Regional Anaesthesia

KEY POINTS
- The obturator nerve arises from the lumbar plexus and provides sensory and motor innervation to the medial compartment of the thigh.
- The obturator nerve divides into anterior and posterior branches, which provide articular branches to the hip and knee joints.
- Obturator nerve blocks are indicated in treating painful adductor spasms and in painful syndromes of the hip and pelvis.
- An obturator nerve block can be used in conjunction with a femoral nerve block for knee arthroplasty to significantly reduce opioid consumption.
- Ultrasound-guided obturator nerve blocks are more reliable than landmark techniques.
INTRODUCTION
The traditional approach of the obturator nerve block was first described by Labat in 1922.1 It is considered a technically difficult block due to wide anatomical variance. In the majority of the population, the common obturator nerve divides into the anterior and posterior branches at the level of the obturator foramen (52%), in the thigh (25%), or the intrapelvic region (23%).2 This has led to a high failure rate for the landmark technique, further contributed by the deep location of the obturator nerve. It may also be difficult to obtain the optimum position of a rotated and abducted leg due to lower limb spasticity. Owing to these difficulties, many clinicians have been reluctant to perform this block. However, the technique has been modified over the years to improve its reliability, make it simpler to perform, and improve patient comfort.3 The 3-in-1 and psoas compartment block were all done with the intent of including the obturator nerve. However, the evidence suggests that it is not always reliably blocked.4 Increasing accessibility and quality of ultrasound equipment has led to a renewed interest in the obturator nerve block.5
ANATOMY
The obturator nerve provides motor function to the muscles of the medial compartment of the thigh, and cutaneous branches innervate the skin of the medial thigh. It originates from the anterior primary rami of L2, L3, and L4 spinal nerves as part of the lumbar plexus. Once formed, it descends through the fibres of the psoas major and emerges from its medial border. It continues to travel posteriorly to the common iliac arteries and laterally along the pelvic wall toward the obturator foramen and enters the medial thigh by passing through the obturator canal, where it divides into the anterior and posterior divisions.
The anterior division enters the thigh in front of the obturator externus. It then descends posteriorly to pectineus and adductor longus and anteriorly to adductor brevis. The anterior division, around the obturator foramen, gives off an articular branch, which innervates the anteromedial capsule of the hip joint. At the lower border of the adductor longus, it gives off a cutaneous branch that innervates the medial aspect of the thigh.
The posterior division enters the thigh by piercing through the anterior part of the obturator externus. It then descends behind the adductor brevis and in front of the adductor magnus. The terminal part of the posterior division forms the genicular branch, which passes through the adductor hiatus and reaches the popliteal fossa, where it pierces the oblique popliteal ligament and then supplies the posterior capsule of the knee joint (Figure 1 and Table).
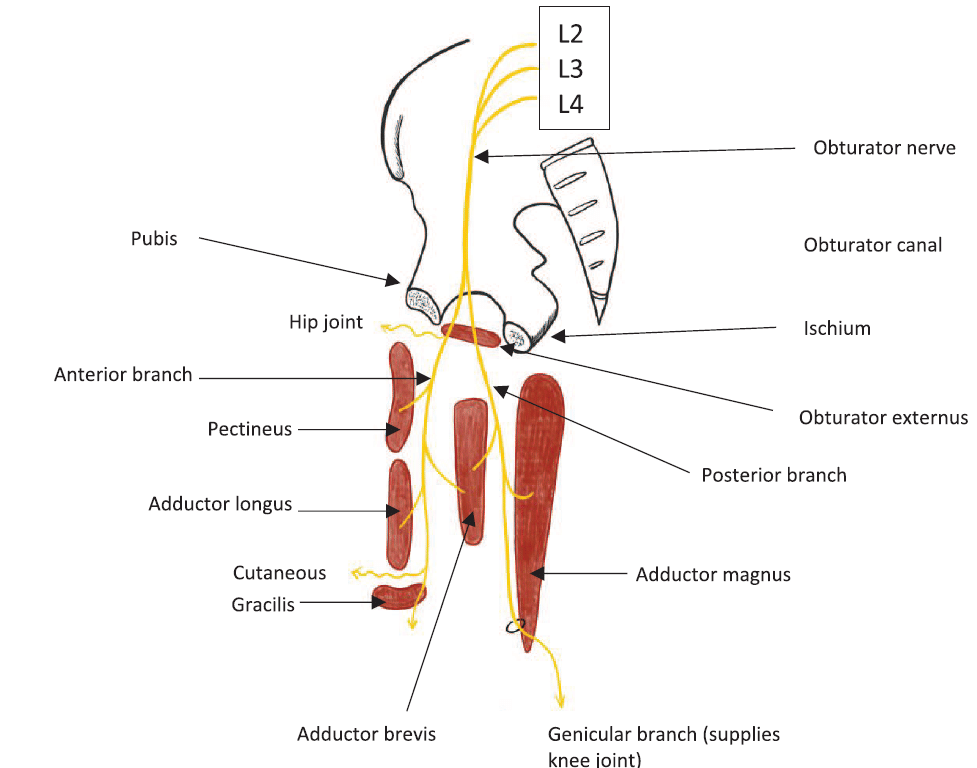
Figure 1. Obturator nerve course from the lumbar spine to the thigh.
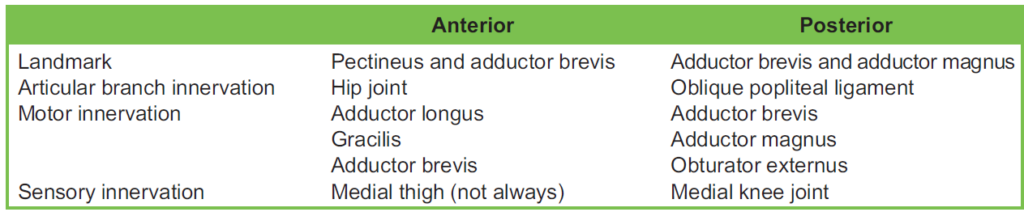
Table. Anterior and Posterior Branches of the Obturator Nerve
INDICATIONS FOR OBTURATOR NERVE BLOCK
Transurethral Resection of Bladder Tumour
The obturator nerve passes close to the bladder wall. In transurethral resection of bladder tumour surgery, electrical stimulation (diathermy) is used for tumour resection. This can cause an “obturator jerk” from stimulation of the obturator nerve. This sudden thigh movement can increase the risk of bladder perforation.6 There are steps that can be taken by surgeons to reduce this risk, such as using bipolar diathermy, reducing the diathermy current, and avoiding overdistension of the bladder. Neuraxial blockade (spinal anaesthesia) does not prevent the adductor muscle spasm. Anaesthetists may consider the use of neuromuscular blockade, which will require general anaesthesia, or selective blockade of the obturator nerve. An obturator nerve block can prevent sudden adduction of the thigh and increase the safety of the procedure.6
Hip Surgery
The hip joint has multiple sensory innervations, and of them, the obturator nerve innervates the anteromedial hip joint capsule. It is unlikely that an obturator nerve block alone will provide sufficient analgesia after hip surgery. A randomised controlled trial demonstrated that a combination of obturator and lateral cutaneous nerve blockade was effective in controlling acute pain after hip fracture surgery.7
Knee Surgery
The knee joint capsule is partially innervated by the obturator nerve. An obturator nerve block can be used in anterior cruciate ligament reconstruction, where there is harvesting of the gracilis tendon. This is because the anterior branch of the obturator nerve innervates the gracilis muscle and can help with pain relief. When an obturator nerve block is performed in addition to a femoral nerve block, it can significantly reduce opioid consumption and pain after total knee arthroplasty compared with a single femoral nerve block or local anaesthetic infiltration.8
Hip Adductor Spasticity
Patients with persistent hip adductor spasticity are at risk of hip joint deformity, scissoring of the hips, and pain, which prevents satisfactory perineal hygiene. This can lead to skin breakdown and infections. Some case studies have shown that obturator nerve block with the addition of a neurolytic agent can be an effective treatment.9
Pain Therapy
Blockade of the obturator nerve can help manage both acute and chronic hip and pelvic pain. Acutely, it is useful for hip and lower medial thigh pain following pelvic trauma and total hip replacement. As the hip joint derives significant innerva- tion from the obturator nerve as well as the femoral nerve, a femoral-obturator nerve block can be used to treat chronic hip pain.
Obturator nerve entrapment has been described in athletes and after pelvic surgery. The obturator nerve has been surgically released with good success. A diagnostic nerve block may be helpful to make the diagnosis.10
LANDMARK TECHNIQUE WITH NERVE STIMULATOR
Classic Pubic Method (Labat Technique)
- Position the patient lying supine and the limb to be blocked abducted 308.
- Palpate to identify the pubic tubercle (Figure 2).
- Using a 22-gauge, 8-cm-long needle, insert the needle perpendicularly to the skin 1.5 cm lateral and caudal to the pubic tubercle.
- Advance until contact with the inferior border of the superior pubic ramus at a depth of 2 to 4 cm.
- After this, withdraw the needle slightly and direct it 458 (cephalad and laterally) to enter the obturator foramen; observe for adductor muscle contraction.
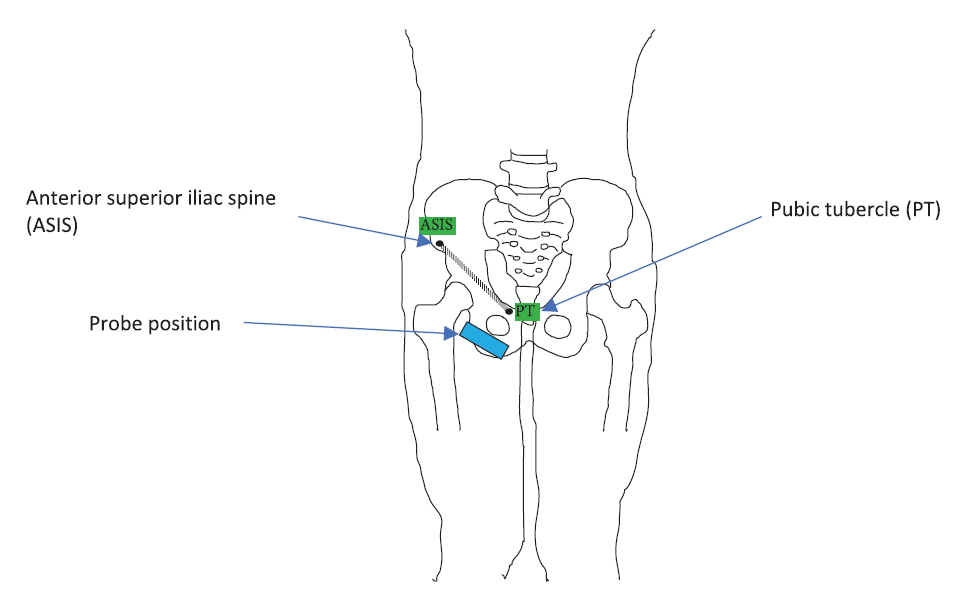
Figure 2. Probe position for the distal ultrasound approach.
- Withdraw the needle and redirect if no contraction is noted.
- When searching with the stimulating needle, initially 1.5 to 3 mA should be sufficient to produce an adductor muscle twitch. Once approaching, the current intensity should be dropped to 0.3 to 0.5 mA.
- Once the adductor muscle contraction is elicited, inject 10 mL of local anaesthetic, with frequent aspirations for blood.
- A reliable block will produce an impaired leg adduction approximately 20 minutes after injection.
Paravascular Superficial Inguinal Approach
- The following need to be identified:
- Tendon of the adductor longus muscle at the pubic tubercle (leg abduction required)
- Femoral artery
- Use an imaginary line drawn over the inguinal fold from the pulse of the femoral artery to the tendon of the adductor longus muscle. Insert a 22-gauge, 8-cm-long needle at the midpoint of this line in 308 cephalad direction.
- Advance the stimulating needle a few centimetres in depth along the adductor longus muscle (you may notice twitching from the adductor longus and gracilis muscles on the posterior and medial aspect of the thigh).
- Insert the needle deeper (0.5 to 1.5 cm) and slightly laterally over the short adductor muscle until a response from the adductor magnus muscle can be visualised on the posterior-medial aspect of the thigh.
ULTRASOUND TECHNIQUE
Ultrasound has been used to identify the obturator nerve, but localisation of the nerve may be difficult and may require confirmation by electrical stimulation. Interfascial ultrasound-guided block has also been described, and success depends on the correct identification of the fascial layers.11 Ultrasound-guided obturator nerve blocks are easier and safer to perform than the landmark techniques. The colour doppler can be used to visualise the obturator arteries located near the nerve branches to avoid puncturing them, although they may not always be visible. The 2 most common ultrasound techniques have been described by Yoshida et al, specifically the distal and proximal approaches.12
Distal
A high-frequency linear probe (12 MHz) is placed just distal to the inguinal ligament and medial to the femoral artery with an imaging depth of 4 cm (Figure 2). The goal is to block the anterior and posterior branch of the obturator nerve individually after they have divided. This is usually medial to the femoral vein. The pectineus, adductor longus, and adductor brevis muscles are easily identified. The branches of the obturator nerves can be seen as hypoechoic circles in a hyperechoic thick layer between the three muscles (Figure 3a,b).
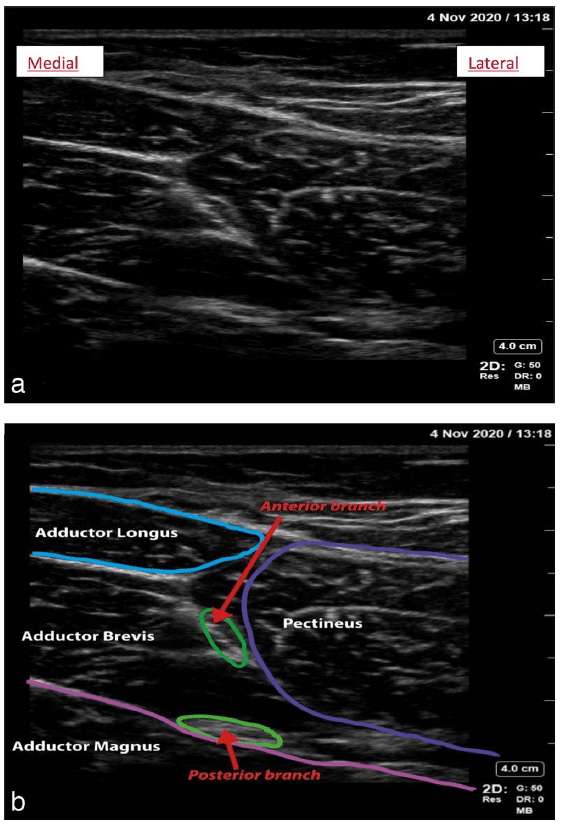
Figure 3. (a) Ultrasound image of the anterior and posterior branches of the obturator nerves. (b) Annotated image showing the muscles and branches of the obturator nerve.
- Position the patient with the leg externally rotated and abducted.
- Use a 12-MHz linear ultrasound probe 1 to 2 cm distal and parallel to the inguinal crease.
- Identify the structures in the femoral triangle (femoral nerve, artery, and vein).
- Move the probe medially to identify the adductor muscle group.
- Use a 22-gauge, 8-cm-long needle (6stimulator).
- Insert the needle in-plane to the ultrasound probe in a lateral-to-medial trajectory.
- Infiltrate 10 mL of 0.5% bupivacaine (or similar); lower concentrations can be used if used in conjunction with other blocks (up to a maximum of 2 mg/kg) between adductor longus and brevis, ensuring interfascial spread to block the anterior division.
- Continue to advance the needle toward the interfascial plane between the adductor brevis and magnus where the posterior division dwells, infiltrating another 10 mL of 0.5% bupivacaine (or similar).
Tip: a nerve stimulator can also be used if the ultrasound visualisation is poor. Contraction of the adductor muscle by stimulation of the anterior obturator nerve is more intense than direct stimulation of the muscles.
Proximal
This technique blocks the common obturator nerve with a single injection. The local anaesthetic is targeted to spread between the pectineus and obturator externus muscles (Figure 4a,b).
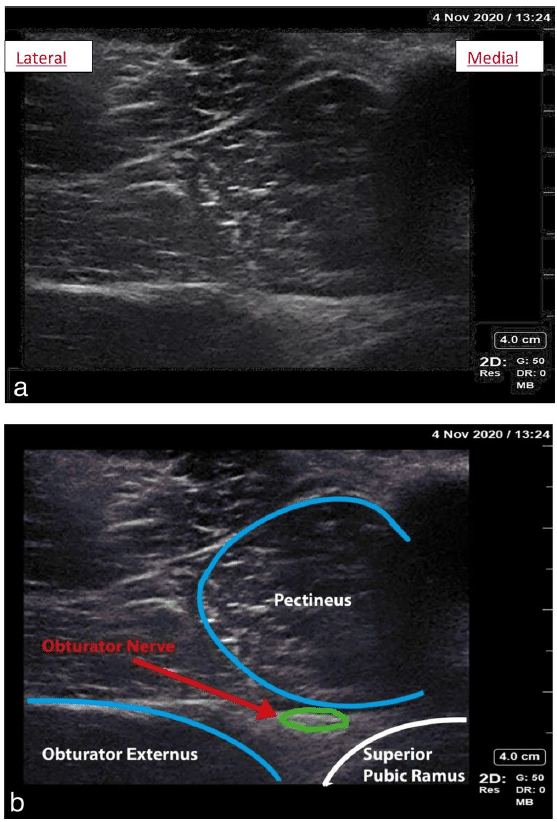
Figure 4. (a) Common obturator nerve. (b) Annotated imaging of the common obturator nerve.
- Align the linear 12-MHz ultrasound probe along the inguinal crease.
- Once the adductor muscle group is visualised, tilt the probe cranially to visualise the inferior margin of the superior pubic ramus.
- The hyperechoic obturator nerve can often be directly visualised between the pectineus and obturator externus.
- If not visualised, an interfascial injection should be sufficient to block the obturator nerve.
- Insert a 22-gauge, 8-cm needle in-plane and infiltrate 10 mL of 0.5% bupivacaine (or similar) up to a maximum of 2 mg/kg.
COMPLICATIONS
The are no reported cases of specific complications related to obturator nerve block. This is, however, likely due to the fact that the block is used infrequently rather than its inherent safety.13 The use of ultrasound guidance may reduce the risk of most common complications of regional anaesthesia, such as blood vessel puncture and inadvertent intravascular or intraneural injections.14
General
- Failure
- Infection
- Bleeding/haematoma
- Pain
- Nerve damage (intraneural injection/nerve ischaemia)
- Intravascular injection of local anaesthetic
- Local anaesthetic toxicity
- Local anaesthetic allergy
Specific
The needle orientation for Labat’s classic pubic method can increase the risk of damage to pelvic structures if advanced too far in the cephalad direction. The “corona mortis” is an anatomical variant. It is a vascular anastomosis between the obturator and external iliac or inferior epigastric vessels. The anastomosis can be venous or both venous and arterial. It is located behind the superior pubic ramus at a variable distance from the symphysis pubis (range of 40 to 96 mm). It is known as the “crown of death” as it is notoriously difficult to achieve haemostasis when injured.15
SUMMARY
The obturator nerve block has been shown to be a useful procedure in many clinical settings. The use of ultrasound has made this technique easier and safer to perform. It is important to know the anatomical landmarks and more especially the expected motor endpoints when using a stimulating needle, so the ultrasound technique, where difficult, can augment a landmark technique. The operator should be careful of repeated attempts as the medial thigh is a highly vascular area. It is recommended where possible to use ultrasound-guided techniques.
REFERENCES
Labat G. Regional Anesthesia: Its Technique and Clinical Application. Philadelphia, PA, and London, UK: W.B. Saunders; 1924.
Anagnostopoulou S, Kostopanagiotou G, Paraskeuopoulos T, et al. Anatomic variations of the obturator nerve in the inguinal region: implications in conventional and ultrasound regional anaesthesia techniques. Reg Anaesth Pain Med. 2009;34(1):33-39.
Wassef M R. Interadductor approach to obturator nerve blockade for spastic conditions of adductor thigh muscles. Reg Anesth. 1993;18(1):13-17.
Kaloul I, Guay J, Cote C, et al. The posterior lumbar plexus (psoas compartment) block and the three-in-one femoral nerve block provide similar postoperative analgesia after total knee replacement. Can J Anesth. 2004;51(1):45-51.
Yalcin E, Akyuz M, Ilgu O, et al. Ultrasonographically guided obturator nerve block for bilateral adductor spasticity in a para- plegic patient. Spinal Cord. 2014;52(Suppl 2):S24-S26.
Shah NF, Sofi KP, Nengroo SH. Obturator nerve block in transurethral resection of bladder tumour: a comparison of ultra- sound-guided technique versus ultrasound with nerve stimulation. Anesth Essays Res. 2017;11(2):411-415.
Rashiq S, Vadermeer B, Abour-Setta AM, et al. Efficacy of supplemental peripheral nerve blockade for hip fracture surgery: multiple treatment comparison. Can J Anaesth. 2013;60(3):230-243.
Runge C, Borglum J, Jensen JM, et al. The analgesic effect of obturator nerve block added to a femoral triangle block after total knee arthroplasty: a randomised controlled trial. Reg Anesth Pain Med. 2016;41(4):445-451.
Ghai A, Sangwan SS, Hooda S, et al. Evaluation of interadductor approach in neurolytic blockade of obturator nerve in spastic patients. Saudi J Anaesth. 2013;7(4):420-426.
Ramamurthy S. Obturator nerve block. In: Waldman S, ed. Pain Management. 1st ed. Philadelphia, PA: Saunders; 2006: 1331-1334.
Ahmad MT. Ultrasound-guided obturator nerve block: a proximal interfascial technique. Anesth Analg. 2012(1):226-239.
Yoshida T, Nakamoto T, Kamibayashi T. Ultrasound-guided obturator nerve block: a focused review on anatomy and updated techniques. Biomed Res Int. 2017;2017:7023750.
NYSORAA. Obturator nerve block—landmarks and nerve stimulator technique. Accessed December, 2022. https://www. nysora.com/regional-anesthesia-for-specific-surgical-procedures/lower-extremity-regional-anesthesia-for-specific-surgical- procedures/obturator-nerve-block/
Hadzic A, Sala-Blanch X, Xu D. Ultrasound guidance may reduce but not eliminate complication of peripheral nerve blocks. Anaesthesiology. 2008;108(4):557-558.- Darmanis S, Lewis A, Mansoor A, et al. Corona mortis: an anatomical study with clinical implications in approaches to the pelvis and acetabulum. Clin Anat. 2007;20(4):433-439.
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/