Obstetrics Anaesthesia

PREFACE
This is the first of a series of obstetric anaesthetic case based discussions. The clinical cases presented include a number of challenges that require consideration of different management strategies. We hope the cases represent ‘real life’ clinical situations. Throughout the progress of each case, guidance and good practise is discussed. We hope these case discussions will complement the understanding of specific areas of obstetric anaesthesia. As in all clinical cases there are often a number of approaches that can be taken and the way each case is ultimately managed, does not necessarily represent the only management strategy.
Matt Rucklidge
Editor, Obstetric Anaesthesia
INTRODUCTION
A 28 year old woman in her first pregnancy is admitted to the labour ward at 38 weeks of gestation. She has no past medical history of significance. Her blood pressure when pregnancy was first confirmed at 8 weeks was 120/70. Today she presents with a mild frontal headache and increasing swelling of her ankles. Blood pressure is 170/120, urine dip stick testing shows 3+ of protein and there is oedema of both ankles to the mid-calf.
What is the most likely reason for these clinical signs?
What other symptoms and signs should be looked for?
What investigations should be performed?
Pre-eclampsia is the most likely diagnosis. Pre-eclampsia is a multisystem disorder which occurs after 20 weeks of pregnancy with variable features, severity and rates of progression.
There are a number of definitions of hypertension in pregnancy which lack consistency and can be confusing.
In essence, high blood pressure in pregnancy can be:
- Pre-existing hypertension
- Pregnancy induced hypertension
- Pre-eclampsia
Most definitions of hypertension in pregnancy are based on a diastolic BP > 90mm Hg on two occasions or diastolic >110 mm Hg on one occasion.
Failure to record and treat systolic hypertension in women with severe pre-eclampsia was highlighted as a common problem in the most recent Confidential Enquiry into Maternal and Child Health (CEMACH). Treatment was recommended if the systolic BP was > 160 mmHg, on two consecutive readings at least 4 hours apart.
Some definitions of hypertension rely on a rise in BP, rather than an absolute value, e.g. a rise in systolic BP of 30 mm Hg, or diastolic BP of 25 mm Hg above the earliest BP taken in pregnancy.
It is essential to monitor blood pressure closely throughout pregnancy and to identify other signs and symptoms suggestive of pre-eclampsia. The distinction between pregnancy induced hypertension and pre-eclampsia is important since pre-eclampsia is associated with a worse outcomes. Pregnancy induced hypertension, like pre-eclampsia, occurs in the second half of pregnancy, but without proteinuria or other signs of pre-eclampsia.
Symptoms that should be looked for to diagnose pre-eclampsia include:
- Headache
- Visual disturbance
- Epigastric pain / right upper quadrant pain
- Nausea / vomiting
- Increasing swelling of legs, fingers, face.
Signs to identify include:
Cardiovascular system: hypertension, vasoconstriction leading to cool peripheries, peripheral oedema
Respiratory system: pulmonary oedema, facial and laryngeal oedema, acute respiratory distress syndrome (ARDS)
Renal system: proteinuria, oliguria, acute renal failure
Central nervous system: hyperreflexia, clonus, cerebral haemorrhage, convulsions (eclampsia), papilloedema, coma
Others: HELLP (Haemolysis, Elevated Liver Enzymes and Low Platelets), thrombocytopenia, DIC (disseminated intravascular coagulopathy)
Fetal signs include: CardioTocoGraphy (CTG) abnormalities, pre-term labour, and intrauterine growth retardation.
Investigations include:
Urine: proteinuria demonstrated by: urine dipstick (1+ = 0.3 g/l, 2+ = 1 g/l and 3+ = 3 g/l) and 24hr collection of urine. More recently, urine protein: creatinine ratio (PCR): a PCR > 30 is significant. Assessment of urine output is important.
Blood: Full blood count, urea and electrolytes, clotting, uric acid, liver function tests, magnesium, serum calcium, Group and save.
Regular assessment of fetal well-being using CTG, ultrasound scan to assess fetal growth and uterine artery Doppler blood flow to assess placental blood flow.

She is reviewed by a junior obstetrician and moved into a room with equipment for cardiovascular monitoring. A 14G intravenous cannula is inserted and the above bloods are sent to the laboratory.
Continuous CTG monitoring is commenced. She complains that her headache is worsening and she is seeing flashing lights. She is found to be hyper-reflexic and she is given a dose of oral labetalol 200mg. At this stage her BP is being monitored every 15mins and despite the oral antihypertensive her BP remains high at 170/120 two hours later.

She is reviewed by a senior obstetrician and anaesthetist and it is decided to commence an IV antihypertensive agent.
What IV antihypertensive drugs are suitable in this case?
Control of acute hypertension in pre-eclampsia may be achieved by:
- Labetalol bolus – 25mg IV bolus (5ml of 5mg/ml neat solution) over at least 1 minute
- Repeat above at 15 minute intervals to a maximum dose of 200mg until blood pressure is controlled and then start infusion:
- Labetalol maintenance infusion – dilute 200mg (40ml of 5mg/ml neat labetalol with 10 ml 0.9% sodium chloride (giving a final concentration of 4mg/ml)
- Commence infusion at 5ml/hr (20mg/hr)
- Double infusion rate every 30 min to maximum 40ml/hr (160mg/hr)
- Titrate to keep diastolic between 90 – 100mmHg
Labetalol should be avoided in women with asthma.
If the woman remains hypertensive on maximum rate or Labetalol is contraindicated or causing side effects, add / replace with a Hydralazine infusion.
- Hydralazine bolus– Dilute 40mg Hydralazine in 40mls Normal Saline to give a concentration of 1mg/ml
- Give 5mls (5mgs) slowly (e.g. over 15 minutes using an infusion pump set at 20mls/hr)
- Check BP. After 20 minutes, if diastolic >100mmHg give further 5mls (5mg) over 15 minutes (pump rate 20mls/hr)
- When diastolic 90 – 100 mmHg commence maintenance infusion.
- Hydralazine infusion: Using same concentration as above set pump rate to 5ml/hr (5mg/hr)
- Titrate to keep diastolic 90 -100 mmHg and systolic 140 -150 mmHg
- Usual maintenance dose is 2-3ml/hr (2-3mg/hr)
- Maximum dose 18ml/hr (18 mg/hr)
- Reduce if significant side effects (see below) or maternal tachycardia >130 bpm
Hydralazine –causes headache, tremor, nausea and tachycardia and may be less well tolerated than labetalol.
- A fluid bolus of 250ml should be considered before commencing IV antihypertensive therapy as there is some evidence that this may avoid the hypotension observed with initiation of vasodilator therapy.
Given the severity of this woman’s symptoms, measures to control BP with an IV agent should have been considered earlier in this case.
A bolus dose of labetalol is given, followed by a continuous infusion of labetalol and her BP starts to stabilise and her diastolic falls to 90mmHg. A litre of Hartmann’s solution (Ringers lactate) is commenced at a rate of 85ml/hr, aiming for urine output of >100ml in 4 hours (excessive fluid administration is harmful in severe pre-eclampsia and fluids should be restricted).
Observations of BP, oxygen saturations, heart rate and respiratory rate are performed every 15 minutes along with continuous CTG monitoring.
While considering a plan for delivery she has a grand mal fit.
What is the most likely reason for the fit?
How should it be managed?
The fit is most likely to be an eclamptic seizure.
Other causes of a fit in this situation include:
- Epilepsy
- Intracranial event (e.g. subarachnoid haemorrhage, cerebrovascular accident)
- Vaso-vagal (may be caused by rapid fall in BP due to treatment)
- Hypoglycaemia
Management of an eclamptic seizure:
- The patient should be turned to the left lateral position
- Call for help
- Assess and support Airway, Breathing and Circulation
- High flow oxygen by face mask
- Obtain IV access
- Treat with IV magnesium sulphate (see below)
- Monitor ECG, BP, respiratory rate and oxygen saturations
- Check blood sugar
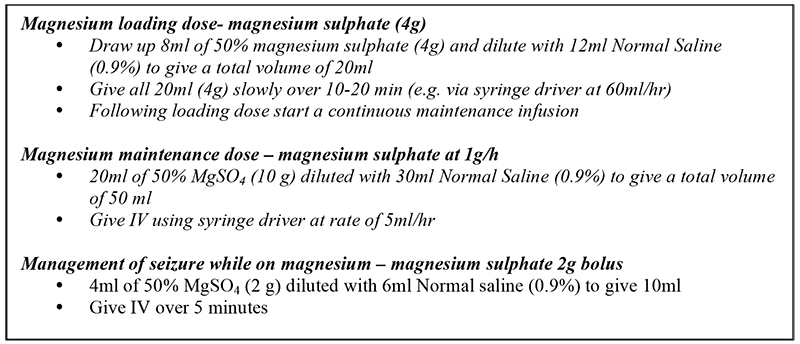
It is beneficial for obstetric departments to set up an “eclamptic box” for use in this kind of emergency. Within the box is stored: magnesium sulphate, normal saline, syringes, needles and instructions for the correct dose and administration. This will improve the timely administration of magnesium and reduce errors in dosing and administration.
Would earlier administration of magnesium have reduced the risk of fitting in this particular case?
The drug of choice to manage eclampsia and reduce subsequent fits is magnesium sulphate. The use of magnesium to prevent seizures in women with pre-eclampsia is less clear.
Guidelines on the management of pre-eclampsia by the Royal College of Obstetricians and Gynaecologists (RCOG) in 2006, recommended prophylactic magnesium sulphate should be considered for women with severe pre-eclampsia for whom there is concern about the risk of eclampsia. This is based on the Magpie Trial. This study showed that magnesium sulphate given to women with pre-eclampsia reduced the risk of an eclamptic seizure by around 58%. It should be noted however that not all women with pre-eclampsia will progress to eclampsia; only 1–2% of women in the UK with pre-eclampsia will fit in the absence of anticonvulsant treatment. The Magpie trial calculated that the number of pre-eclamptic women needed to be treated with magnesium to prevent one of them from fitting is 91 (i.e. of 91 pre-eclamptics receiving magnesium, 1 would gain benefit by not fitting while 90 will derive no benefit from its administration and may be at risk of its side effects.)
A bolus dose of magnesium is administered and she is commenced on an infusion of magnesium at a rate of 1g/h. Her respiratory rate and reflexes are checked regularly. She is nursed in the left lateral position.
The CTG now demonstrates repetitive and severe fetal heart rate decelerations.
She is reviewed by the senior obstetrician and a decision is made for an emergency delivery by Caesarean section (category 1). The anaesthetist attends to make a plan for anaesthesia.
What is the most appropriate anaesthetic technique? GA or Regional?

Regional anaesthesia is not contraindicated after an eclamptic fit if the mother has regained consciousness and treatment for seizures and BP control has been commenced. If an epidural has already been in place for labour, this can be topped up as long as it has been effective. If there is no epidural (as in this case) or it is considered that there is not enough time to top up the epidural, spinal anaesthesia should be provided.
The benefits of spinal anaesthesia include provision of a rapid, dense and predictable block suitable for surgery while avoiding general anaesthesia which has the risk of BP surges due to the pressor response of laryngoscopy, intubation and extubation.
There have been concerns with spinal anaesthesia and severe pre-eclampsia due to the fear of causing a sudden and significant drop in BP. This fear appears unfounded because women with pre-eclampsia have high levels of circulating catecholamines which may protect them against a fall in BP as a result of a spinal induced sympathetic block. If a spinal technique is chosen there should be cautious use of vasopressors as an exaggerated hypertensive response to vasopressors may be observed.
Sometimes a regional block may be contraindicated, for example: maternal refusal, coagulopathy, thrombocytopenia and poorly controlled seizures or there is no time because of severe fetal distress. In these cases general anaesthesia will have to be undertaken.

The factors which make general anaesthesia in pre-eclampsia particularly hazardous include:
- the increased risk of difficult airway and intubation
- marked pressor response at laryngoscopy, intubation and extubation resulting in dangerous surges in blood pressure
There is a significant risk of intracranial haemorrhage secondary to uncontrolled severe hypertension at induction of general anaesthesia. Therefore in patients who require general anaesthesia, BP and convulsions should be maximally controlled and ideally, invasive monitoring inserted prior to induction of general anaesthesia. A senior anaesthetist should be present to manage these challenging cases.
The blood tests which were sent earlier are now available and demonstrate a platelet count of 55×109/l. She is assessed by the anaesthetist and consented for a general anaesthetic. A thorough assessment of her airway is performed and she denies any history of stridor, voice change or hoarseness.
She is transferred to theatre and full monitoring is attached to the patient. An arterial line is inserted prior to induction. She is pre-oxygenated in the left tilted position and a rapid sequence induction is performed with thiopentone 450mg and suxamethonium 100mg. No other drugs are administered prior to laryngoscopy. The trachea is intubated after 45 seconds with a size 7 endotracheal tube at which point her BP surges to 240/140. Anaesthesia is maintained with isoflurane in nitrous oxide and oxygen and she is paralysed with atracuruim 40mg. After delivery of the baby she is given morphine 10mg and prophylactic antibiotics.
At the end of the caesarean section she is slow to wake up.
How can you obtund the pressor response to laryngoscopy and intubation?
What might be the cause of her slow recovery?

The response to laryngoscopy can be obtunded by the following:
- A short acting opiate bolus (e.g. alfentanil 10-20mcg/kg or remifentanil 1 mcg/kg)
- A bolus dose of labetalol 10-20mg i.v
- Bolus of magnesium 40 mg/kg i.v
- Bolus of lidocaine 1.5mg/kg i.v 3-5 min before induction
If opiates are given prior to delivery, inform the neonatal team of the possibility of neonatal respiratory depression.
There are several reasons why she is slow to wake up and these include:
- Effect of excess anaesthetic agents
- Effect of excess opiates
- Inadequate reversal of neuromuscular block: magnesium potentiates non-depolarising neuromuscular
- blocking drugs
- Respiratory depression due to magnesium toxicity
- Hypoglycaemia
The most concerning possibility is that she has experienced an intracranial event due to excessive hypertension during intubation. This should be diagnosed by pupil examination and response and emergency CT scan.
Fortunately, over the next 15 minutes she slowly wakes and makes an uneventful recovery from her general anaesthetic.
What on-going management of her pre-eclampsia should be continued?
After her caesarean section this lady should go to a high dependency area for close observation and blood tests.
It is important she also has:
- Effective postoperative analgesia as this reduces the stress response and consequent hypertension caused by poorly controlled pain; however NSAIDs should be avoided until proteinuria has resolved and there is no evidence of impairment of renal or platelet function.
- Ongoing anti-hypertensive therapy. This should be continued after the delivery as dictated by her blood pressure. Although blood pressure usually falls initially after delivery it may rise again around 24 hours postpartum. IV antihypertensive therapy should be converted to oral therapy with further reductions made in a stepwise fashion.
- Close monitoring must continue as she is at risk of further eclamptic seizures. Magnesium therapy should be continued until 24hrs after her delivery (or the last convulsion, whichever is the later).
- Cautious fluid intake. She should continue with a total of 85ml/h of fluids (subtracting oral intake from IV prescription). Fluid overload must be avoided and transient rises in plasma urea and creatinine concentrations are acceptable in the short term as a spontaneous dieresis is usual within 1-2 days of delivery.
Most women with severe pre-eclampsia or eclampsia will need inpatient care for 4 days or more following delivery.
Further reading
- The management of severe preeclampsia/eclampsia. Royal College of Obstetricians and Gynaecologists. Guideline no.10a. http://www.rcog.org.uk/files/rcog-corp/uploaded files/GT10aManagementPreeclampsia2006.pdf
- Aya AG et al. Patients with severe preeclampsia experience less hypotension during spinal anaesthesia for elective caesarean delivery than healthy parturients: a prospective cohort comparison. Anesth Analg 2003; 97: 867-72
- Hart E, Coley S. The diagnosis and management of pre-eclampsia. Continuing Education in Anaesthesia Critical Care and Pain Medicine 2003; 3: 38- 42
- Obstetric Anaesthesia (Oxford Specialist Handbooks in Anaesthesia) Edited by Paul Clyburn, Rachel Collis, Sarah Harries, Stuart Davies. Oxford University Press 2008. ISBN 978-0-19- 920832-6
- Ngan Kee WD et al. Maternal and neonatal effects of remifentanil at induction of general anesthesia for cesarean delivery: a randomized, double-blind, controlled trial. Anesthesiology 2006; 104:14-20
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/