Paediatric Anaesthesia

Try to answer these questions before reading the tutorial. Discuss them with you’re your colleagues or trainer. Answers are given at the end of the tutorial.
- What are the advantages and disadvantages of regional blocks in children?
- What are the contraindications to regional blocks in children?
- Name some local anaesthetic drugs. What type of drug are they (ester or amide)?
- How do local anaesthetics work?
- What factors affect the onset and duration of a block?
- Which has the faster onset: lidocaine or bupivacaine?
- Which lasts longer: chirocaine or bupivacaine?
- How many mg of drug are present in:
- 10 ml 1% lidocaine
- 2 ml 0.25% bupivacaine
- 30 ml 0.125% chirocaine
- 5ml 2% lidocaine
- What is the difference between a regional block needle and an ordinary one?
- How does a peripheral nerve stimulator work? Is it always necessary and if not, why?
- What are the complications of regional block?
- What is local anaesthetic toxicity? How would you recognise it:
- in an awake patient?
- in an asleep patient?
- How do you treat local anaesthetic toxicity?
Introduction
Regional anaesthetic blocks in children are safe and provide very effective pain relief both per- and post operatively. The techniques in children are the same as for adults.
Whilst it is safer to perform a regional block in an awake patient (complications can be spotted earlier and risks are reduced) the majority of children would not tolerate this. As a result regional blocks are usually placed with the child asleep. An extra degree of vigilance is therefore necessary to avoid the problems this may cause.
This tutorial looks at the principles involved with using regional blocks in children. Actual blocks are not discussed, but can be found in the online handbook on Regional Blocks on the World Anaesthesia homepage www.worldanaesthesia.org , and will be the subject of a future tutorial of the week.
Contents
- Advantages, disadvantages and contraindications
- Local anaesthetics
- Regional block needles
- How to use a peripheral nerve stimulator
- Complications of regional blocks
- Signs, symptoms and treatment of local anaesthetic toxicity
- Rules for performing regional blocks
1. Advantages, disadvantages and complications
Advantages
If used as sole anaesthetic technique regional blocks are probably safer than general anaesthetics and avoid the complications associated with them. It is inexpensive, and avoids the need for an anaesthetic machine. There is less post-operative sedation and nausea, and a faster return to “normal”. However, most regional blocks in children are done with the child asleep. Even so, with a block in place less anaesthetic will be needed to keep the child asleep, there is less surgical stress response, and analgesia lasts into the post-operative period
Disadvantages
- Patient or surgeon anxiety when the patient is awake. (But most children are asleep).
- Time delay when performing block as well as GA; good technique requires knowledge, skill and the right equipment.
- Risk of complications from regional block as well as from GA: failure (up to 10%), permanent damage to nerve or other structure.
Contraindications
Absolute:
- Patient refusal
- Major coagulation disorders
- Infection at the site of needle insertion
Relative:
- Shocked or severely hypovolaemic patient
- Anticipated technical difficulty, inexperienced anaesthetist
- Neurological disease (eg multiple sclerosis)
- Uncertain duration of surgery (the surgery may outlast the block, but in an asleep patient the block can be repeated, or placed at the end of the operation).
2. Local Anaesthetics
The local anaesthetic solutions available are mostly amides. Esters (eg cocaine) are less stable, shorter acting and more likely to cause allergic reactions.
Solutions available include:
- Bupivacaine: 0.25%, 0.5% both plain or with vasoconstrictor (adrenaline)
- Levobupivacaine (Chirocaine, the L-isomer of bupivacaine) 0.25%, 0.5%
- Lidocaine 1%, 2%
- Prilocaine 1%, 4% (usually for Intravenous regional anaesthesia)
- Ropivacaine 0.2%, 0.75%, 1%
Mechanism of Action
The local anaesthetic is injected into the tissues surrounding a nerve (but NOT into the nerve). It diffuses into the nerve, and causes a reversible block of the sodium channels. This prevents depolarisation and conduction of the nerve action potential.
Sensory nerves are blocked before motor because they are smaller and have less myelin so drug diffuses more quickly into the nerve. A bigger dose of local anaesthetic (higher concentration or larger volume), gives a quicker onset and longer duration of the block.
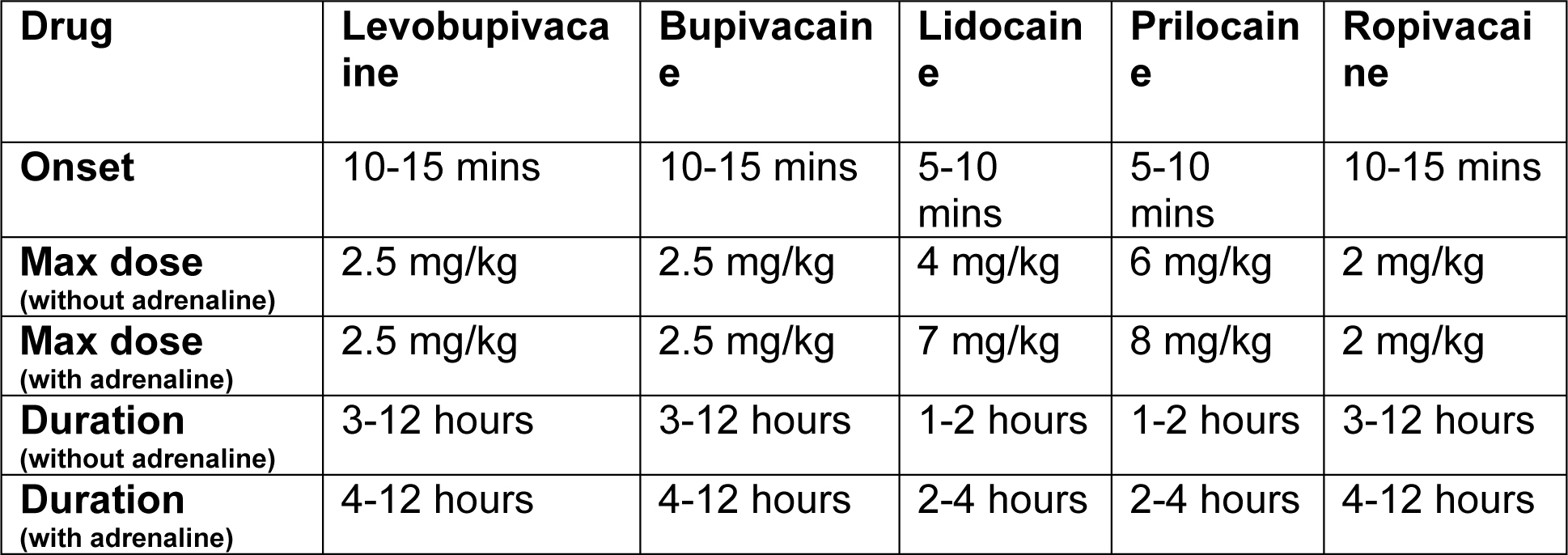
The duration of action depends on the drug used (bupivacaine lasts longer than lidocaine), the amount of drug present, protein binding at the site of action, and speed of drug removal from it (depends on nerve size and vascularity or the area). Additives such as adrenaline and sodium bicarbonate also prolong the duration of block.
For a rapid onset of block use lidocaine or prilocaine. For post-operative analgesia where a longer duration is required use bupivacaine, chirocaine or ropivacaine.
Solutions are given as percentages. This equals the amount of drug (in grams) in 100ml.
- 1% solution = 1g in 100ml = 1000 mg in 100ml = 10 mg/ml
3. Regional block needles
These are short-bevelled needles that give a distinctive “feel” or “click” as they pass through fascial planes. This helps locate the correct site for injecting local anaesthetic. They are also necessary for using a peripheral nerve stimulator.
If not using a nerve stimulator an ordinary needle may be used, but needs to be blunted slightly (eg by tapping it very gently once on the inside of a sterile glass ampoule) to give the same “feel”.
4. How to use a Peripheral nerve Stimulator (PNS)
This is not always necessary, but increases the chance of success when performing a block, especially if the patient is asleep.
Equipment required:
- Stimulating (regional block) needle – different sizes available according to block 25, 50 and 100mm (depth required to reach nerve).
- Peripheral nerve stimulator. Black (Cathode -ve) and red (anode +ve) electrodes. Connect black (negative) to needle and red (positive) to patient via an ECG electrode. Current adjustor – set at 1mA, frequency set at 2Hz
Technique:
- Flush needle with local anaesthetic
- Insert insulated needle through skin according to landmarks
- Start with current at 1mA looking for appropriate motor response
- When motor response obtained reduce current to the minimum possible which still obtains a motor response (threshold). If this is as low as 0.2mA then reposition as intraneural placement is likely. Aspirate then inject. The motor response should disappear after a 1 ml of local anaesthetic solution due to displacement of the nerve away away from the needle. If the motor response still persists then reposition the needle.
- Inject slowly. Aspirate every few mls looking for blood. If blood present, reposition needle.
- If there is any increased resistance to injection the needle may be intraneural. Stop injecting and reposition needle.
5. Complications
- Wrong drug, wrong site – always check carefully beforehand
- Nerve damage: either from direct trauma or by injection into the nerve (use a nerve stimulator and regional block needle where possible, avoid forceful injection, look for signs of pain).
- Haematoma
- Damage to other local structures (bone, muscle, lung depending on site of block)
- Infection (always use aseptic technique).
- Vasoconstrictor problems (do not use adrenaline in concentrations greater than 1:200,000 (5 micrograms/ml), never use adrenaline around end-arteries (fingers, penis).
- Local anaesthetic toxicity: occurs with intravenous injection or excess absorption from injection site.
6. Signs, symptoms and treatment of local anaesthetic toxicity
Signs and symptoms
The central nervous and cardiovascular systems are primarily involved, with areas having a good blood supply affected first. Early CNS signs will not be obvious in an anaesthetised patient, so be very careful to check that the injection is not intravascular by aspirating before injecting (this may still miss an intravenous needle placement).
CNS
- Early: tingling lips, ringing in the ears, light-headedness, confusion, nausea and vomiting.
- Later: convulsions, coma, respiratory arrest, cardiovascular collapse.
CVS
- Early: if adrenaline has been used with the local anaesthetic, tachycardia and hypertension may occur before cardiovascular collapse.
- Later: bradycardia, hypotension, cardiac arrest (ventricular fibrillation, which can be resistant to defibrillation especially with bupivacaine. Chirocaine is meant to be safer in this respect).
Treatment
*Stop injecting!*
Resuscitation (ABC) as per APLS guidelines (see TOTW Paediatric Shock)
A: secure and maintain the airway, intubate if necessary
B: ventilate the patient until they can breathe adequately for themselves
C: maintain circulation with atropine (bradycardia), fluids and adrenaline (hypotension) and CPR if cardiac arrest occurs.
Toxic doses local anaesthetic agents increase the Q–T interval on the ECG which may lead to VT or VF. Defibrillation may be required, but may be ineffective until the local anaesthetic wears off.
Bretylium was the drug of choice for ventricular arrhythmias secondary to local anaesthetic toxicity. Now that it is no longer available, there are 2 alternative antiarrhythmic agents for which some evidence exists for their use: amiodarone and magnesium
Amiodarone
Class III antiarrrhythmic agent (blocks K channels primarily but also has class I, II, and IV activity). It increases the duration of the action potential. It is used in resuscitation for resistant VF/pulseless VT. Also used for the chemical cardioversion of atrial and ventricular arrhythmias.
- Paediatric Dose Loading dose: 5mg/kg diluted in 5% dextrose. Slow injection over at least 3 minutes. Infusion: 5 –15mcg/kg/min.
Magnesium
Physiological calcium antagonist. Used for Torsades de pointes and refractory VF if hypomagnesaemia suspected.
- Paediatric Dose Loading Dose: 50mg/kg (0.2mmol/kg) diluted in 5 % dextrose. Give over 15 minutes. Infusion: 25mg/kg/hour (0.1mmol/kg/hour)
Key Point
Always have emergency resuscitation equipment on hand, check it and know how to use it.
7. Rules for Performing Regional Blocks
- Ensure no contraindications to the local block (ie; surgical, infection, coagulopathy)
- Obtain consent: explain common risks versus the benefits
- Perform in an appropriate environment with a trained assistant and resuscitation equipment available (in case seizures, arrhythmias occur)
- Establish intravenous access
- Attach monitoring (pulse oximeter, ECG, blood pressure as appropriate)
- Know the anatomy: confirm correct side/site with consent form and surgeon
- Know the correct technique, correct dose and how to manage complications. Never exceed the maximum dose
- Always use an aseptic technique
- Always aspirate before you inject to avoid intravenous injection
- Inject small amounts at a time looking for signs of incorrect placement
- Most paediatric blocks are performed asleep, use a peripheral nerve stimulator wherever possible.
- Avoid neuromuscular blockers before using a peripheral nerve stimulator, otherwise there will be no muscle twitches! (Common mistake!!)
- Record the technique in the notes and any complications that occur eg: bleeding
References:
- The Abbott pocket guide to practical peripheral nerve blockade. B Nicholls, D Conn, A Roberts. Published 2003.
- Regional Anaesthetic Blocks. John Hyndman. World Anaesthesia website. www.world-anaesthesia.org
Answers:
- What are the advantages and disadvantages of regional blocks in children?
- see section 1
- What are the contraindications to regional blocks in children?
- see section 1
- Name some local anaesthetic drugs. What type of drug are they (ester or amide)?
- amides: lidocaine, prilocaine, mepivacaine, bupivacaine, ropivacaine, levobupivacaine (chirocaine).
esters: cocaine, procaine, amethocaine, and chloroprocaine. [Check the prefix. Amides have an ‘i’ in the prefix, esters do not].
- amides: lidocaine, prilocaine, mepivacaine, bupivacaine, ropivacaine, levobupivacaine (chirocaine).
- How do local anaesthetics work?
- see section 2
- What factors affect the onset and duration of a block?
- see section 2
- size and function of nerve (sensory or motor).
- type and amount of local anaesthetic injected (mg).
- protein binding at site of action
- vascularity of area (allows drug to be removed quicker. eg intercostal area very vascular, so block relatively shorter acting) additives eg adrenaline, vasoconstricts and prolongs block
- Which has the faster onset: lidocaine or bupivacaine?
- lidocaine
- Which lasts longer: chirocaine or bupivacaine?
- A trick question – they are the same drug! Bupivacaine is the racaemic mixture of both R and S enantiomers, chirocaine (levobupivacaine) is the S enantiomer only. Chirocaine is less cardiotoxic than bupivacaine.
- How many mg of drug are present in:
- 10 ml 1% lidocaine – A. 100 mg. (1%=10 mg/ml)
- 2 ml 0.25% bupivacaine – A. 5 mg (0.25%=2.5 mg/ml)
- 30 ml 0.125% chirocaine – A. 37.5 mg (0.125%=1.25 mg/ml)
- 0.5ml 2% lidocaine – A. 10 mg (2%=20 mg/ml)
- What is the difference between a regional block needle and an ordinary one?
- see section 3.
- How does a peripheral nerve stimulator work? Is it always necessary and if not, why?
- see section 4.
- What are the complications of regional block?
- see section 5.
- What is local anaesthetic toxicity? How would you recognise it:
- see section 6.
- Toxicity occurs when the blood levels of the drug rise too high. This may be due to intravenous injection or excess absorption from the injection site.
- The early warning signs will not be apparent in an asleep patient and apnoea or cardiac arrest may be the first indication. Adding adrenaline to the solution may give advance warning as it can cause tachycardia with intravenous
- injection. However the most important thing is to anticipate problems, have full monitoring in place and check for intravenous placement by careful aspiration prior to slow injection of anaesthetic.
- How do you treat local anaesthetic toxicity?
- see section 6.
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/