General Topics

KEY POINTS
- Anaemia is a common, often reversible, contributing factor to post-operative morbidity and mortality.
- A screening full blood count is advised in all patients prior to undergoing major/complex surgeries, or in those with significant co-morbidities scheduled for intermediate surgery.
- Iron studies should be performed in cases of anaemia to guide management of the underlying pathology.
- Different types of anaemia may co-exist in the same patient.
- Correction of anaemia may take several months, so treatment options must be balanced against the urgency of surgery.
INTRODUCTION
The World Health Organisation (WHO) defines anaemia as a haemoglobin concentration of <130 g/L for men, 120 g/L for non pregnant women and <110 g/L for pregnant women1. Globally, 41.8% of pregnant women, 30.2% of non-pregnant women, 12.7% of men, and 23.9% of the elderly (over 60 years old) are estimated to be anaemic by these criteria2. Pre-operative anaemia is a risk factor for post-operative morbidity and mortality in non-cardiac surgery; wherein even minor deviations below the normal range are associated with poorer outcomes3,4
Red Blood Cells
Haematopoiesis is the formation of the cellular components of blood from haematopoietic stem cells present within the long bones of children and the pelvis, sternum, skull and vertebrae of adults. As red blood cells develop, they synthesise haemoglobin and their nuclei shrink. When released into the circulation, the nucleus has been lost and the cells are called reticulocytes. Maturation to erythrocytes occurs within 24 hours of release.
The typical red blood cell circulates for approximately 120 days, after which it is removed from the circulation by macrophages in the liver, spleen, and bone marrow. The red blood cell is the cellular vehicle responsible for transport of haemoglobin, and therefore oxygen, around the body. Understanding the equation below highlights key factors affecting oxygen delivery to the tissues.

Figure 1. Equation demonstrating the factors determining oxygen delivery to tissues. DO2 = Oxygen delivery (ml/min/m2), CO = Cardiac output (ml/min), 1.34 = Huffner’s Constant, the amount of oxygen able to bind per gram of haemoglobin (ml O2 / g Hb), [Hb] = Haemoglobin concentration (g/dL), SaO2 = Arterial haemoglobin oxygen saturations, 0.003 = Oxygen carrying capacity of plasma (ml O2/100ml blood), PaO2 = Partial pressure of oxygen in arterial blood
At sea level, the two most important factors determining oxygen delivery are cardiac Output (CO) and the concentration of haemoglobin ([Hb]). Anaemia can thus have a significant impact on oxygen delivery. At times of physiological stress (e.g. surgery), tissue hypoxia may result.
Screening
Guidance from the United Kingdom National Institute for Health and Care Excellence (NICE) suggests that a Full Blood Count (FBC) should be performed pre-operatively for all elective patients undergoing major or complex surgery. This also applies to ASA 3 or 4 patients with cardiovascular or renal symptoms due to undergo intermediate surgery5.
If a previously undiagnosed anaemia is identified, a detailed history and iron studies should be conducted to further differentiate the type of anaemia and guide treatment. The algorithm below assists in diagnosis of the most common causes of anaemia.
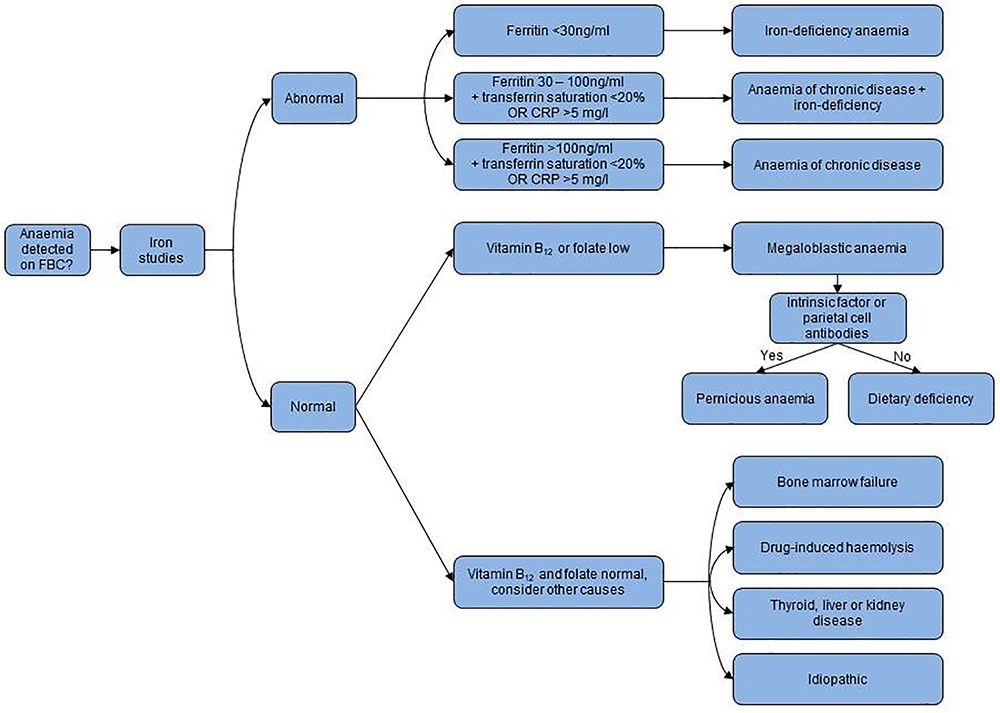
Figure 2. Classification of anaemia. Anaemia on FBC defined as per WHO definitions of anaemia1 Adapted from the original figure by Munoz et al6.
CLASSIFYING ANAEMIA
Anaemia with Low Ferritin (<30ng/ml)
Iron Deficiency Anaemia
This is the most common form of anaemia worldwide1 and results from low dietary iron intake, poor absorption, high requirements (such as pregnancy or rapid growth), or from chronic blood loss. Common causes of chronic blood loss are menorrhagia, chronic gastrointestinal bleeding, or mechanical breakdown of red cells (such as by mechanical cardiac valves).
Treatment
Oral iron is a low-cost intervention for dietary iron deficiency. Treatment needs to be commenced at least eight weeks prior to surgery and continued post-operatively. There is often poor adherence to oral iron therapy because of gastro-intestinal side effects and the duration of treatment (some cases require up to six months for iron stores to be replenished).
Intravenous (IV) iron is generally better tolerated than oral preparations, but carries a 0.024 – 0.068% risk of anaphylaxis (after sensitisation), dependent on the preparation used7. IV iron treatment is recommended for those who cannot tolerate or absorb oral iron, those with functional iron deficiency, or when surgical urgency does not allow sufficient time for oral iron therapy to be effective8. A rise in haemoglobin is typically observed within one to two weeks, with peak effect observed at around six weeks. Studies evaluating the impact of preoperative intravenous iron therapy in orthopaedic and major abdominal surgery demonstrated a decreased red cell transfusion requirement post-operatively9,10.
Special Cases of Iron-Deficiency Anaemia
Sickle cell disease can be a significant cause of anaemia depending on the geographic location. Genetic abnormalities in the structure of the red blood cell results in increased turnover secondary to breakdown of fragile erythrocytes, or from sequestration within the spleen. Severity of the disease is determined by its genetic phenotype. Pre-operative red blood cell transfusion may be indicated to treat an absolute anaemia, or to increase the amount of normal red blood cells present. Patients homozygous for the condition are at higher risk of being affected and more likely to necessitate transfusion to address their disease as opposed to just a numeric anaemia. Local guidelines should be sought, and guidance from a specialist Haematologist included. Unless already diagnosed, a high index of suspicion and enquiry about family history is vital.
Malaria is endemic around the equator, in particular; Sub-Saharan Africa, parts of the Americas, and Asia. Patient history is often highly suggestive of infectious status. Screening FBC and liver function tests (LFT) may show a mixed picture of haemolysis, iron deficiency, erythropoiesis, and direct liver injury. Diagnosis is confirmed by thick and thin blood films with staining for Plasmodium falciparum. Suspicion of infection, or known infectious state should prompt involvement of Infectious Disease specialists, and consideration as to whether surgery should be delayed until treatment is completed and the anaemia has resolved. Iron supplementation during active infection is associated with higher mortality in paediatric populations11.
Chronic blood loss will present as an iron-deficiency anaemia with a high reticulocyte count, as the bone marrow compensates by releasing more immature red cells into the circulation. The cause should be investigated pre operatively and appropriate management instigated in advance of surgery. In elderly patients, cryptogenic anaemia consistent with chronic blood loss should always raise concerns for the presence of gastrointestinal tumours.
Mechanical heart valves can cause shearing and lysis of red blood cells, producing a rise in bilirubin with an elevated erythrocyte count. This is likely to be chronic, while the raised turnover of red cells can produce a co-existent iron-deficiency anaemia. Management involves regular transfusion to control symptoms, with consideration of surgical valve replacement if malfunctioning.
Anaemia with Ferritin level 30-100ng/ml
Anaemia of Chronic Disease with Iron-Deficiency Anaemia
A chronic inflammatory state is usually suggested by the history but may co-exist with iron-deficiency anaemia. A raised C-reactive protein (CRP) in the absence of acute pathology suggests chronic inflammation.
Common Causes:
- Autoimmune and connective tissue disorders e.g. rheumatoid arthritis, systemic lupus erythematosus, scleroderma or inflammatory bowel disease
- Chronic infection e.g. tuberculosis, hepatitis, or HIV
- Chronic disease e.g. chronic kidney disease, diabetes, chronic obstructive pulmonary disease, or heart failure
- Malignancy e.g. lymphoma, leukaemia, multiple myeloma, or renal cell carcinoma
- Critical illness or major trauma
Treatment
The primary focus is management of the underlying condition. Reducing inflammation increases iron absorption from the gut and increases the action of erythropoietin, thus improving utilisation of iron stores. Where iron-deficiency co-exists, treatment is as discussed earlier.
Anaemia with Ferritin >100ng/ml
Anaemia of Chronic Disease
Ferritin levels >100ng/ml, in the presence of chronic inflammation, may indicate iron sequestration. Caution is required in interpreting an increased Ferritin alone, as it is also elevated as an acute phase reactant. If microscopy reveals hypochromic erythrocytes, then co-existent iron-deficiency anaemia is present.
Treatment
As above.
Anaemia with Normal Iron Studies
B12 <150pg/ml and/or Folate <2ng/ml
Both Vitamin B12 and folate are essential to DNA synthesis and therefore erythropoiesis. Deficiencies rarely exist in isolation but are likely to co-exist with iron deficiency anaemia. Low levels of either can produce megaloblastic anaemia with macrocytosis. Because vitamin B12 is essential for nerve function, deficiency may also result in neurological involvement.
Pernicious anaemia is the commonest cause of Vitamin B12 deficiency, and is diagnosed by the presence of auto-antibodies to intrinsic factor or gastric parietal cells.
Treatment
If neurological involvement is evident, treatment is intramuscular hydroxocobalamin, with doses and frequency varying depending on the presence or extent of neurological involvement. Pernicious anaemia is treated with a loading regime, followed by maintenance treatment. Dietary deficiency of Vitamin B12 and folate is commonly treated with oral supplementation of Vitamin B complexes. They may also be considered for prophylaxis in chronic haemolytic states and patients undergoing dialysis. Specific doses for each situation should be sought based on local recommendations.
Anaemia with Normal Iron Studies, B12 and Folate
Bone Marrow Failure
Bone marrow failure is usually secondary in nature. A transient red cell aplasia may result from a viral infection e.g. parvovirus B19. Pregnancy can result in a longer transient red cell aplasia, while permanent aplasias can develop from viral hepatitis, lymphoproliferative disorders, or collagen vascular disorders (such as lupus).
Preoperative testing may reveal a pancytopaenia, which is the most common finding in bone marrow failure. If significant blood loss is anticipated from the pending surgery, pre-operative blood transfusion should be considered. Definitive treatment is bone marrow transplant, while pancytopaenia secondary to tumour or granuloma formation may improve with treatment of the underlying condition. Specialist Haematology advice should be sought for all cases of single cell type aplasia or pancytopaenia.
Thyroid
The relationship between thyroid function and anaemia is complex. Thyroid hormones stimulate erythropoiesis by directly activating erythrocyte precursors and by increasing erythropoietin gene expression in the kidneys12. Normocytic anaemia is the most common anaemia in thyroid disorders. Microcytic and macrocytic anaemia may also occur secondary to comorbid conditions, including other auto-immune disorders (such as pernicious anaemia), and co-existent nutritional deficiencies.
In the presence of an associated anaemia, clinical features which should increase suspicion of an associated hypothyroidism include: fatigue, weight gain, weakness, coarse dry hair, depression, cold intolerance, and irregular menses. Blood tests typically reveal low thyroxine (T4), with high or low Thyroid Stimulating Hormone (TSH) depending on the cause. Clinical suspicion or tests consistent with hypothyroidism should prompt referral to a family doctor or an endocrinologist for further work-up, management, and optimisation, with consideration of whether to delay surgery.
For those patients with hypothyroidism, exact estimates regarding the associated prevalence of anaemia varies, with studies identifying rates from 7.7 – 57.1% 13,14.
The exact mechanism of hyperthyroid-induced anaemia remains unclear but is likely secondary to nutrient deficiencies in a heightened metabolic state. The prevalence of anaemia in hyperthyroid patients has been demonstrated to range from 14.6 – 40.9% 12,14. Clinical features of overt hyperthyroidism include: weight loss, hyperhidrosis, tremor, heat intolerance, agitation, and psychosis. Clinical suspicion of hyperthyroidism should prompt specialist consultation. Adequate control of thyroid function may take several months.
Liver
Up to 75% of patients with chronic liver disease are anaemic, but the aetiology can be complex. The presence of oesophago-gastric varices, gastritis, gastric ulcers, or clotting disorders may cause slow blood loss and a resultant iron-deficiency anaemia. Portal hypertension leads to increased sequestration in the spleen. The secondary increase in erythrocyte turnover, as well as nutritional deficiencies, may result in a macrocytic appearance on blood film.
Treatment:
Management is complex and should ideally involve a gastroenterologist or hepatologist. Nutritional deficiencies (including iron) and the specific complications of chronic liver disease require several months to improve, and realistic targets should be set early to allow surgery to proceed in a timely manner.
Kidney
Erythropoietin is produced by healthy kidneys in response to cellular hypoxia, stimulating red blood cell production in the bone marrow. In failing kidneys, erythropoietin levels are low, resulting in a normocytic normochromic anaemia.
Treatment:
Indications for erythropoietin supplementation include 8,15:
- Symptomatic anaemia associated with chronic renal failure
- Symptomatic anaemia in adults receiving chemotherapy
- To allow for autologous blood to be donated pre-operatively
- To correct moderate preoperative anaemia in adults prior to surgery with an expected moderate blood loss
- Symptomatic anaemia in patients refusing blood transfusion
In the first two indications, erythropoietin should only be used to correct symptoms of anaemia. In end-stage renal failure and cancer, over-correction of anaemia can increase cardiovascular morbidity and overall mortality.
Drug-Induced Anaemia
Drug-induced haemolytic anaemia is a rare condition of uncertain incidence, associated with drug-dependent or independent erythrocyte autoantibodies. Associated drugs include: penicillin, cephalosporins, nitrofurantoin, chlorpromazine, and ibuprofen. Onset is usually within two weeks of commencing therapy and results in a raised reticulocyte count with hyperbilirubinaemia. Other drugs, in particular chemotherapy and disease-modifying agents, produce a pancytopaenia.
Treatment
Haemolytic anaemia resolves following cessation of the causative drug, but other causes should be actively investigated. Should the anaemia fail to resolve or pancytopaenia develop, further discussion with a haematologist is advised.
SUMMARY
Anaemia is a complex group of diseases with a variety of aetiologies, many of which often co-exist. Blood tests may reveal a confusing range of abnormalities, but a detailed history is vital in refining a differential diagnosis. Adequate time between pre-operative assessment and surgery is essential to allow identification, investigation, and optimal treatment of these patients. Treating even mild anaemia can result in better post-operative outcomes, but the time taken to achieve this must be balanced against the urgency of surgery.
REFERENCES
- World Health Organisation (WHO) Iron deficiency anaemia: assessment, prevention, and control. A guide for programme managers, 2001. www.who.it WHO reference number: WHO/NHD/01.3. (Accessed under: Publications, on 03/04/2018).
- De Benoist B, McLean E, Egli I, Cogswell M. Worldwide prevalence of anaemia 1993–2005 : WHO global database on anaemia. www.who.it (Accessed under Nutrition Publications, on 03/04/2018)
- Wu WC, Schifftner TL, Henderson WG et al. Preoperative hematocrit levels and postoperative outcomes in older patients undergoing noncardiac surgery. JAMA 2007;297:2481–2488. [PubMed: 17565082]
- Musallam KM, Tamim HM, Richards T et al. Preoperative anaemia and postoperative outcomes in non-cardiac surgery: A retrospective cohort study. Lancet 2011;378:1396–1407. [PubMed: 21982521]
- NICE Guideline [NG45], Routine preoperative tests for elective surgery. https://www.nice.org.uk/guidance/ng45 (Accessed on 03/04/2018).
- Munoz M, Acheson AG, Auerbach M, et al. International consensus statement on the peri-operative management of anaemia and iron deficiency. Anaesthesia 2017;72:233–24.
- Wang C, Graham DJ, Kane RC et al. Comparative Risk of Anaphylactic Reactions Associated With Intravenous Iron Products. JAMA 2015;314(19):2062-8. [PMID: 26575062]
- Nice Guideline [NG24], Blood transfusion. www.nice.org.uk/guidance/ng24 (Accessed on 03/04/2018).
- Munoz M, Gomez-Ramirez S, Cuenca J, et al. Very-short-term perioperative intravenous iron administration and postoperative outcome in major orthopedic surgery: a pooled analysis of observational data from 2547 patients. Transfusion 2014;54:289–99. [PubMed: 23581484]
- Froessler B, Palm P, Weber I et al The Important Role for Intravenous Iron in Perioperative Patient Blood Management in Major Abdominal Surgery, A Randomized Controlled Trial. Annals of Surgery 2016;264(1):41-46. [PubMed: 26817624]
- Sazawal S, Black RE, Ramsan M et al. Effects of routine prophylactic supplementation with iron, and folic acid on admission to hospital, and mortality in preschool children in a high malaria transmission setting: community-based, randomised, placebo-controlled trial. Lancet 2006;367:133–143. [PubMed: 16413877]
- Golde DW, Bersch N, Chopra IJ, et al. Thyroid hormones stimulate erythropoiesis in vitro. British Journal of Haematology 1977;37:173-177. [PubMed: 603753]
- M’Rabet-Bensalah K, Aubert CE, Coslovsky M, et al. Thyroid dysfunction and anaemia in a large population-based study. Clinical Endocrinology 2016;84:627-631. [PubMed: 26662849]
- Omar S, Hadj Taeib S, Kanoun F, et al. Erythrocyte abnormalities in thyroid dysfunction. Tunis Med 2010;88:783-788. French. [PubMed: 21049405]
- British National Formulary (BNF) online. https://bnf.nice.org.uk/ (Accessed on 18/06/2018).
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/