General Topics

INTRODUCTION
Any surgical patient in hospital may be acutely ill for a number of reasons:
- their primary surgical condition e.g. peritonitis
- a pre-existing medical condition e.g. diabetes mellitus
- a result of developing a new “medical” illness whilst in hospital for a surgical problem e.g. pneumonia
Furthermore, patients admitted to hospital with a medical condition (e.g. cardiac failure) may also develop a surgical complication (e.g. perforated duodenal ulcer) that requires surgical expertise and transfer to a surgical team’s care. However, we now recognise that some patients are at particularly high risk of physiological deterioration or developing a complication (Table 1).
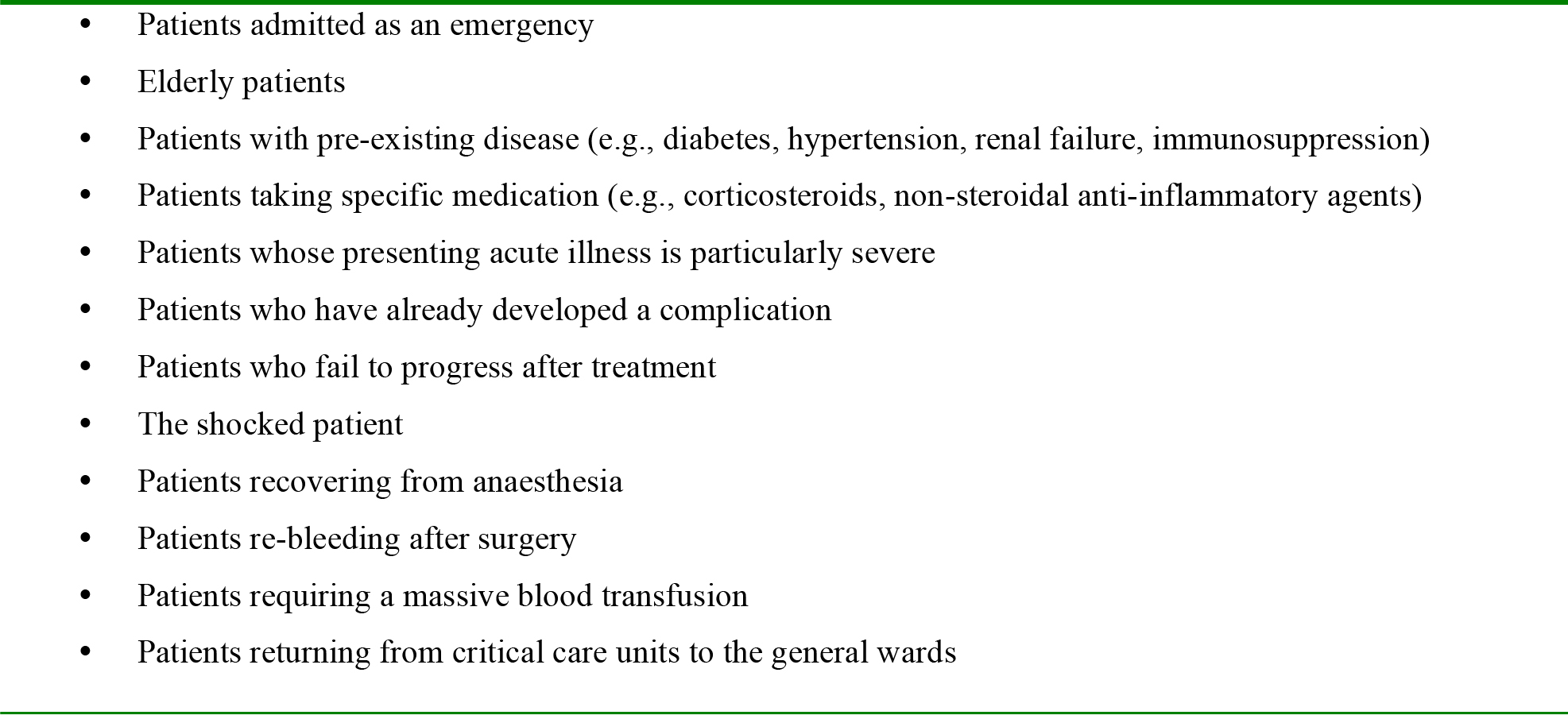
Table 1: Patients at risk of physiological deterioration or of developing a complication
THE CONSEQUENCES OF DEVELOPING ACUTE ILLNESS
Patients who are acutely ill, irrespective of the cause, have a greater chance of physiological deterioration or developing a further complication and the development of a single complication increases the chances of another one. Ultimately, the patient may develop organ failure that requires them to be admitted to the intensive care unit (ICU); in this group of patients, the risk of further complications and in-hospital death rises significantly. Within the UK, patients admitted to an ICU have average ICU and hospital mortality of 20% and 30%, respectively. Although the high mortality rate is influenced by the nature and severity of the underlying pathology, this is not necessarily the sole determinants. Mortality is likely to be higher if the patient has received sub-optimal care or delay before being referred to ICU. Unfortunately, some patients deteriorate to the point of having a cardiac arrest before the severity of their condition is recognised. Once cardiac arrest has occurred overall survival averages around 15%. However, for many patients on general wards whose arrest is secondary to deterioration from an acute illness, the survival rate is much lower.
RECOGNISING THE ACUTELY ILL PATIENT
With the exception of a few, often fatal, conditions such as pulmonary embolism, most acute illnesses develop slowly and signs of physiological decompensation e.g. hypotension, tachycardia, tachypnoea and reduced level of consciousness, are evident for many hours. The signs that a patient is unwell reflect failing cardiovascular, respiratory and neurological systems and numerous studies have identified that these abnormalities are good indicators of impending critical events. Consequently, regular vital sign measurement is fundamental to the early detection of the onset and progression of acute illness. Unfortunately, on most wards outside critical care areas, vital signs measurement occurs infrequently even in sick patients. As a result, there will be a failure to both recognise patient deterioration and act correctly to treat it. Ultimately this may result in cardiac arrest or death. Consequently in the UK, the National Institute for Health and Clinical Excellence (NICE) has recommended that adult patients admitted to hospital, or in whom a clinical decision to admit has been made, should have vital signs observations recorded at the time of their admission or initial assessment. These observations should be monitored at least every 12 hours and that the frequency should increase if abnormal physiology is detected. Using this guidance the aim is to recognise clinical deterioration in most patients and to institute appropriate interventions early.
ASSESSING AND MANAGING THE SICK OR DETERIORATING PATIENT
If you are called to assess a patient who is unwell, you may not have seen him/her previously and may have no prior knowledge of his/her surgical or medical history. Therefore you should have a plan of questions to ask to try and obtain some useful information that you can be thinking about as you attend the ward:
- How old is the patient?
- When were they admitted?
- Do they have a diagnosis, and if so what?
- Are they conscious?
- What are they complaining of?
- How quickly have they deteriorated?
- When and what were their last vital signs?
Underlying principles of assessment:
When assessing and managing any patient, irrespective of the severity of their condition, the immediate aim must be to make the patient safe rather than trying to make a precise diagnosis. Many clinical crises can be managed initially by prompt recognition and correction of a modest number of common abnormalities using simple therapies (e.g., oxygen and fluids). It is logical for all members of the healthcare team to use the same systematic approach to assess and treat the “at risk” or acutely ill patient incorporating:
- Immediate assessment and treatment using an ABCDE approach
- Start simple bedside monitoring
- A full assessment of the patient using all available information
- Decision making
- A definitive management or care plan
- Good record keeping
Key points when dealing with an acutely ill patient
- The aim of initial interventions is to make the patient safe and produce some clinical improvement, such that definitive treatment may be initiated.
- Always correct life-threatening abnormalities before moving on to the next stage of the assessment.
- Resuscitation measures (oxygen, fluids, etc) often take a few minutes to have an effect.
- Call for help early. At every stage of the patient assessment, consider “Do I need help?”
Once resuscitation is underway and the patient has been made safe, undertake a full initial assessment and re-assess regularly to identify the impact of treatment and to detect patient deterioration. Remember, there will be other members of the team around, do not try and do everything yourself. To do this you will need to communicate effectively with everyone; staff, patients and at some point the relatives.
Occasionally there may be several things happening simultaneously and it is important to ensure your own safety and that of the patient; take note of environmental hazards – fluid spillage etc and ensure that needles and other sharps are disposed of safely. Wear protective aprons, gloves and masks to reduce the risk of contamination from secretions and blood. Finally, do not forget that hygiene is important to patient outcome and at all times ensure good hand hygiene and use aseptic techniques for invasive procedures.
INITIAL APPROACH TO THE PATIENT
Once you reach the patient ask them a simple question, such as “How are you”. A normal verbal response immediately informs you that the patient:
- has a patent airway;
- is breathing;
- has brain perfusion with oxygenated blood
If the patient can only speak in short sentences, this suggests severe respiratory distress. Failure to respond to the question suggests they are seriously ill and you should immediately assess the patient for signs of life (listen at the victim’s mouth for breath sounds, look for chest movement, feel for air on your cheek and, if trained to do so, assess the victim’s carotid pulse for not more than 10 sec) whilst keeping the airway open. If the patient has no signs of life, follow the current resuscitation guidelines for cardiac arrest (http://www.resus.org.uk/). Assuming that the patient does respond, the next step is to carry out an ABCDE assessment. At the same time, ask an assistant to attach the following monitors as soon as is safely possible:
- pulse oximeter
- ECG monitor
- Manual or automated blood pressure monitor
The ABCDE system.
- A is for AIRWAY
- B is for BREATHING
- C is for CIRCULATION
- D is for DISABILITY (i.e., central nervous system function)
- E is for EXPOSURE (permitting full patient examination).
The assessment and consequent actions are prioritized in this order because in general airway obstruction will cause death more quickly than a breathing disorder, which in turn will cause death more quickly than blood loss or cardiac dysfunction. Each part of the assessment system has the same aim; to identify immediately life-threatening emergencies and treat them simultaneously. Most abnormalities can be identified using simple clinical examination based on a look-listen-feel approach. The order of the various components of this approach will vary depending on the body system being examined.
Assessing the state of the airway (A)
The aim is to identify and treat airway obstruction. You should always treat airway obstruction as a medical emergency and obtain expert help immediately. Untreated, airway obstruction leads to hypoxia (a lowered PaO2), may damage tissues (e.g. brain, kidneys, heart) and if not relieved will eventually cause cardiac arrest and death. In a critically ill patient, airway obstruction is frequently due to a depressed conscious level, but there are many other causes (Table 2).
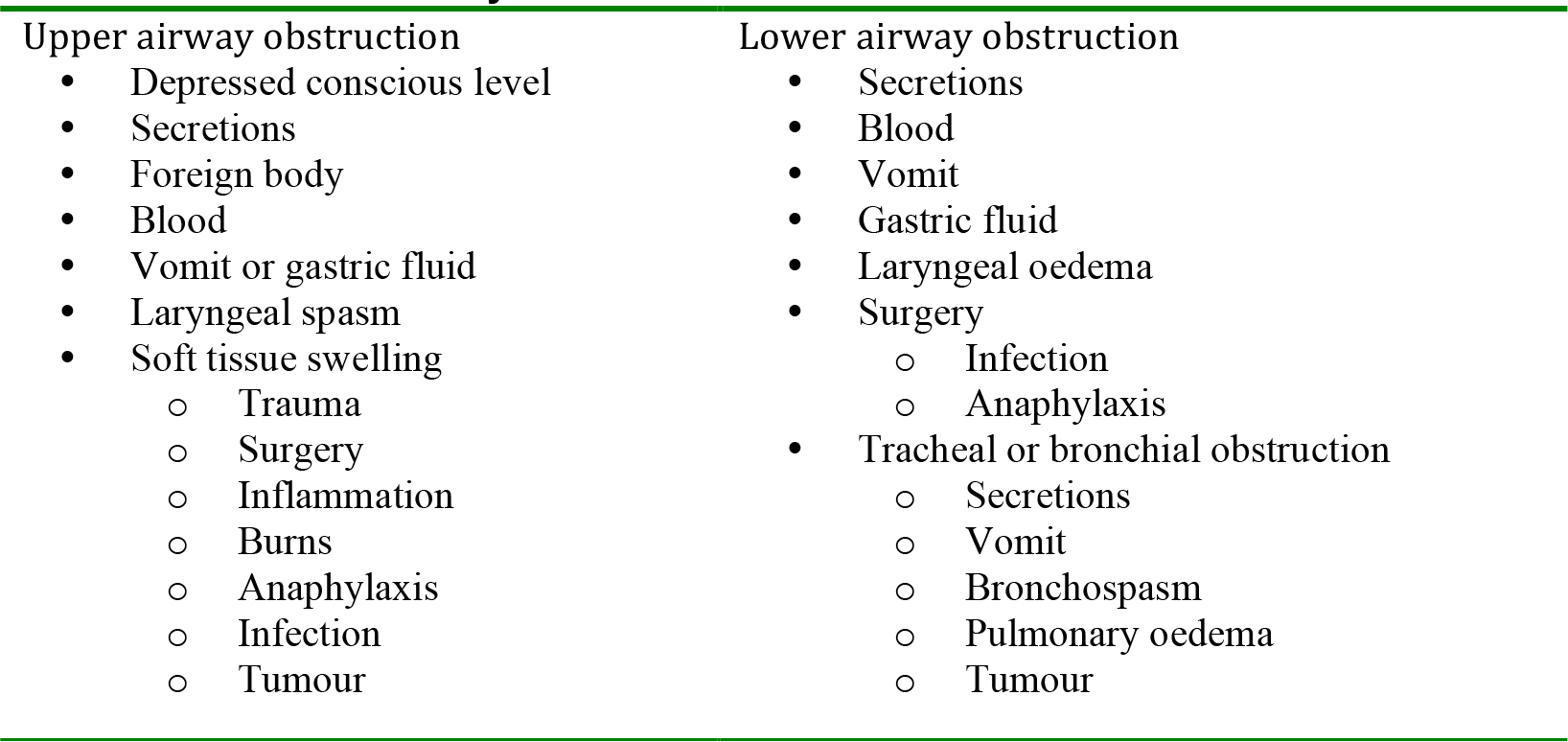
Table 2: Causes of airway obstruction
Look for the signs of airway obstruction:
- Paradoxical chest and abdominal movements (‘see-saw’ respirations)
- Use of the accessory muscles of respiration (e.g., sternomastoid and muscles of the neck, back and shoulder girdle)
- NOTE: central cyanosis is a late sign of airway obstruction
Feel for the presence of air movement at the mouth by placing your face or hand immediately in front of the patient’s mouth.
Listen for the signs of airway obstruction:
- In complete upper airway obstruction, there are no breath sounds at the mouth or nose
- In partial airway obstruction, air entry is diminished and often noisy
- Certain noises assist in localizing the level of the obstruction (Table 3).
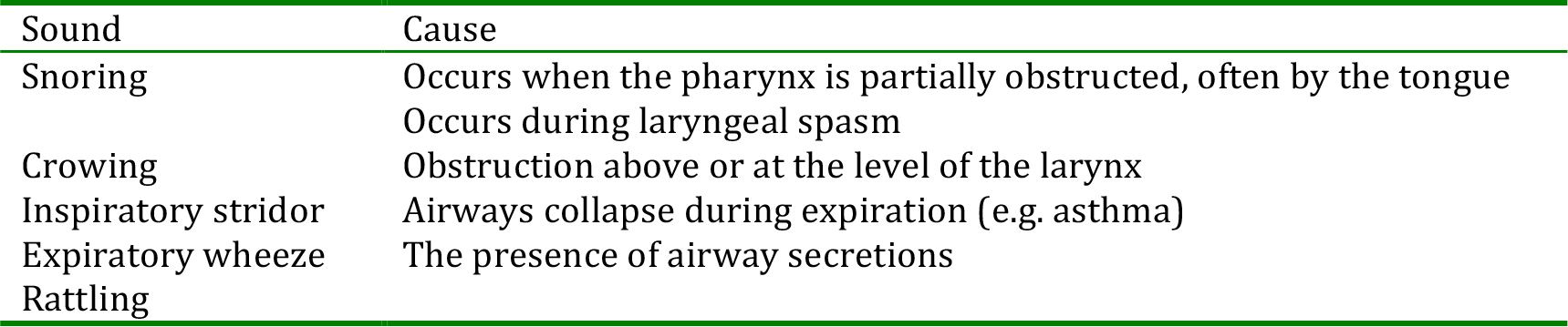
Table 3: The characteristics of airway noises assist in localizing the level of airway obstruction
A patient with signs of airway obstruction must be treated as a medical emergency:
- Call for expert help immediately.
- In most situations, simple methods of airway clearance are all that are required and the use of airway opening manoeuvres (e.g., head tilt and chin lift), airways suction and insertion of an oropharyngeal or nasopharyngeal airway will suffice. If these measures fail, which is a rare occurrence, tracheal intubation may be required, but should not be attempted by inexperienced staff. In many situations, intubation will require the use of sedative and neuromuscular blocking drugs.
- Give oxygen at high concentration. For patients who are acutely ill, use a face mask with an oxygen reservoir. Ensure that the oxygen flow rate is sufficient (usually 10-15 litres per minute) to prevent collapse of the oxygen reservoir during inspiration. This system will deliver approximately 85% oxygen.
- Check that the oxygen saturation is improving and move on rapidly to assess breathing.
Assessing breathing (B)
The aim is to identify and treat immediately life-threatening conditions, e.g., acute severe asthma, pulmonary oedema, infection, massive haemothorax. If untreated, inadequate breathing will lead to hypoxia risking damage to the brain, kidneys and heart. It may also lead to hypercapnia (a raised PaCO2) that can eventually lead to unconsciousness. There are many other causes of disordered or inadequate breathing (Table 4).
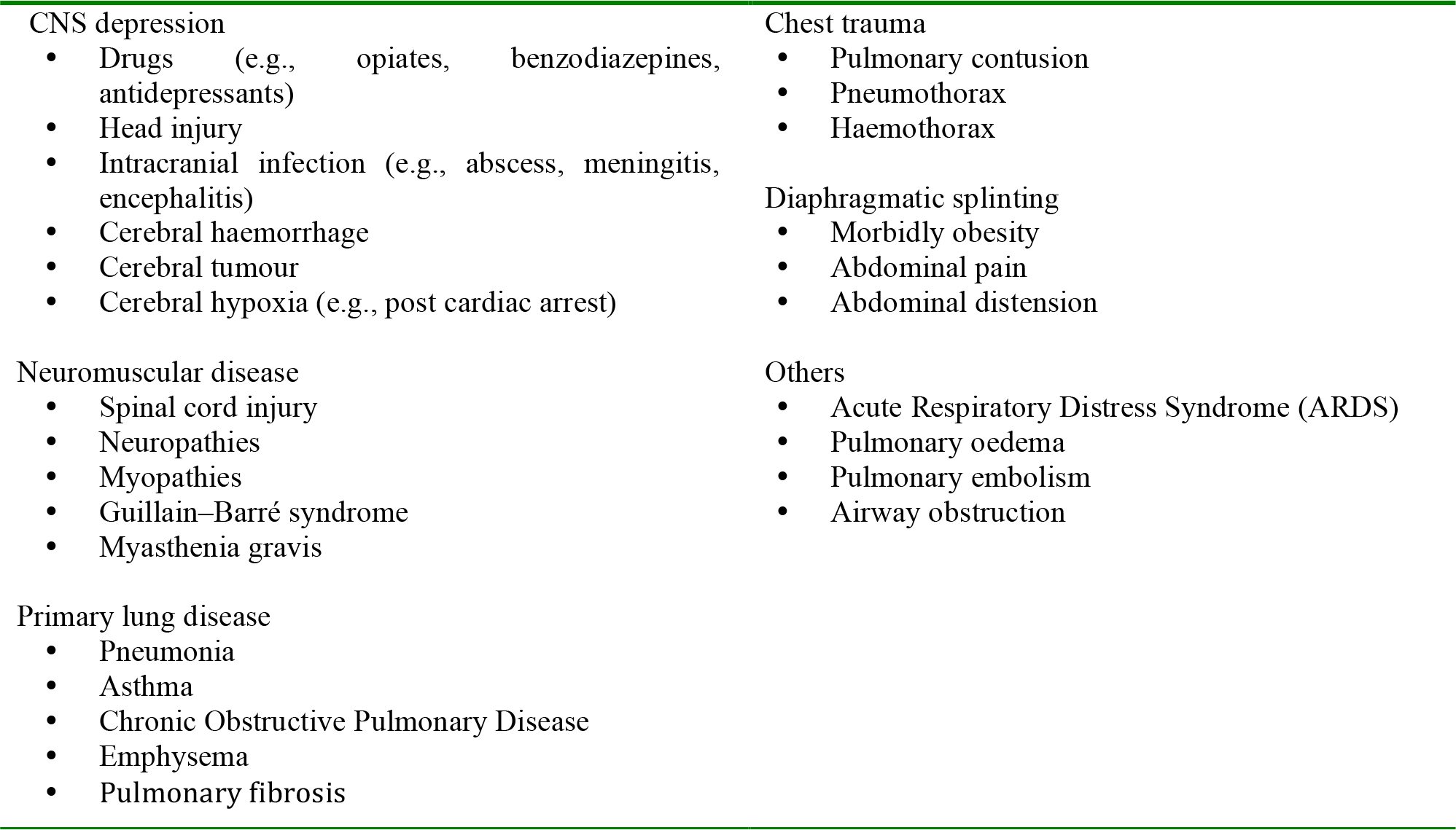
Table 4: Common causes of disordered breathing
Look for the signs of abnormal breathing:
- General signs of respiratory distress – sweating, central cyanosis, use of the accessory muscles of respiration, abdominal breathing
- Count the patient’s respiratory rate. The normal rate is between 12 and 20 breaths per minute. Higher rates, or those that are rising, are markers of illness and should be regarded as a warning that the patient may suddenly deteriorate.
Look and assess the:
- depth of each breath
- pattern (rhythm) of breathing
- equality of movement of the two sides of the chest
Look for the following:
- chest deformity, as this may impair the ability to breathe normally
- raised JVP (may signify acute severe asthma or a tension pneumothorax)
- chest drains – assess if they are patent and draining
- abdominal distension, as this exacerbate respiratory distress by limiting diaphragmatic movement
Feel (palpate) the chest for:
- the position of the trachea in the suprasternal notch. Deviation to one side indicates mediastinal shift (e.g., pneumothorax, lung fibrosis or pleural fluid)
- surgical emphysema or crepitus (assume that this indicates a pneumothorax until proven otherwise).
Feel (percuss) the chest;
- hyper-resonance suggests a pneumothorax; dullness suggests consolidation or pleural fluid (Table 5)
Listen for the signs of breathing problems:
- Listen to the patient’s breath sounds a short distance from his/her face. Rattling or gurgling airway noises indicate the presence of airway secretions, usually due to the inability of the patient to cough sufficiently or to take a deep breath. Stridor or wheeze suggests partial, but significant, airway obstruction.
Listen (auscultate) the chest:
- assess the quality of the breath sounds. Bronchial breathing indicates lung consolidation; absent or reduced sounds suggest the presence of a pneumothorax or pleural fluid.
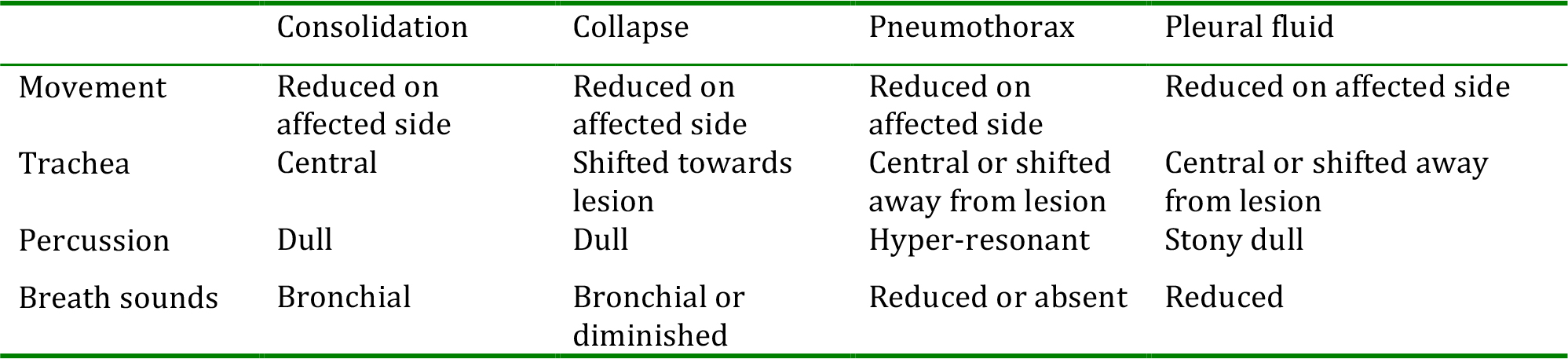
Table 5: Common signs of pulmonary disease
If the patient’s breathing is dangerously inadequate or they are apnoeic, support their ventilation using a bag-mask system, give high concentration oxygen and call for expert help urgently. As soon as possible record the patient’s oxygen saturation (SpO2, normally 97-100%). If possible start to treat the underlying cause of the abnormal breathing, e.g. pulmonary oedema, bronchospasm. For most patients the aim is to raise their oxygen saturation to above 95%. In patients known to be suffering from an acute exacerbation of COPD, once their oxygen saturation reaches 90%, the inspired concentration should be titrated to keep their saturation between 90-92%. In all patients consider sending an arterial blood sample for blood gas analysis if this investigation is available. This will provide useful information on:
- Oxygenation; if the difference between the patient’s PaO2 (kPa) and the inspired oxygen concentration (kPa, approximates to %) is more than 10kPa, there is a defect in oxygen uptake.
- Ventilation; hypercapnia (increased PaCO2) is a result of hypoventilation, hypocapnia reduced PaCO2) is a result of over ventilation.
- Metabolism; sick patients will often have a low pH (due to a metabolic acidosis), as will patients with diabetic ketoacidosis and surgical patients loosing large volumes from the gastrointestinal tract due to diarrhoea or fistulae.
Important points to remember:
- A pulse oximeter does not measure PaCO2 and, therefore, gives no indication of the adequacy of a patient’s ventilation.
- If a patient is receiving oxygen therapy, the SpO2 may be normal, despite inadequate ventilation.
- A “normal” PaO2 (12-14 kPa) whilst breathing 100% oxygen is not normal.
Assessing the circulation (C)
The aim is to identify and treat shock from whatever cause, e.g. severe hyovolaemia, haemorrhage, cardiogenic and septic. If untreated, shock will lead to damage to the vital organs.
Shock can be defined as inadequate perfusion of the vital organs with oxygenated blood
In almost all surgical (and medical) emergencies, hypovolaemia should be considered to be the primary cause of shock, until proven otherwise. Unless there are obvious signs of a cardiac cause, any patient with cool peripheries and a tachycardia should receive intravenous fluid. In surgical patients, haemorrhage (obvious e.g. into drains or hidden e.g. into a body cavity) must be excluded rapidly. Breathing problems such as a tension pneumothorax, can also compromise a patient’s circulatory state, but, ideally, such a cause should have been detected and treated at an earlier stage of the ABCDE assessment.
Look at the colour of the hands and digits.
- are they cyanosed, pink, pale or mottled?
Look the state of the peripheral veins.
- are they under-filled or collapsed, signifying hypovolaemia?
Look for other signs of a poor cardiac output:
- reduced level of consciousness
- oliguria (urine volume < 0.5 ml/kg/hour).
Look for obvious signs of blood or extracellular fluid loss:
- bleeding
- nasogastric or other drain loss
- NOTE: empty drains do not exclude active bleeding. Remember that haemorrhage may be concealed (e.g., intrathoracic, intraperitoneal, pelvic or into gut).
Feel
- assess the limb temperature by feeling the patient’s hands. Are they cool or warm, suggesting poor perfusion?
- measure the capillary refill time (CRT). Apply cutaneous pressure for 5 seconds on a fingertip held at heart level (or just above). Count the time in seconds that it takes for capillary refill (colour to return to the compressed area) once the pressure has been released. Usually, CRT is less than 2 seconds. Remember that CRT may be affected by the environmental temperature.
- a peripheral pulse (usually at the radial artery). Assess for: rate, quality, regularity. A thready pulse suggests a poor cardiac output. A bounding pulse may indicate sepsis.
Listen (auscultate) to the heart:
- a third heart sound may indicate heart failure
- a murmur may indicate valvular disease
- a pericardial rub may suggest pericarditis
If an assistant has not already measured the patient’s blood pressure, it should now be taken. Measure both the diastolic and systolic values. Even in shock, the blood pressure may be relatively normal, as compensatory mechanisms increase peripheral resistance in response to reduced cardiac output. Causes of hypotension are shown in table 6.
It is important to remember that heart rate and blood pressure are related to the situation; a fit young adult will tolerate a heart rate of 60/min and blood pressure of 90/50mmHg, but the elderly patient with cardiovascular disease may be critically ill with the same readings.
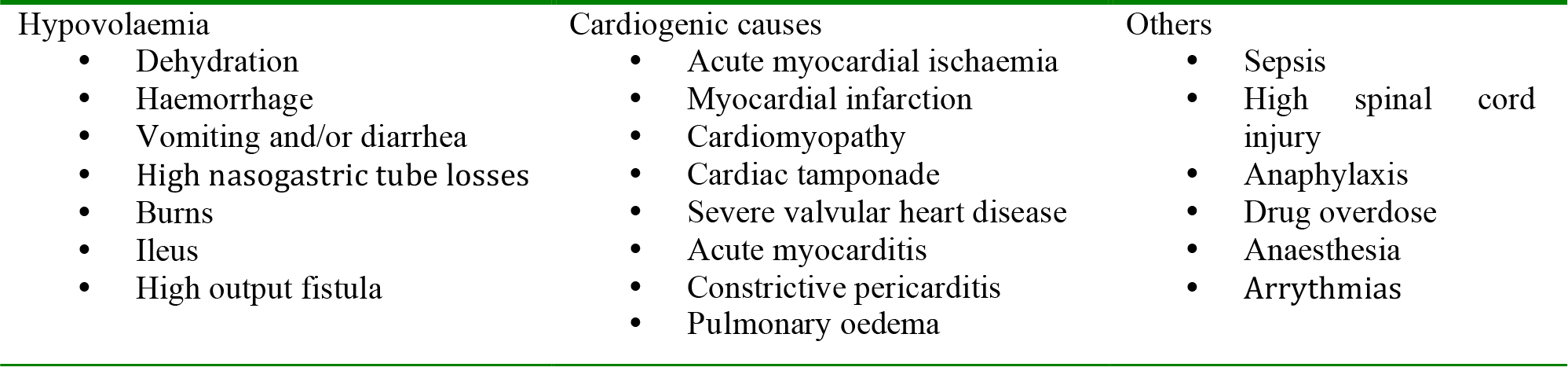
Table 6: Common causes of hypotension
The specific treatment of shock will be determined by the cause, but the initial response should be directed towards:
- Restoration of tissue perfusion using fluid replacement
- Haemorrhage control
Most patients will respond initially to a fluid challenge. In all cases, insert one or more large (14 or 16g) intravenous cannulae. Use short, wide-bore cannulae, as they have the highest flow rate. Remember to take blood from the cannula for routine investigations; full blood count (FBC), ESR, urea, electrolytes, coagulation studies, microbiological investigations and blood grouping and cross-matching. Attach the fluid and give a rapid fluid challenge (over 5-10 minutes):
- 500mls of warmed crystalloid solution, if the patient has a SBP> 100mmHg
- 1000mls of warmed crystalloid solution, if the patient has a SBP< 100mmHg
- 250 mls of warmed crystalloid solution, if the patient has pre-existing cardiac failure.
Reassess and document the pulse rate and BP regularly (every 5 minutes), watching for signs of improvement; decrease in pulse rate, increase in BP, increase in level of consciousness. Consider insert a urinary catheter, an output of 50-100ml/hr suggests adequate perfusion. Patients with known cardiac failure should receive closer monitoring; listen to the chest for crepitations after each bolus, consider a CVP line and if possible an arterial line. If the patient shows no signs of improvement, the fluid challenge can be repeated, but consider the following:
- Massive or ongoing blood loss
- Septic shock
- Cardiogenic shock
If symptoms and signs of cardiac failure (dyspnoea, increased heart rate, raised JVP, a third heart sound and pulmonary crepitations on auscultation) occur, the rate at which fluid is being given should be reduced or the fluids stopped altogether. Seek expert help as alternative means of improving tissue perfusion will be required:
- inotropes to increase myocardial contractility
- vasodilators to reduce afterload
- nitrates or diuretics to reduce the preload to the left ventricle.
Important points to remember:
- Resting heart rate is normally lower than systolic blood pressure.
- In some patients, e.g., those with gastro-intestinal or intra-abdominal haemorrhage, immediate surgery may be required as the only effective form of resuscitation.
- Even patients with cardiac disease can suffer from hypovolaemia and may benefit from careful use of intravenous fluids.
Assessing neurological state – disability (D)
The aim is to asses the patient’s conscious level and if reduced, identify and treat the cause. Common causes of unconsciousness include profound hypoxaemia, hypercapnia, cerebral hypoperfusion, or the recent administration of sedatives or analgesic drugs (Table 7). Ideally, such causes should have been detected and treated at an earlier stage of the ABCDE assessment.
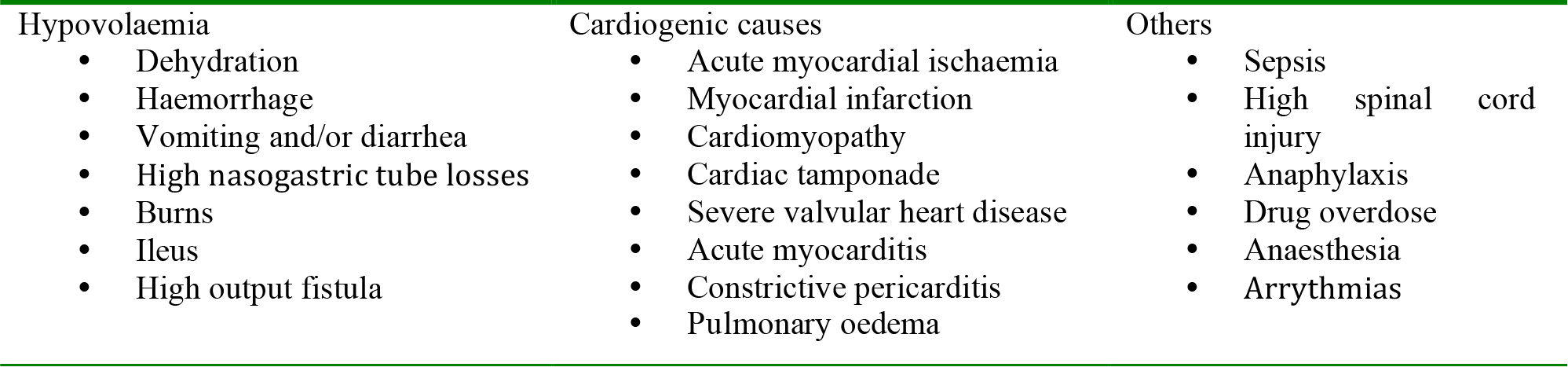
Table 7: Common causes of a decreased conscious level
Look at the pupils and check their :
- size and reactivity to light
- small, pinpoint pupils and reactive: opioids, pontine haemorrhage
- mid-sized, unreactive; midbrain lesion
- widely dilated, unreactive; severe brain ischaemia, hypoglycaemia, brainstem lesion, postictal, tricyclic antidepressant drugs overdose, recent intravenous administration of adrenaline
- unilateral dilatation, unreactive; intracerebral haematoma)
Check the patient’s drug chart for reversible drug-induced causes of depressed consciousness. Administer the appropriate antagonist, where available, e.g. naloxone for opioids.
Look and listen to assess the patient’s conscious level using either the AVPU or Glasgow Coma Scales (GCS, see Table 8). Record the best response. The highest GCS score is 15 and the lowest 3. Patients in a coma have a GCS score of 8 or less; they have no eye-opening (1), have no recognisable speech (2) and do not obey commands (5).
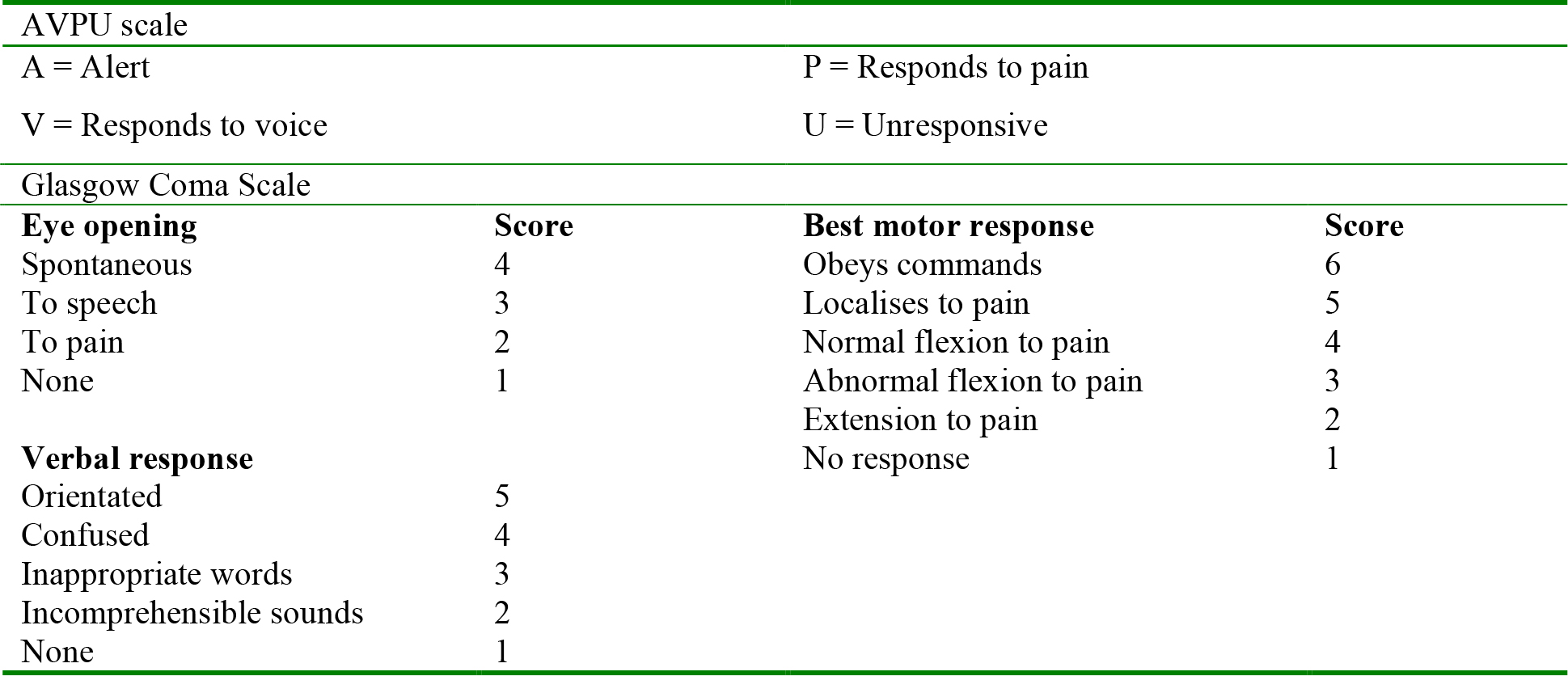
Table 8: Assessing the patient’s level of consciousness
Measure the blood glucose, if possible using a rapid bedside method, to exclude hypoglycaemia. If below 3mmol/l, administer 25-50ml of 50% glucose solution intravenously.
Patients with a reduced level of consciousness are at risk of developing airway obstruction in the supine position. In addition, airway protective reflexes may be insufficient to prevent inhalation of secretions, vomit or blood. Until help can be obtained to secure their airway, nurse these patients in the recovery position.
Exposure/Examination (E)
The aim is to carry out a full examination of the patient, head-to-toe, back and front. In order to achieve this and detail is not missed, full exposure of the body may be necessary. Do this in a way that respects the dignity of the patient and prevents heat loss. At this stage of the assessment, the examination should be focused on the most likely area of the body causing the patient’s poor condition (e.g., for a patient presenting with hypovolaemia following laparotomy, this would be the abdomen).
Next stages:
The underlying aim of your intervention so far has been a “holding measure” that keeps the patient alive, and produces some clinical improvement, in order that definitive treatment may be initiated. Even if the patient’s vital signs are still abnormal, they should be moving in a direction of improvement. At this point, gather more information about the patient.
- Take a full clinical history from the patient, his relatives or friends and other staff. Co-morbid conditions (e.g., hypertension, diabetes mellitus) can have a significant impact upon a patient’s response to critical illness, and must not be overlooked.
- Perform a full examination of the patient, using a traditional clinical examination format.
- Review the patient notes and charts. Although the charts may appear to carry an overwhelming amount of data, they can be assimilated by systematic analysis.
- Study both absolute and trended values of vital signs.
- Check that important routine medications are prescribed and being administered.
- Review the results of laboratory or radiological investigations.
- Consider if you have a credible diagnosis that accounts for the patient’s condition and recent deterioration.
- If yes, consider the definitive treatment of the patient’s underlying condition.
- If no, re-assess the patient in case you have missed important detail or in case the patient’s condition has progressed since your last assessment. Involve more senior colleagues
- Make complete entries in the patient’s notes of your finding, assessment and treatment. Record the patient’s response to therapy. Make sure that your entry in the notes is legible, signed, dated and timed.
- Consider which level of care is required by the patient (e.g., ward, HDU, ICU). This may be dictated by your hospital’s policies or the local facilities available.
COMMUNICATING INFORMATION ABOUT PATIENT DETERIORATION
The system described so far will allow you to recognise, assess and start treatment of the acutely ill patient. However, it is almost inevitable that you will at some point need senior help. The key to getting this help in a timely and successful manner is good communication.
- Use a system for communicating patient deterioration. A suggested system is to use the term RSVP.
- R = Reason for calling
- S = Story
- V= Vital signs (plus any early warning score)
- P = Plan
- Know the objectives of the call. Why are you calling?
- Do you want a more senior colleague to assess the patient?
- Are you calling for advice?
- Do you think the patient needs an operation?
- Be assertive when communicating, but be careful to avoid aggression. Sentences such as “I have done all I can and I am unsure of what to do next” or “I am concerned that I may be missing something” are likely to assist in obtaining help.
- Before making the call, gather all the useful information together.
- What is known about the patient
- What the patient was like when you first arrived
- What you have done so far
- What the response has been
- What you have found on subsequent examination or investigations
- Get the message across in first two sentences, e.g.:
- This is __________ I apologise for disturbing you, but Mr X is deteriorating and I think that he may need an urgent operation.
SUMMARY
With a few exceptions, most acute illnesses develop slowly and are accompanied by deterioration in the patient’s physical signs that in retrospect have been evident for many hours. The signs that a patient is unwell reflect failing cardiovascular, respiratory and neurological systems and numerous studies have identified that these abnormalities are good indicators of impending critical events. Early recognition and response to these changes using an ABCDE system will keep the patient from harm while help is obtained to make a definitive diagnosis and treat the patient without them coming to further harm.
BIBLIOGRAPHY
- McQuillan P, Pilkington S, Allan A, Taylor B, Short A, Morgan G, et al. Confidential inquiry into quality of care before admission to intensive care. BMJ 1998; 316: 1853-8.
- McGloin H, Adam SK, Singer M. Unexpected deaths and referrals to intensive care of patients on general wards. Are some cases potentially avoidable? J R Coll Physicians Lond 1999; 33: 255-9.
- Smith GB, Poplett N. Knowledge of aspects of acute care in trainee doctors. Postgrad Med J 2002; 78: 335- 8.
- Smith GB, Osgood VM, Crane S. ALERT–a multiprofessional training course in the care of the acutely ill adult patient. Resuscitation 2002; 52: 281-6.
- Hodgetts TJ, Kenward G, Vlackonikolis I, Payne S, Castle N, Crouch R, et al. Incidence, location and reasons for avoidable in-hospital cardiac arrest in a district general hospital. Resuscitation 2002; 54: 115- 23.
- Kause J, Smith G, Prytherch D, Parr M, Flabouris A, Hillman K. A comparison of antecedents to cardiac arrests, deaths and emergency intensive care admissions in Australia and New Zealand, and the United Kingdom–the ACADEMIA study. Resuscitation 2004; 62: 275-82.
- Andrews T, Waterman H. Packaging: a grounded theory of how to report physiological deterioration effectively. J Adv Nurs 2005; 52: 473-81.
- Perkins GD, Barrett H, Bullock I, Gabbott DA, Nolan JP, Mitchell S, et al. The Acute Care Undergraduate TEaching (ACUTE) Initiative: consensus development of core competencies in acute care for undergraduates in the United Kingdom. Intensive Care Med 2005; 31: 1627-33.
- DeVita MA, Bellomo R, Hillman K, Kellum J, Rotondi A, Teres D, et al. Findings of the first consensus conference on medical emergency teams. Crit Care Med 2006; 34: 2463-78.
- Esmonde L, McDonnell A, Ball C, Waskett C, Morgan R, Rashidian A, et al. Investigating the effectiveness of critical care outreach services: a systematic review. Intensive Care Med 2006; 32: 1713-21.
- Gao H, McDonnell A, Harrison DA, Moore T, Adam S, Daly K, et al. Systematic review and evaluation of physiological track and trigger warning systems for identifying at-risk patients on the ward. Intensive Care Med 2007; 33: 667-79.
- Winters BD, Pham JC, Hunt EA, Guallar E, Berenholtz S, Pronovost PJ. Rapid response systems: A systematic review. Crit Care Med 2007; 35: 1238-43.
- McDonnell A, Esmonde L, Morgan R, Brown R, Bray K, Parry G, et al. The provision of critical care outreach services in England: findings from a national survey. J Crit Care 2007; 22: 212-8.
ACKNOWLEDGEMENT
The authors would like to express their gratitude to Wiley-Blackwell for permission to reproduce material from Gwinnutt C. Lecture Notes Clinical Anaesthesia, 3rd ed. Oxford: Wiley-Blackwell, 2008.
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/