may not be appropriate for unstable patients; however, this may prolong the time to definitive care.
- Retrieval teams must be knowledgeable about their local guidelines for PPH management.
- The retrieval team may not be able to stop PPH. Rapid transfer to definitive care may be the most appropriate management option in addition to adjuncts discussed above.
- Additional blood, equipment, and help can be prearranged for receiving bases and hospitals.
CASE 3: PREECLAMPSIA/ECLAMPSIA
Nicole is a primigravid mother presenting to a remote clinic at 38 weeks gestation with severe headache. The clinic notes that she has a blood pressure of 156/94 mmHg and 2+ proteinuria. She is otherwise well. Two large-bore cannulas and a urinary catheter are inserted. The retrieval team is 35 minutes away by helicopter as the nearby airstrip is flooded.
Disorders of hypertension in pregnancy include pre-existing hypertension, gestational hypertension, and preeclampsia. They increase both maternal and foetal morbidity and mortality and are a leading cause of maternal death.8
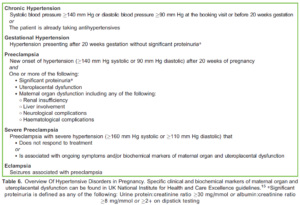
Preeclampsia forms a continuum of disease that can present as, or progress into, severe preeclampsia and eclampsia. Table 6 summarises the key diagnostic criteria.15 Please refer to Anaesthesia Tutorial of the Week tutorials 2, 158, and 304 16,17,18 for more information on these pathophysiologies and their management.
PREDEPARTURE MANAGEMENT
This patient meets the criteria for a diagnosis of preeclampsia, and she has symptoms suggestive of severe preeclampsia.
A conference call is made including the clinic nurse, retrieval team, obstetric clinician, and paediatric clinician. The clinic is advised to administer oral labetalol.
The goal of treatment at this stage is to lower the patient’s blood pressure by approximately 1 to 2 mm Hg every minute.8 Several agents are routinely used for this including labetalol, nifedipine, and hydralazine. Each agent has its own contraindications and interactions that should be carefully considered before administering. Local guidelines should be sought regarding dosages and route of administration.
MANAGEMENT BY RETRIEVAL TEAM
On arrival, Nicole is complaining of a persistent headache and has vomited. Her blood pressure is 152/88 mm Hg and the foetal heart rate is approximately 150 beats/min. All other observations are within normal limits. A second dose of oral labetalol is administered and Nicole is prepared for transfer. While transfer monitoring is being attached she has a seizure. She is placed in the left lateral position, given 15 L/min oxygen via a non-rebreather mask and the retrieval consultant is called for advice.
Eclamptic seizures must be dealt with using supportive measures, which may include intubation and ventilation. Specific first- line medical therapy for an eclamptic seizure is magnesium 4 g IV over 5 minutes. A magnesium infusion running at 1 g per hour for 24 hours should be administered following the bolus, as this reduces the likelihood of recurrent seizures. A second bolus of magnesium 2 to 4 g IV over 5 to 15 minutes can be given if seizures recur.8,15
Whilst receiving magnesium, patients should be monitored for signs of toxicity. Features include muscle weakness, loss of tendon reflexes, respiratory failure, hypotension, prolonged QT interval, and cardiac arrest. For this reason, cardiac monitoring, respiratory rate, and tendon reflexes must be continuously monitored. Ten percent calcium gluconate 10 mL IV over 10 minutes can be administered if magnesium toxicity is suspected or confirmed.8
The seizure terminates within 3 minutes. Airway is patent and there is no suspicion of aspiration. Frequent, non-invasive monitoring is applied and transfer commences.
CASE 3: LEARNING POINTS
- Preeclampsia and eclampsia are a significant cause of maternal deaths worldwide.
- Preeclampsia symptoms are varied but indicate significant disease and risk of progression to eclampsia.
- Lowering the blood pressure is the mainstay of management for preeclampsia. This can be achieved using multiple different agents.
- Magnesium 4 g IV bolus followed by a 1-g/h infusion is the treatment for an eclamptic seizure.
- A second bolus of 2 to 4 g IV over 5 to 15 minutes can be given if seizures recur.
- Magnesium may also be administered for seizure prevention in preeclamptic patients with severe features.
- Patients receiving magnesium should be carefully monitored for signs of toxicity.
SUMMARY
Obstetric transfers represent a clinical and psychological challenge for the prehospital or retrieval clinician. There are many factors to consider when making decisions about treatment and timing of transfer. The clinician can improve their confidence and ability by understanding key points about the nature of obstetric retrievals. Additionally, it is essential to become familiar with the management of the most common causes of obstetric retrievals: PTL, haemorrhage, and preeclampsia. Retrieval practitioners should also be trained and familiar with recognised neonatal resuscitation guidelines. Clinicians must recognise the limitations of the retrieval environment and their own clinical capabilities. Expert help in the form of midwives, labour nurses, obstetricians, paediatricians, and senior retrieval clinicians must be sought for all obstetric retrievals. This multidisciplinary approach improves decision-making in situations where the goal is always to ensure good maternal and neonatal outcomes.
ACKNOWLEDGEMENT
Special thanks to Jodie Martin, Clinical Nurse Consultant, CareFlight, Darwin, Northern Territory, Australia for providing her expertise to this topic.
REFERENCES
- Bedson R, Riccoboni A. Physiology of pregnancy: clinical anaesthetic implications. Contin Educ Anaesth Crit Care Pain. 2014;14(2):69-72.
- World Health Trends in Maternal Mortality 2000 to 2017: Estimates by WHO, UNICEF, UNFPA, World Bank Group and the United Nations Population Division. Geneva: World Health Organization; 2019.
- Gardiner F, Richardson A, Roxburgh C, et al. Characteristics and in-hospital outcomes of patients requiring aeromedical retrieval for pregnancy, compared to non-retrieved metropolitan Aust N Z J Obstet Gynaecol. 2021;61(4):519-527.
- Stephenson JC. Air travel and pregnancy—with reference to obstetric and perinatal aeromedical retrieval. JMVH 2010; 18(2):16-23.
- Mayer C, Apodaca-Ramos Tocolysis. Accessed June 14, 2023. https://www.ncbi.nlm.nih.gov/books/NBK562212/
- Xiong Z, Pei S, Zhu Four kinds of tocolytic therapy for preterm delivery: systematic review and network meta-analysis. J Clin Pharm Ther. 2022;00:1-13.
- Shipway T, Johnson E, Bell S, et A case review: in-flight births over a 4-year period in the Northern Territory, Australia. Air Med J. 2016;35(5):317-320.
- Leslie D, Collis Hypertension in pregnancy. BJA Educ. 2016;16(1):33-37.
- Walfish M, Neuman A, Wlody Maternal haemorrhage. Br J Anaesth. 2009;103(1):47-56.
- Devine PC. Obstetric Semin Perinatol. 2009;33(2):76-81.
- Giordano R, Cacciatore A, Cignini P, et Antepartum haemorrhage. J Prenat Med. 2010;4(1):12-16.
- Plaat F, Shonfeld Major obstetric haemorrhage. BJA Educ. 2015;15(4):190-193.
- WOMAN Trial Collaborators. Effect of early tranexamic acid administration on mortality, hysterectomy, and other morbidities in women with post-partum haemorrhage (WOMAN): an international, randomised, double-blind, placebo- controlled trial. Lancet. 2017;389(10084):2105-2116.
- Hofmeyr GJ, Mshweshwe NT, Gülmezoglu Controlled cord traction for the third stage of labour (review). Cochrane Database Syst Rev. 2015;1(1).
- National Institute for Health and Care UK NICE guideline NG133—hypertension in pregnancy: diagnosis and management. Accessed June 16, 2023. https://www.nice.org.uk/guidance/ng133
- Dalgleish Pre-eclampsia. World Federation of Societies of Anaesthesiologists. 2005;2.
- Hull J, Rucklidge Severe Pre-eclampsia Case Based Discussion. World Federation of Societies of Anaesthesiologists. 2009;158.
- Krishnachetty B, Plaat F. Management of Hypertensive Disorders of Pregnancy. World Federation of Societies of Anaesthesiologists. 2014;304.
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/