General Topics

QUESTIONS
Before continuing, try to answer the following questions. The answers can be found at the end of the article, together with an explanation.
- Which of the following statements is correct?
- The Robertshaw tube has a carinal hook
- The White tube is a left sided Carlens tube
- The Carlens tube has a carinal hook
- The Unitube has a double lumen
- List the indications for one lung anaesthesia
- What measures should be under taken in the event of hypoxia during one lung ventilation.
INTRODUCTION
In the UK, thoracic surgery accounts for only 0.5% of the total number of surgical procedures performed in the National Health Service (NHS). Due to the nature of the pathology being operated on, these patients usually present an anaesthetic challenge – they have a limited respiratory reserve and pulmonary function, and the nature of the anaesthetic technique requires advanced skill and specialist airway equipment.
One lung ventilation (OLV) is a technique that allows isolation of the individual lungs under anaesthesia. Safe implementation of this technique requires an understanding of specialist airway equipment, and of the physiological changes that occur during the procedure.
It is necessary to emphasize that endobronchial intubation, with these specific airway adjuncts, and OLV, may significantly add to the anaesthetic risk, resulting from trauma to the airways, and failure of adequate ventilation.
Indications for One lung ventilation
There are four main indications for one-lung anaesthesia:
- Isolation of the lungs
- To improve surgical access
- Greater control over ventilation
- Unilateral bronchopulmonary lavage
When haemorrage or infection is unilateral the isolation of the affected lung by endobronchial intubation, confers protection of the healthy lung.
For certain operations, the provision of one lung anaesthesia is a high priority. For example, repair of a thoracoabdominal aneurysm, pneumonectomy, videoscopic assisted thoracic surgery (VATS), single lung transplant. Conversely some other procedures such as oesophagectomy, lobectomy, wedge resections, hilar and mediastinal surgery and thoracic spine surgery, are made easier by one lung anaesthesia, but may in some instances be performed with standard dual lung ventilation.
Individual lung ventilation can be utilized in the treatment of bronchopleural fistulae, or as a lung protective strategy in individuals with large bullae or cysts.
Unilateral bronchopulmonary lavage is employed in the treatment of alveolar proteinosis.
Preoperative Assessment3,4
Alongside the generic preoperative assessment of the patient for anaesthesia, specific predictive tests of postoperative pulmonary function are conducted.
Often these patients are elderly, and may be predisposed to cardiovascular disease as a result of years of cigarette smoking. Most of the risk factors are not amenable to reduction or elimination prior to surgery.
It is important to investigate the possibilities of an obstructed airway, caused by masses (tumors), in the upper larynx, mid tracheal, lower tracheal and bronchial airways. Should these be present, they would require planning and careful management prior to anaesthesia and surgery. These are usually investigated radiologically by X-rays and CT scans.
Spirometry (post bronchodilator) and exercise data are used to predict the perioperative risk and postoperative respiratory reserve, i.e. pulmonary function and risk of respiratory failure.
The predicted postoperative FEV1 (ppo FEV1) can be estimated from the formula using the total number of segments in both lungs, 19 (9 in the Left lung, 10 in the Right lung) and the number of segments to be resected (y).
ppo FEV1 = FEV1 x (19-y)/19
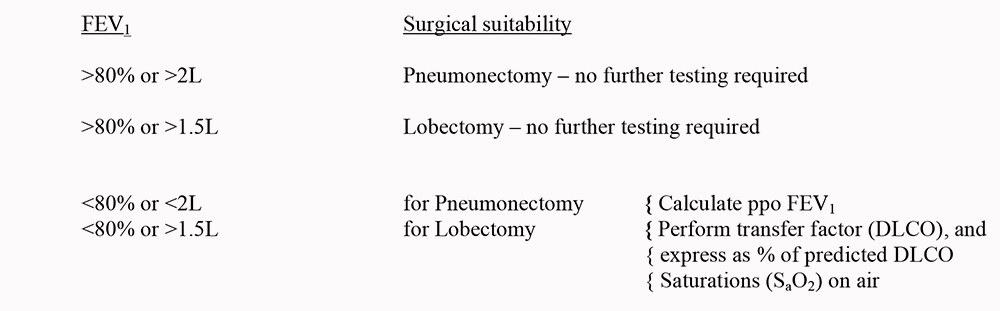
ppo FEV1 <40% and DLCO <40% = HIGH RISK
ppo FEV1 >40% and DLCO >40% and SaO2>90% = AVERAGE RISK (no further testing)
Any other combination requires further exercise testing:
Shuttle walk test:
- <25 shuttles or desaturation >4% = HIGH RISK
- >25 shuttles and <4% desaturation -> full cardiopulmonary exercise testing (specialist centres only) VO2max <15ml/kg/min = HIGH RISK; VO2max>15ml/kg/min = AVERAGE RISK
METHODS OF PROVIDING ONE LUNG VENTILATION
Double lumen tubes
The use of Double lumen tubes (DLT) allows the greatest control over switching from dual lung ventilation to single lung at various stages of a procedure. They also allow suctioning of individual lungs and the administration of CPAP/PEEP to individual lungs. They are available in left and right sided forms, but all utilize a tracheal and bronchial cuff. They are larger and longer that standard endo-tracheal tubes. The DLT is inserted with the bronchial lumen curved anteriorly, and once through the laryngeal inlet, requires a 70-90 degree rotation. For this reason they may be more difficult to insert than a standard endo-tracheal tube. This means that they may not be suitable for patients with difficult airways, or in patients at risk of aspiration. They are not suitable for patients under 35kg in weight. Due to the reduced internal diameter of each lumen they may present a considerable increase in airway resistance in a spontaneously breathing patient.
Left sided DLT’s are more commonly employed than their right sided equivalents (unless significant left sided lung resection, or a left pneumonectomy is planned). This is due to the difficulties in ensuring that the right double lumen tube is correctly positioned to prevent occlusion of the right upper lobe bronchus, which would result in failure to ventilate the right upper lobe, risking intraoperative hypoxia and atelectasis.
The most commonly used DLT are plastic disposable tubes, available in sizes 26 – 41 Fr. 37 – 39 Fr and 39 – 41 Fr are most suited for adult females and males, respectively. Tube size is dictated not only by width of the trachea, but the length of the trachea (patient height is used).
The orange rubber Robertshaw DLT is available in small, medium and large sizes.
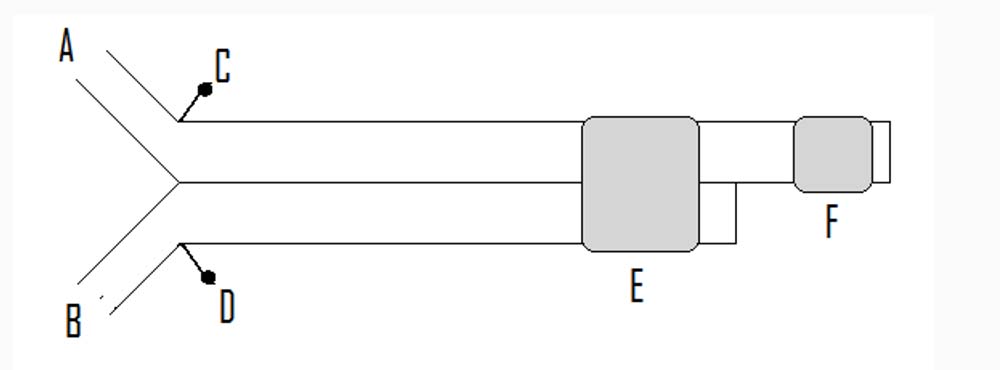
Diagram 1. Schematic representation of a double lumen tube.
A = Bronchial lumen. B = Tracheal lumen. C = Bronchial cuff pilot balloon. D = Tracheal cuff pilot balloon. E = Tracheal cuff. F = Bronchial cuff

Table 1: Properties of commonly employed Double lumen tubes
Endobronchial blockers
An advancement on the use of balloon tipped catheters is the use of specialist bronchial blockers. These too utilize inflation of a balloon to isolate individual bronchi but also have a hollow inner lumen allowing limited suctioning and administration of oxygen to the isolated lung. These can be inserted blindly but correct placement can be improved with the use of rigid or flexible fibre optic bronchoscopes.
Endobronchial intubation, with standard Endo tracheal tube.
The quickest and easiest way to isolate an individual lung is to introduce a standard endotracheal tube into one of the main bronchi. When more specialist equipment is not readily at hand or in order to isolate a lung in an emergency this may represent the most appropriate technique. However when compared to more advanced techniques it has a higher rate of bronchial damage and in the event of hypoxic episodes treatment options are more limited.
Tracheal intubation in combination with a balloon tipped catheter.
The main bronchi may be isolated by the introduction of fogarty embolectomy or foley catheters into the main bronchi, and inflating the balloons. In small or paediatric patients a pulmonary artery floatation (Swan-Ganz) catheter can be employed. Correct positioning of the balloons may be difficult and this technique does not allow suctioning or ventilation of the isolated lung.
Correct positioning of a Double lumen tube.
Correct positioning of double lumen tubes is vital. In the U.K the 1998 NCEPOD report implicated malpositioned tubes contributing to 30% of deaths in the perioperative period for patients undergoing oesophagectomy. Up to 12 % of all DLT may become displaced during the operative period. For this reason many departments recommended that the position of DLT’s should be confirmed with a fibre optic bronchoscope, post insertion. This is especially important if a right sided tube is being used due to the high chance of occlusion of the right upper lobe bronchus.
In some developing countries such equipment may not be readily available. The following clinical technique describes an alternative technique relying on auscultation and changes in airway pressure1,3.
The DLT has 2 curves – anteroposterior, and a 2nd curve of the bronchial tube (left or right). Prior to insertion of a DLT the patency of both tracheal and endobronchial balloons should be checked. Insertion is often aided by the use of a stylet, with an anterior curve applied to the bronchial lumen. Standard laryngoscopy is performed, and when the tip of the bronchial lumen is just through the laryngeal inlet (just past the vocal cords), the stylet can be removed. A 70-90 degree rotation of the tube is then performed in the direction of the bronchus you intend to intubate (clockwise rotation for a right sided tube or counter clockwise for a left sided tube). The tube is then advanced until resistance is felt, avoiding excess force.
The tube is connected to the anaesthetic circuit, and the tracheal cuff inflated until there is no air leak, and bilateral chest movement and air entry is confirmed by auscultation. Take note of the peak airway pressures at this time.
The tracheal lumen is opened, and the fresh gas flow to it clamped. The bronchial cuff can now be inflated (1-2ml of air), until no air leak is felt at the tracheal opening during ventilation. Auscultation is used to ensure good air entry at the apex and base of the lung unilaterally, and confirmed deflation of the contra lateral lung. Airway pressures are also noted. There should be a rise of no more than 8 to 12 cmH20 in peak airway pressure. Ventilate both lungs again. Now open the bronchial lumen, and clamp its fresh gas flow inlet. Tracheal ventilation is then initiated, which is confirmed by unilateral air entry on auscultation and unilateral chest expansion. If there is a rise in airway pressure greater than 12 cmH20, or there is reduced air entry to the non- bronchial lumen it suggests the bronchial cuff is causing obstruction (by herniation across the carina) and needs to be inserted further. The bronchial cuff is deflated and auscultation is repeated. If there is no difference in air entry or if there is NO change in airway pressures on deflation of the cuff it suggests the tube is abutting the carina or the tracheal portion of the tube is endobronchial, and the tube should be slightly withdrawn.
Physiological changes during one lung anaesthesia
For bronchial lavage or for use in intensive care the patient will often be in a supine position. However, for many thoracic operations the patient will be in the lateral decubitus position to further facilitate surgery. The lower and upper lungs when in this position are termed dependent and non dependent, respectively.
Due to the effects of gravity, in the lateral position, the pulmonary blood flow will be greatest in the dependent lung, whereas the non dependent lung will have a higher compliance and be easier to ventilate. This compliance will increase further on opening of the thoracic cavity.
On initiation of one lung ventilation (OLV), the primary physiological change that takes place is perfusion of the non dependent lung without ventilation, effectively causing a large shunt. However, this degree of shunt is reduced by gravity causing decreased blood flow to the non dependent lung, and is further diminished by a phenomenon termed hypoxic pulmonary vasoconstriction (HPV). The mechanism of HPV is not fully understood but is either as a direct response to regional alveolar and mixed venous hypoxia, or due to the release of vasoactive substances during hypoxia, causing vasoconstriction in the pulmonary blood vessels.
In terms of anaesthetic technique volatile agents and direct vasodilators directly inhibit pulmonary vasoconstriction. Interestingly vasoconstrictive drugs such as Noradrenalin preferentially constrict the vascular beds in areas of the lung with normal oxygen tensions, which indirectly inhibits pulmonary vasoconstriction.
Ventilatory changes occur during OLV in the lateral decubitus position and contribute to further problems in maintaining oxygenation. These problems that occur are threefold. Firstly, expansion of the dependent lung is restricted by the weight of the mediastinum, the cephalad displacement of the diaphragm and abdominal organs, and the non compliance of the hemi thoracic chest wall. This leads to atelectasis of the dependent lung, decreasing the ventilated lung surface. The result is HPV, increased resistance to flow in the dependent pulmonary artery, and diversion of flow to the independent lung, thereby increasing the shunt fraction further. Secondly, an increase in ventilation pressure and lung volume of the dependent lung impedes perfusion, leading to increased perfusion of the independent lung, and increased venous shunting.
Thirdly, poor ventilation strategies may cause lung injury (large tidal volumes, and high airway pressures).

Table 2. Summary of the V/Q changes in the lateral decubitus position
Management of Hypoxia during one lung ventilation.
A systematic approach should be used to treat hypoxia. Oxygen supply and ventilator function should be checked. Blockage or disconnection of the breathing circuit must be ruled out. It is vital to ensure that the endotracheal tube, be it single or double lumen, is still correctly positioned. If available this should be done with a fibre optic bronchoscope.
If possible oxygen should be delivered to the non-dependent lung. If a double lumen tube has been used then CPAP can be applied. Positive end expiratory pressure (PEEP) can also be applied to the dependent lung to attempt to recruit collapsed alveoli. However, it should be noted that this may impede pulmonary blood flow to the dependent lung which may exacerbate the degree of shunt. The application of PEEP may also decrease the venous return, thereby reducing the cardiac output and blood pressure.
Inform the surgeon of the problem. Surgical pressure on the mediastinum may have caused a fall in cardiac output which could be the cause. If oxygenation remains problematic, definitive management of the shunt caused by one lung ventilation is to instruct the surgeon to clamp the pulmonary artery. If this does not work it may be necessary to revert back to double lung ventilation, which may be quicker and easier to perform if a double lumen tube has been used.
If adequate oxygenation cannot be established with ventilation of both lungs it may be necessary to abandon the surgical procedure.
- Administer 100% Oxygen
- Check Ventilator, Circuit and catheter mount
- Clear secretions and debris by suctioning dependent lung
- Check tube position
- Apply CPAP or entrain Oxygen to non dependent lung
- Perform recruitment manoeuvre and apply PEEP to dependent lung
- Revert to two lung ventilation
- Clamp non-dependent pulmonary artery
ANSWERS TO QUESTIONS
- Q 1. Answer is C. The White tube is a right sided Carlens tube. The Omni tube has a single lumen and is designed to make placement of bronchial blockers easier. The Robertshaw tube does not have a carinal hook.
- Q 2. As outlined in the article the four indications are: Isolation of the lungs, Unilateral bronchopulmonary lavage, to provide greater control over ventilation and to improve surgical access.
- Q 3. The stepwise management is summarized in the box above.
REFERENCES and FURTHER READING
- Ahmed S, Janjua S, Ishaq M, Tariq M, Raza H. Double lumen intubation; reliability of the auscultatory method? Professional Med J 2009; 16: 105-108
- Karzai W, Schwarzkopf K. Hypoxemia during One Lung Ventilation: Prediction, Prevention, and Treatment. Anesthesiology 2009; 110: 1402-1411
- Faber P, Klein A. Theoretical and practical aspects of anaesthesia for thoracic surgery. Journal of Perioperative Practice 2008; 18: 121-129
- British Thoracic Society and Society of Cardiothoracic Surgeons of Great Britain and Ireland Working Party. Guidelines on the selection of patients with lung cancer for surgery. Thorax 2001; 56: 89-108
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/