General Topics

This tutorial will detail the factors that determine how local anaesthetic spreads within the CSF therefore determining the extent of the block.
Mechanisms of drug spread
The CSF of the vertebral canal occupies the narrow (2-3 mm deep) space surrounding the spinal cord and cauda equina, and is enclosed by the arachnoid mater. As the local anaesthetic solution is injected, it will spread initially by displacement of CSF and as a result of any currents created within the CSF. The next stage may well be the most crucial, and is spread due to the interplay between the densities of both CSF and local anaesthetic solution under the influence of gravity. Gravity will be ‘applied’ through patient position (supine, sitting, etc) and, in any horizontal position, by the influence of the curves of the vertebral canal. Many factors are said to affect these mechanisms.
What factors may affect how far the local anaesthetic spreads?
CHARACTERISTICS OF THE INJECTED SOLUTION
- Baricity
- Volume / Dose / Concentration
- Temperature of injectate
- Viscosity
- Additives
CLINICAL TECHNIQUE
- Patient position
- Level of injection
- Needle type / Alignment
- Intrathecal catheters
- Fluid currents
PATIENT CHARACTERISTICS
- Age
- Height
- Weight
- Sex
- Intra-abdominal pressure
- Spinal anatomy
- Lumbosacral CSF volume
- Pregnancy
The key factors are the physical characteristics of CSF and the solution injected, the clinical technique used and the patient’s general features. These inter-relate in complex ways. Once bulk spread of the injectate under the influence of the physical forces outlined above is complete, the final stage will be diffusion of drug through the CSF and into the nervous tissue.
The way a local anaesthetic moves in the CSF is determined by its “heaviness”. This is variably described in terms of baricity, density and specific gravity? Can you define them?
CSF characteristics
CSF is an isotonic, aqueous medium with a constitution similar to interstitial fluid. The terms density, specific gravity and baricity define its physical characteristics, but are often used inaccurately causing confusion. Precise definitions are:
- i) Density: the ratio of the mass of a substance to its volume. It varies with temperature, which must be specified.
- ii) Specific gravity: the ratio of the density of a substance to a standard. It is usual to relate local anaesthetic solutions at 20°C to water at 4°C.
- iii) Baricity: analogous to specific gravity, but expressed as a ratio of the densities of local anaesthetic and CSF, both at 37°C.
The units of density are weight per unit volume, but the other two, being ratios, have no units. At 37°C the mean density of CSF is 1.0003, with a range of 1.0000-1.0006 (± 2 SD) g/litre. Given the normal variation, it is necessary that solutions which are to be predictably hypobaric or hyperbaric in all patients have baricities below 0.9990 or above 1.0010 respectively. Most glucose-free solutions used intrathecally are slightly hypobaric, but behave in a hyperbaric manner if cooled to 5°C before injection (explained later). Plain bupivacaine has a baricity of 0.9990, which means that it is only just on the edge of being hypobaric.
CSF density is lower in women than men, in pregnant than non-pregnant women, and in premenopausal women than postmenopausal women and men. Theoretically, these differences could lead to differences in the movement of a particular solution in the various patient groups but the differences between groups are small and probably clinically unimportant.
FACTORS AFFECTING INTRATHECAL SPREAD
Characteristics of the injected solution
Baricity
While various techniques have been used to alter the baricity of local anaesthetics, the addition of glucose is the only one to remain in routine use. The usual choice for the clinician is between a hyperbaric solution and one with a baricity at, or just below, that of CSF. Hyperbaric solutions are more predictable, with greater spread in the direction of gravity and less variability. In contrast, most plain solutions exhibit greater variability in effect and are less predictable, so that the block may either be too low, and inadequate for surgery, or excessively high, and cause side-effects. The greater mean spread of hyperbaric solutions may be associated with an increased incidence of cardiorespiratory side effects, although this is not always the case, and may depend on the concentration of the glucose. Commercially available solutions contain up to glucose 8%, but most of the evidence shows that any concentration in excess of 0.8% will produce a solution that behaves in a hyperbaric manner, but with less spread if the glucose concentration is at the lower end of the range. Hyperbaric solutions can be made by adding 5% dextrose to plain bupivacaine.
Do you think injecting a larger volume will lead to a more extensive block?
Volume / Dose / Concentration injected
Clearly, it is difficult to change one of these factors without changing another. For example, many studies purporting to show an effect of volume fail to change the concentration of local anaesthetic, with a consequent increase in the dose administered. When the effect of volume (up to 14 ml) is isolated from other factors, most studies suggest there is no significant influence on mean spread although very low volume injections (1.5-2 ml) may reduce mean spread.
Similar basic concerns apply to studies of the effects of different doses: a change in dose will be accompanied by a change in either volume or concentration. Some studies, designed to control for changes in the other factors, have shown that increased dose is associated with increased spread, and others that there is no difference. What really needs to be appreciated is the scale of the effect. If no drug is injected there will be no effect, and a massive overdose (eg accidental intrathecal injection during epidural block) will produce a total spinal, but there is not a straight-line relationship in between. Within the range of doses normally used, a 50% increase in the dose injected will result in an increase of mean spread of only a dermatome or so. Such differences may, on occasion, be statistically significant, but are rarely clinically so, although the increase in duration associated with a larger dose is.
Do you think the temperature of the injectate makes a difference to the spread?
How does temperature affect the density of a solution?
Temperature of the solution
Both CSF and local anesthetics exhibit a curvilinear decrease in density with increasing temperature. Cerebrospinal fluid is at core body temperature whereas local anaesthetic solutions are administered at room temperature. There will be some local decrease in CSF temperature (2–3°C with a 2.7 ml bolus, 6–8°C with a 12 ml bolus) immediately after injection but the core figure is restored within 2 min, so solution density should be reported at body temperature. The consequences of temperature effects are most relevant with plain solutions, 0.5% bupivacaine, for example, being slightly hyperbaric at 24°C (density 1.0032 kg m-3), but slightly hypobaric at 37°C (density 0.9984 kg m-3). Even such minor differences in baricity can cause completely opposite distribution patterns, and may also account for the large variability in the spread of plain bupivacaine when injected at ‘room’ (which may vary considerably) temperature.
Viscosity
This factor has received little attention, but addition of glucose to an aqueous solution affects viscosity as well as density. The more viscous solutions produce significantly greater mean spread than the others. Plain solutions are considerably less viscous than those containing glucose, which may be less miscible with CSF. The injected bolus of hyperbaric solution may thus spread further before mixing fully with CSF, but producing a more ‘even’ distribution as it does so.
Other drugs can be added to the spinal anaesthetic solution to modify the block. What effect do you think this would have on the spread?
Local anaesthetic drug and additives
The extent of intrathecal spread is not altered by which local anaesthetic is used, as long as the other factors are controlled. Solutions containing vasoconstrictors spread in exactly the same way as those without, although block duration may be prolonged. Addition of other drugs, such as opioids or clonidine, has a dual effect. Density is reduced which could make the mixture behave in a more hypobaric manner, but no effect has been shown in clinical practice, suggesting that the changes in density are small. The second effect is seen with opioids, which increase mean spread and delay regression, presumably due to pharmacological enhancement of sub-clinical block. Alkalinisation of the solution does not increase spread, but does prolong duration.
How do you think the patient posture would affect spread?
Clinical Technique
Patient position
The difference between the densities of CSF and the solution injected has a major effect on intrathecal drug spread. This is the result of the action of gravity; hyperbaric solutions ‘sinking’ and hypobaric ones ‘floating’, so the degree of caudad or cephalad spread will depend on the interplay between density and patient position. This interplay is the major determinant of the final extent of block with most techniques.
It is widely believed that injection of a hyperbaric solution in a seated patient will result in a more restricted block. However the block, while initially more restricted, eventually extends to a level equivalent to that which would have been obtained had the patient been placed supine immediately after injection. Production of a classical ‘saddle block’ requires use of relatively small amounts of local anaesthetic in a patient kept in the sitting position for at least 10 minutes. This will restrict the local anaesthetic to the sacral side of the lumbar lordosis when the supine position is resumed. If larger volumes are used, they will still ‘spill over’ into the higher lumbar and thoracic segments spreading higher up.
Given that most plain solutions are marginally hypobaric, some cephalad extension of block might be expected if patients are kept seated after injection. This will result in an adequate block, but has two disadvantages; delay while the block spreads and the risk of serious hypotension due to venous pooling in the legs as the local anaesthetic reaches and blocks the sympathetic outflow.
When using hyperbaric solutions tilt is sometimes used to influence spread, usually in an attempt to limit the cephalad spread and reduce the risk of hypotension. The maintenance of 10° or so of head-up tilt reduces spread, but also has two potentially adverse effects; the block may not spread far enough for the projected surgery and the risk of peripheral pooling of venous blood causing serious hypotension. In fact, every authority on spinal anaesthesia from the time of Labat has recommended the reverse; a small degree of head down tilt to ensure venous return so as to maintain cardiac output and blood pressure. This manoeuvre does not increase the cephalad spread of a hyperbaric solution; due to the curves of the spine, (see later) particularly the posterior thoracic curve in the supine position. Even a 30° tilt has minimal effect on mean spread, although it does increase variability.
An alternative technique for minimizing sympathetic block is to keep the patient in the lateral position after injection so that only one side of the sympathetic chain is affected. As with ‘saddle block’, a small volume of local anaesthetic needs to be used and the position maintained for at least 15 20 minutes for any significant effect. Even then, the block will still tend to spread to the other side once the patient is placed supine for surgery.
Placing the patient in the lithotomy position immediately after the injection of a hyperbaric solution might be expected to limit cephalad spread by abolishing the lumbosacral curve, the ‘slope’ down which the local anaesthetic moves under the influence of gravity. However, this has not been shown to have an effect on spread, perhaps because even the most extreme positioning does not abolish the curve altogether. The cardiovascular effects are less, probably from the beneficial effects of leg elevation on venous return.
In most circumstances, intrathecal local anaesthetic stops spreading about 20-25 minutes after injection. However, marked changes in patient posture, up to 2 hours after injection, can lead to significant changes in extent of the block. The effect is independent of solution baricity, and probably represents bulk movement of CSF still containing significant concentrations of local anaesthetic. All patient movements should be slow and progressive until the block has regressed completely.
Level of injection
Studies with plain solutions of bupivacaine have shown that a higher level of injection results in significantly greater cephalad spread, even when the difference in injection level is only one interspace. Hyperbaric solutions have a more predictable spread, the effect of gravity being the more dominant factor.
Needle type and alignment
Different types of needle bevel impart varying degrees of ‘directionality’ to the flow of drug solution into the CSF. For instance, fluid leaves the Whitacre needle at an angle of 55° to its plane, and this has been used to promote unilateral block. However, there is conflicting evidence regarding the effect of cephalad orientation of the orifice. With plain solutions, cephalad orientation of the Sprotte needle produces a block of faster onset, but to the same mean level, whereas similar alignment of the Whitacre produces greater spread with less variability. The orientation of the orifice does not seem to influence the spread of hyperbaric solutions. Again this may reflect the over-riding effect of density/gravity with these preparations.
Fluid currents
Currents generated within the CSF by fluid injection are an obvious cause of spread. Many factors might affect the formation of these currents, notably the size, shape and orientation of the bevel and the speed of injection. It is widely thought that barbotage, the intentional creation of such currents by the repeated aspiration and re-injection of CSF and local anaesthetic, increases spread, but evidence does not confirm this. Simply varying the speed of injection has been investigated extensively, but with conflicting results. In general, faster injections produce greater spread with plain solutions, but the effect is less marked with hyperbaric ones, with some suggestion that slower injection actually produces greater spread. Glass models of the spinal cord are often used to study such factors, but they omit any representation of the cauda equina and spinal cord, which may act as efficient ‘baffles’ to the generation of fluid currents. Additionally, a fast injection may produce a bulk movement of CSF and pressure changes, which tend to keep the solution near the injection site, whereas a slow injection may allow the solution to spread according to baricity and gravity.
Practical Point: The best injection technique depends upon the desired block. In general, it is best to use a slow injection over at least 15 seconds, without barbotage, of a hyperbaric solution which is more controllable and predictable. I usually have the patient sat up as it is easier to identify landmarks, then lie them down immediately after the injection. Testing the block early (5 mins and 10 mins) can give an idea of how quickly the block is likely to spread. This will often also give an idea of the extent to which it will spread (rapidly spreading block will often reach more segments than a slower spreading block).
Head down or head up tilt can then be used to modify the block to a small degree.
Patient characteristics
Although there is significant variation in maximum spread between patients given a standard technique, spinal anaesthesia is very reproducible in the individual patient. Clearly, the variability must be due to patient factors, but it is far from clear which is the most significant.
Age
At the extremes of age there are small, but significant increases in maximum spread, rate of onset of motor block, and cardiovascular instability regardless of the solution used. It is probable that these are secondary to age related changes in spinal anatomy, nerve physiology and cardiovascular reflexes.
Height
No firm correlation between height and spread has been found – this is probably since most of the difference in height between adults is due to the length of the lower limb long bones, not the spine.
Weight
It is often suggested that epidural fat compresses the dural sac, reduces CSF volume and results in the increased spread observed in obese patients. However, these studies used plain solutions, which are known to produce wider variability in block height, and studies with hyperbaric solutions have failed to show a significant relationship. In addition, it is recognized that the level of injection in obese patients is often higher than intended, and this can result in greater cephalad spread. Finally, when an obese patient is lying in the lateral position, the distribution of adipose tissue may alter the alignment of the vertebral canal. There are no data available which have controlled these variables in an attempt to determine if weight per se has any influence on local anaesthetic spread.
Sex
The spread of hyperbaric solutions may be influenced by differences in body shape while the patient is in the lateral position. Males tend to have broader shoulders than hips so that the spinal column has a ‘head up’ tilt in the lateral position, whereas the reverse is true in females. However, patients are usually turned supine immediately after injection so this effect is likely to be small. Differences in CSF density may be more relevant. This is higher in males, and will reduce the baricity of the local anaesthetic solution, thereby limiting cephalad spread.
Intra-abdominal pressure
It is often said that raised intra-abdominal pressure increases blood flow through the epidural veins, which then distend and compress the theca to decrease CSF volume. However, this theory was not entirely supported by an MRI study which found that increased abdominal pressure decreased CSF volume by displacing tissue into the vertebral canal through the intervertebral foraminae rather than by changing epidural venous volume. A reduction in CSF volume may influence cephalad spread of local anaesthetic, but no study has distinguished this effect from other causes.
Spinal anatomy
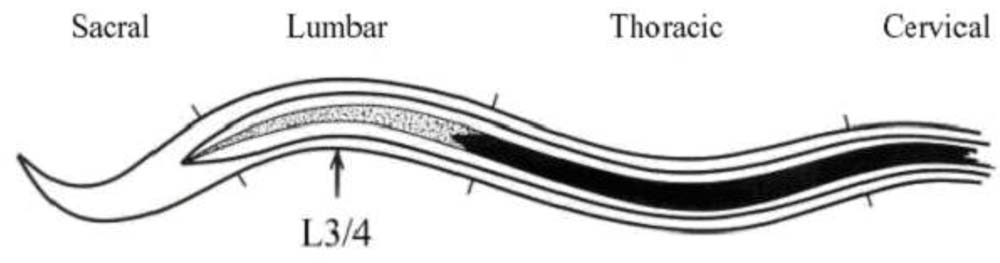
Variations in spinal curvature are only of importance when they influence the gravitational spread of local anaesthetic solutions. Consequently, a scoliosis is unlikely to influence spread unless the patient is kept in the lateral position. A kyphosis, or a change in the normal lumbar lordosis (e.g. in pregnancy), is more likely to have an effect because the antero-posterior curves are crucial to the pattern of spread of a hyperbaric solution in the supine patient. Abnormal spinal curvature can be a cause of block failure, particularly if it moves the ‘highest’ point of the lumbar spine in the supine position from its usual level of L4. The picture shows the curves of the spine in a supine patient.
Lumbosacral CSF volume
Total CSF volume in an average adult is about 150 ml, approximately half of which is intracranial. The remainder lies within the spinal subarachnoid space, and represents the volume through which the injected solution can distribute. While many factors influence CSF volume, and it may have a crucial effect on intrathecal drug spread, detailed study is, unfortunately, inhibited by the difficulties of measuring CSF volume, even with radiological imaging.
Pregnancy
Many physiological changes that occur during pregnancy increase the effect of intrathecal anaesthetic injection. Physical spread of the solution can be increased by changes in the lumbar lordosis, and in the volume and density of the CSF. Cephalad spread may be greater due to a progesterone mediated increase in neuronal sensitivity, The mechanisms which may be involved include direct effects on membrane excitability, indirect actions on neurotransmitters, increased permeability of the neural sheath, potentiation of endogenous opioids, and potentiation of GABA-mediated increases in chloride conductance. These physical and pharmacological factors add up to a considerable increase in the consequences of an intrathecal injection in the full term pregnant patient.
Summary
Many factors affect the intrathecal spread of injected local anaesthetics, however, the influence of most of these is small, unpredictable and outwith the clinician’s control. The major factors are the baricity of the solution injected and the subsequent posture of the patient. The most predictable effects are produced by the slow injection (into a patient placed supine immediately thereafter) of a small volume of local anaesthetic solution containing glucose. Use of glucose concentrations somewhat lower (about 1%) than are traditional (5-8%) will reduce the risk of excessive spread, but still ensure good quality and extent of block for most surgical procedures for which spinal anaesthesia is appropriate. Manipulation of the factors which affect spread may be used to produce different types of block, as long as the clinician has a clear understanding of what is involved.
Further reading
- Hocking G, Wildsmith JAW. Intrathecal drug spread. British Journal of Anaesthesia 2004; 93: 568-78
- For details of practical aspects of spinal anaesthesia, please refer to:
- Ankorn C, Casey WF. Spinal Anaesthesia – a practical guide 2000; 12: 21-34
- Casey WF. Spinal Anaesthesia – a practical guide 1993; 3: 2-15
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/