Intensive Care Medicine

KEY POINTS
- Propofol infusion syndrome is a rare but potentially fatal condition first described in the paediatric population and subsequently reported in adult intensive care, particularly in neurointensive care.
- Refractory bradycardia, unexplained metabolic acidosis, electrocardiogram changes and rhabdomyolysis are consistent features.
- There is no diagnostic test; therefore, a low index of suspicion is required for early detection.
- Pathophysiology is not clearly understood but resembles mitochondrial diseases.
- The mainstay of management is prevention and early detection.
- Treatment of established diagnosis is supportive.
INTRODUCTION
Propofol is a nonbarbiturate intravenous anaesthetic agent that was approved for use in 1989. As with many general anaesthetic agents, it produces its hypnotic effects by potentiating the effects of the inhibitory neurotransmitter gammaaminobutyric acid (GABA).
It is an important drug that is widely used throughout the world. It is currently on the World Health Organisation’s (WHO) ‘Model List of Essential Medicines’, which lists what WHO considers to be the most effective and safe medications needed to meet the needs of a health care system.1
Propofol is widely used for the induction and maintenance of general anaesthesia, and it also has many properties that favour its use as a sedative agent in the critically ill. Of note, 70% of propofol use worldwide is for sedation. These properties include the following:
rapid onset and offset of action;
sedative, anxiolytic, antiemetic and anticonvulsant properties; and
beneficial anti-inflammatory and antioxidant properties.
It has an excellent safety profile, but a rare and potentially fatal complication called propofol infusion syndrome (PRIS) is recognised.
The first reported case of this syndrome occurred in 1990, in a 3-year-old child in Denmark. Two years later, a case series was published in the British Medical Journal, describing similar presentations in 5 young children.2 A United States Food and Drug
Administration study that year failed to find a link between propofol and further deaths, but propofol’s use for paediatric sedation was abandoned shortly afterward, explaining in part why subsequent literature features mostly adult cases.
Similar presentations in adults started to be reported during the late 1990s, starting in 1996 with the case of a 30-year-old woman admitted with exacerbation of asthma who went on to receive sedation and invasive ventilation.
This tutorial aims to summarise the clinical features, pathophysiology and management of the condition.
DEFINITION
The term propofol infusion syndrome (PRIS) was first coined by Bray in 1998, in an article that aimed to define some of the common clinical features of the cases in which children had suffered adverse consequences associated with, although not proven to be caused by, high-dose and long-term (.48 hours) propofol infusions.3
Although there has been no universally accepted definition of PRIS, an early definition was as follow:
…occurrence of acute refractory bradycardia, progressing to asystole, associated with propofol infusion, in the presence of one or more of the following: metabolic acidosis, rhabdomyolysis or myoglobinuria, lipaemic plasma, or enlarged liver or fatty liver.4
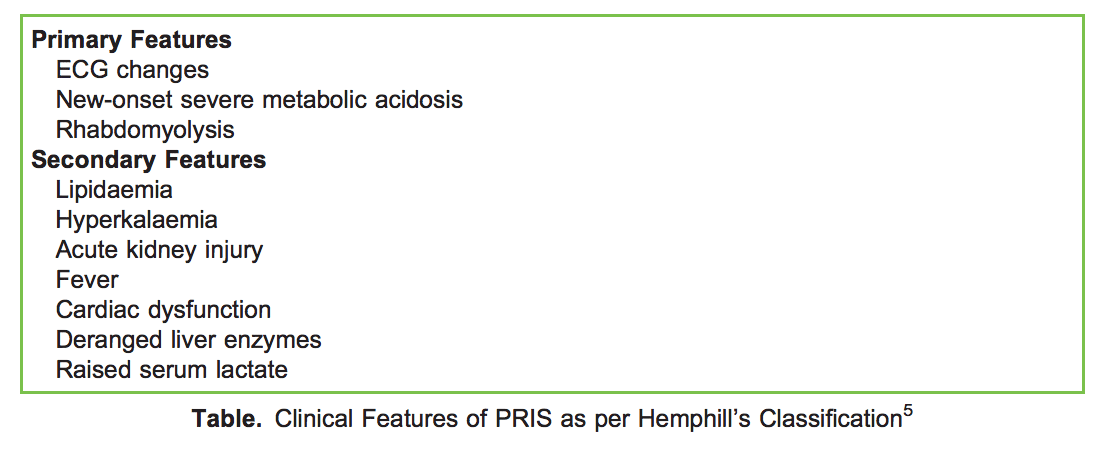
The description including refractory bradycardia leading to asystole in this phrasing was felt to limit practical value, and so an alternative definition has recently been described, based on primary features (those that can be the sole manifestation of PRIS) and secondary features (those that occur in combination with other features).5 This latter definition is as follows and these features are detailed in the Table:
…propofol infusion syndrome occurs in critically ill patients receiving propofol infusions, typically either high dose (.5mg/ kg/hr) or of long duration (.48 hrs), and is characterised by one or more of the following: otherwise unexplained metabolic acidosis, rhabdomyolysis, or ECG changes with or without acute kidney injury (AKI), hyperkalaemia, lipidaemia, cardiac failure, fever, elevated liver enzymes or raised lactate.5
CLINICAL FEATURES
Hemphill et al,5 as described above, classified the clinical features into primary (features characteristic and consistent with PRIS that can be the only presenting feature) and secondary (those that occur in combination with other features):
The primary features include electrocardiogram (ECG) changes characteristically described as a ‘coved pattern’ of ST elevation in leads V1-V3 as per Brugada syndrome; however, they can also include any form of ventricular or supraventricular tachycardia, bundle branch block or bradycardia. Furthermore, severe new-onset metabolic acidosis (a high anion gap metabolic acidosis) is often contributed to by renal dysfunction and a raised serum lactate. The third primary feature is rhabdomyolysis, which often becomes a causative factor in the development of acute kidney injury.
INCIDENCE
The lack of a universal definition of PRIS has led to variation in the reported incidence. However, one multicentre US adult critical care investigation described an incidence of 1.1%, which would mean an average critical care unit might well see a handful of cases each year.6
RISK FACTORS
Cumulative Dose
There is plenty of evidence to suggest a linear relationship between the cumulative dose of propofol and quantity and severity of features. Although the definition given above referenced high doses (.5 mg/kg/h) or long duration of administration (.48 hours), there have been many cases reported at lower cumulative doses.
Obesity
Pharmacokinetic studies suggest that dosing for propofol should be based on a patient’s lean body weight rather than actual body weight. (Target controlled infusion models are not formally validated in the obese and use different weight values in their calculations).
Although there has been no clear relationship between obesity and the development of PRIS, the dose for sedation should be calculated based on lean body weight. Cases have been reported in which administration of propofol based upon actual body weight has been associated with PRIS and may have been exacerbated by the ‘relative overdose’ of propofol.
Steroids
Steroids are known to contribute to the development of a critical illness myopathy, possibly by triggering enzymes that cause direct muscle damage. The rhabdomyolysis seen in PRIS may occur as a result of a similar mechanism, and there is certainly a link between steroid therapy and the development of PRIS.
Catecholamines
There is a link between the use of vasopressors and the development of PRIS.7 It is thought that propofol clearance is increased by the raised levels of endogenous catecholamines seen in the brain-injured patient or the patient with a hyperdynamic circulation in the context of sepsis or a systemic inflammatory response syndrome. This is also thought to occur with administration of higher doses of inotropic or vasopressor infusions. The increased clearance may reduce the therapeutic effect of propofol, leading to the need to increase the administered dose of propofol. Whether this is a causal effect is not clear; acidosis due to PRIS may impair vasomotor tone, leading to an increased vasopressor requirement.
Critical Illness
The neuroendocrine stress response to critical illness causes a surge in catecholamines and glucocorticoids, which are implicated as risk factors for PRIS. These hormones modulate the activity of lipase enzymes, promoting breakdown of triglycerides into glycerol and free fatty acids (FFAs). Furthermore, in critical illness, there is a shift from carbohydrate to lipidbased substrates for energy production, which also increases FFAs. This is of importance as FFAs are a key substrate for the part of the pathophysiological mechanism of PRIS (see below).
Lipid Overload
It is possible for patients to develop a relative lipid overload associated with parenteral nutrition, propofol infusions or both.4 This leads to an accumulation of unused FFAs. There should be an adequate source of carbohydrate to balance this out and suppress excessive lipolysis, perhaps in the form of a dextrose infusion. This may be one of the reasons that children, with their relatively limited glycogen stores, exhibit an increased susceptibility to PRIS.
PATHOPHYSIOLOGY
The exact mechanism underlying PRIS is not fully understood. We know that propofol uncouples oxidative phosphorylation and energy production in mitochondria as well as inhibits electron transfer in the myocyte electron transport chain, leading to a disturbance in ATP production, cellular hypoxia and acidosis. Most of the existing evidence points to this as the most likely pathway for the aetiology of PRIS.
FFAs, which are an essential fuel for these myocytes during ‘stress’, cannot be used when oxidative phosphorylation is uncoupled. They can build up and act as a proarrhythmogenic substance, contributing to cardiac dysfunction in PRIS.8
Propofol also antagonises beta-adrenergic receptors and calcium channel binding, further depressing cardiac function and causing a degree of resistance to inotropic agents.
It has also been suggested that the pathophysiology resembles certain mitochondrial diseases, such as medium-chain acyl coenzyme dehydrogenase deficiency, suggesting that a genetic predisposition to PRIS may exist.
Ultimately, the uncoupling effect on the respiratory chain and the resultant imbalance between energy demand and utilisation causes the accumulation of lactate and myocyte necrosis. This leads to metabolic acidosis, cardiac dysfunction and rhabdomyolysis.
PREVENTION
It is known that the risk of PRIS rises with dosage of propofol, in terms of both the infusion rate and the duration of the infusion. The existing literature recommends infusion rates less than 5 mg/kg/h, although most manufacturers actually recommend a lower maximum infusion rate of 4 mg/kg/h.9
Although it makes sense to follow this recommendation, it is worth noting that cases of PRIS have been described after only a few hours of propofol or at infusion rates much lower than these.10
The coadministration of other agents, such as opioids or the use of additional/alternative agents if sedation requirements are high is another way to control the dose of administered propofol. If high doses are needed, close monitoring of pH, lactate and creatinine kinase (CK) is imperative.
Propofol should be avoided in patients with proven or suspected mitochondrial diseases because of the resemblance in pathophysiology of the two.
Given the role of FFAs in PRIS, it is also prudent to ensure a continuous carbohydrate supply to patients receiving a propofol infusion for sedation.
MANAGEMENT
The lack of a clear definition and the inevitable presence of confounding organ dysfunction in critically ill patients means that there are no established guidelines for treatment of PRIS.
The condition is difficult to treat, and awareness of its existence and the risk factors for its development, along with a high index of suspicion for signs in at-risk patients, is critical. Some institutions monitor CK levels daily after 48 hours of a propofol infusion.8
Once diagnosed, the following are priorities:
- stopping further administration of propofol and commencing alternative sedation,
- supportive therapy to treat the complications of PRIS and
- elimination of propofol from the body.
Cardiovascular support in the form of inotropic agents and/or vasopressors may be needed. Arrhythmias are treated in line with standard treatment algorithms. Catecholamine-resistant cardiac shock has been reported, possibly as a consequence of the calcium channel–blocking effect of propofol. The use of extracorporeal membrane support has been reported in such cases, whereas electrical pacing has been of limited use, possibly because of the direct nature of myocyte damage.
Metabolic acidosis should be addressed as it may propagate arrhythmias or reduce their effective treatment as well as potentially decrease the effects of vasoactive agents. This is done by ensuring an adequate minute ventilation, adequate intravascular volume and the early consideration of continuous haemofiltration.
Haemofiltration also has a role in the elimination of propofol from the body. Propofol is metabolised in the liver to water-soluble phenol derivatives, which are then excreted in the urine. Hemofiltration cannot eliminate the highly lipophilic propofol, but it can eliminate the water-soluble metabolites as well as help manage acidosis and hyperkalaemia, which may be caused by cardiac dysfunction or rhabdomyolysis.
There is limited evidence to suggest a role for bicarbonate other than as a temporising measure for hyperkalaemia in the presence of metabolic acidosis. Adequate fluid therapy is needed to treat myoglobinuria.
Summary
Propofol has pharmacokinetic properties that make it a good choice for sedation in the critically ill, but its use is associated with a definite incidence of PRIS. PRIS can present in a number of ways, but the primary clinical features are metabolic acidosis, ECG changes and rhabdomyolysis.
The condition is uncommon. There is no diagnostic test or antidote, and treatment is supportive, so a high index of suspicion should be maintained in any patient but particularly in those receiving a high dose or a prolonged infusion or those with specific risk factors for the development of PRIS. Doses should be limited to 4 mg/kg/h in all cases.
References
1. World Health Organisation. The selection and use of essential medicines: twentieth report of the WHO Expert Committee
2015 (including 19th WHO Model List of Essential Medicines and 5th WHO Model List of Essential Medicines for
Children). https://apps.who.int/iris/bitstream/handle/10665/189763/9789241209946_eng.pdf?sequence¼1. Accessed
December 3, 2019.
2. Parke TJ, Stevens JE, Rice ASC, et al. Metabolic acidosis and fatal myocardial failure after propofol infusion in children:
five case reports. Br Med J. 1992;305:613-616.
3. Bray RJ. Propofol infusion syndrome in children. Paediatr Anaesth. 1998;8:491-499.
4. Fudickar A, Bein B. Propofol infusion syndrome: update of clinical manifestation and pathophysiology. Minerva Anesth.
2009;75:339-344.
5. Hemphill S, McMenamin L, Bellamy MC, et al. Propofol infusion syndrome: a structured literature review and analysis of
published case reports. Br J Anaesth. 2019;122(4):448-459.
6. Roberts R, Barletta J, Fong J, et al. Incidence of propofol-related infusion syndrome in critically ill adults: a prospective,
multicenter study. Crit Care. 2009;13(5):R169.
7. Smith H, Sinson G, Varelas P. Vasopressors and propofol infusion syndrome in severe head trauma. Neurocrit Care.
2009;10:166-172.
8. Loh NW, Nair P. Propofol infusion syndrome. Cont Educ Anaesth Crit Care Pain. 2013;13(6):200-202.
9. Medicines and Healthcare Products Regulatory Agency. Summary of product characteristics for propofol. http://www.
mhra.gov.uk/spc-pil/?subsName¼PROPOFOL&pageID¼SecondLevel. Accessed December 18, 2019.
10. Fodale V, La Monaca E. Propofol infusion syndrome: an overview of a perplexing disease. Drug Saf. 2008;31:293-303
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/