Regional Anaesthesia
Tutorial 59

Questions
- Name 5 surgical procedures which are suitable for a subarachnoid block?
- What level do the following end:
- spinal cord?
- dural sac?
- What type and size of spinal needle is recommended for a subarachnoid block?
- What is the average distance from the skin to the dura?
- How are Local anaesthetic drugs rendered “Heavy”
INTRODUCTION
- The subarachnoid block (SAB) is popularly known as a spinal block. There can be confusion when the term “spinal anaesthesia” is used as some anaesthetists include subarachnoid block and epidural block under the classification of spinal anaesthesia.
- To avoid this confusion, it is preferable to use the terms subarachnoid block and epidural block exclusively. Hopefully “spinal anaesthesia” will disappear from the anaesthetic lexicon in due course.
- Subarachnoid block is an extremely useful technique. It is a relatively easy block for the novice to learn and it is a satisfying technique for the patient, surgeon and anaesthetist.
- The novice anaesthetist rapidly gains confidence as proficiency is gained. Success rates of 95% plus can be expected.
- SAB provides excellent surgical operating conditions for procedures below the umbilicus.
- It is quite remarkable that an anaesthetist can carry on his person the necessary equipment to provide excellent anaesthesia to half the body. necessary equipment to provide excellent anaesthesia to half the body.
- The simplicity of the block belies the dangers in the technique. Make no mistake – the subarachnoid block can be lethal in the hands of the inexperienced or incompetent anaesthetist.
- A clear knowledge of the relevant anatomy is essential. I suggest the reader consults an anatomical atlas to reacquaint himself with the anatomical features of the lumbar spine. It is also a good idea to study an articulated skeleton or some of the excellent “plastic spines” available.
- Remember: It is easy to learn this technique. It is avoiding (or managing) the complications which may prove difficult.
INDICATIONS
- SAB is suitable for most surgical procedures below the level of the umbilicus (T 10).
- Typical operations include perineal surgery, abdominal gynaecological procedures, prostatectomy, caesarean section and hernia repairs. Most hip and knee joint replacements are performed under SAB.
- Patients may choose to remain awake but light sedation is usually less stressful for all concerned.
- SAB is particularly suitable for elderly patients – especially those suffering from cardiovascular and respiratory disease.
- These patients tend to be less confused post operatively.
- SAB is ideal for patients suffering from renal, hepatic and metabolic disease (eg diabetes).
- It is clearly better for mother and baby in obstetric anaesthesia.
- I believe SAB is a safer and cheaper form of anaesthesia in remote location situations. When the relatively inexperienced anaesthetist is called upon in an emergency to provide anaesthesia, my view is that SAB is a better option than general anaesthesia. This is a controversial issue however.
- SAB is a good choice when called upon to provide emergency anaesthesia for lower limb surgery in the intoxicated patient with a full stomach.
CONTRAINDICATIONS
- These can be divided into absolute and relative contraindications:
- Absolute
- Patient refusal
- Sepsis at site of lumbar puncture
- Coagulopathies or patients on anticoagulants.
- Relative
- Hypovolaemia
- Aortic stenosis
- Septicaemia
- Raised intracranial pressure
- It should be remembered that no surgical or anaesthetic procedure is entirely risk free. Common sense and clinical judgement are important when deciding upon a suitable form of anaesthesia.
- A SAB may be the preferred technique despite being relatively contraindicated (eg emergency lower limb surgery in the hypovolaemic patient with chest trauma).
- It is pertinent to mention that a contraindication would be an inexperienced, poorly equipped anaesthetist.
- It is best to become proficient in the technique of subarachnoid anaesthesia whilst working under the supervision of an experienced anaesthetist.
ANATOMY
- As mentioned previously, the reader should consult an anatomical atlas and study an articulated skeleton or plastic spine to become familiar with lumbar spinal anatomy.
- The spinal cord ends at L2 and the dural sac ends at S2.
- The cord terminates in a spray of nerves (filium terminale).
- The ideal place to insert a spinal needle is between L2 and S2.
- A line drawn between the highest points of the iliac crests (the intercristal line) crosses the L 4 spinous process.
- Always insert the spinal needle at the L3-4 interspace. If you fail to reach the cerebrospinal fluid (CSF), reattempt at the interspace above or below (ie L2-3 or L4-5). The Taylor approach via L5 – S1 is the next choice when the 3 above interspaces have been unsuccessful (see later).
- I try to avoid L 1-2 and above for fear of damaging the spinal cord.
What follows is an imaginary journey from the skin to the subarachnoid space at the L3-4 interspace: [Fig 16]
- The spinal needle enters the skin in the midline between the lumbar spines.
- The subcutaneous adipose tissue is usually 1-2 cm thick (can of course be much thicker).
- Next is the supraspinous ligament – a longitudinal strap which joins the tips of the spines together.
- Next is the interspinous ligament – a narrow fibrous band between the spines.
- Next, at a depth of 3 – 4 cm from the skin is the tough ligamentum flavum which holds the bony laminae together. This 0.5 cm thick structure is an important landmark for the anaesthetist.
- The ligamentum flavum has a hard, gritty texture and grips the spinal needle. This is very distinctive and the anaesthetist rapidly gains a “feel” for this.
- Immediately beyond the ligamentum flavum is the epidural space. This space contains large thin walled epidural veins and adipose tissue.
- The needle is now within millimetres of the dura. Advance the needle and you may get the sensation of the dura being ‘tented’ by the needle tip and a definite “pop” as it perforates.
- Advance the needle another couple of millimetres and withdraw the stylet. You should be rewarded by the appearance in the hub of clear, opalescent CSF.
- The distance from the skin to the dura is 4 – 5 cm on average.
- The subarachnoid space is essentially the contents of the dural sac (ie the spinal cord and nerve roots bathed in CSF).
- At this level, the spinal cord is about the diameter of the patients little finger. The dural sac is about the diameter of the patients index finger.
- Local anaesthetic (3 – 4 ml) deposited here spreads over several segments and “fixes” within a few minutes as it soaks into the cord.\
- The result is a temporary pharmacological trans-section of the spinal cord at this level.
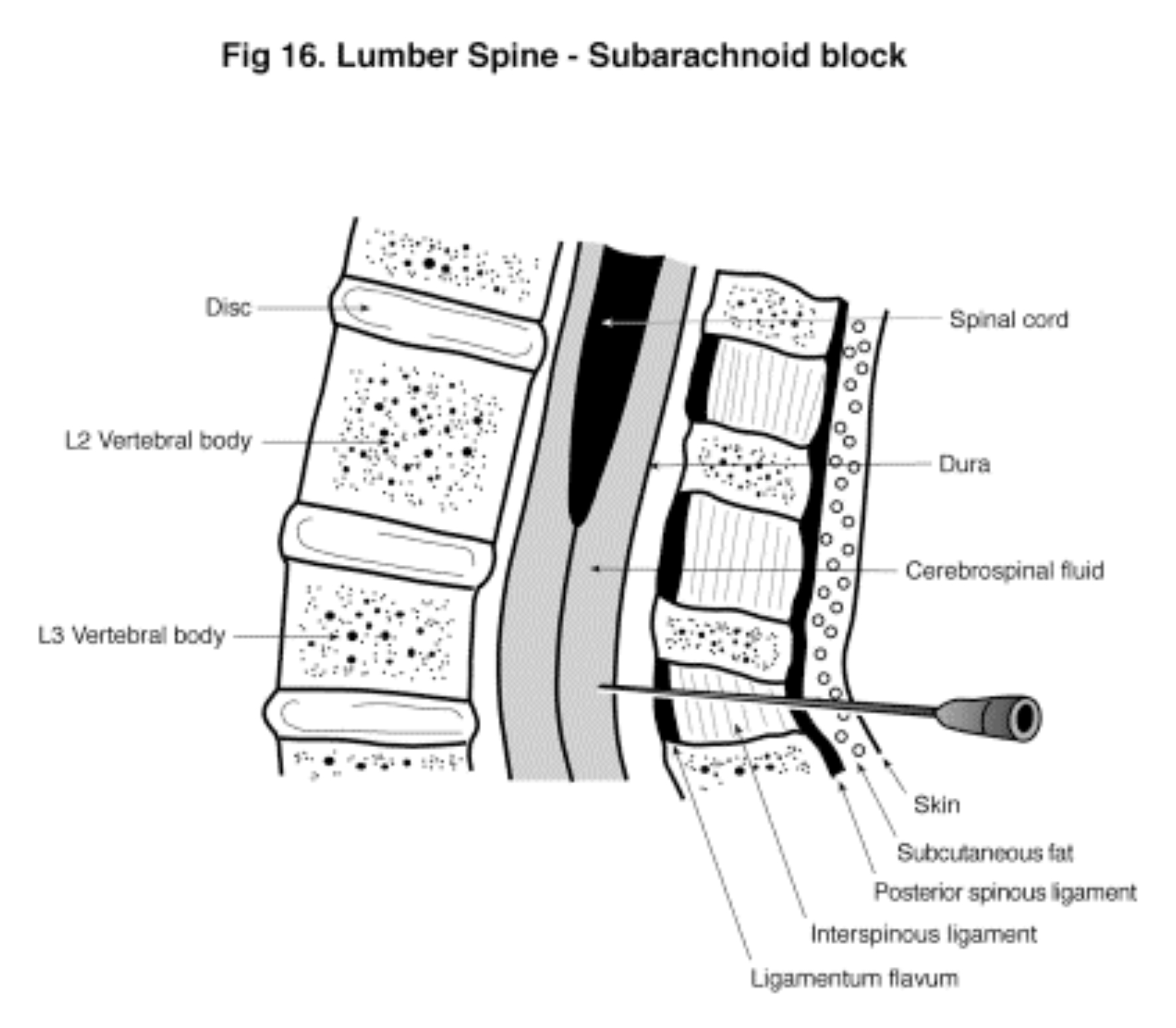
Figure 16 (Click to enlarge)
EQUIPMENT
Spinal needles:
Traditional spinal needles have a stilette and a bevelled tip. They range in size from 20 G – 29G. The standard lengths are 90mm and 100mm.
- The commonly used gauges are 22 G and 25 G.
- I no longer use these needles in my anaesthetic practice as they are associated with a 10 – 15% incidence of post spinal headache.
- There are several designs on the market. I strongly recommend the pencil point needle. This needle has a solid tip (like a pin) and an opening 2 – 3 mm from the tip.
- Pencil point needles push through the dura rather than cutting through. This results in less leakage of CSF and an incidence of spinal headache of less than 1%.
- I routinely use a 26 G pencil point needle but the beginner should use 22 or 23 G traditional needles to learn the technique. The reason for this is that it is easier to “feel” the different tissues with the larger needle.
- Using the 26 G pencil point needle is more technically demanding and the beginner is likely to “pepperpot” the dura with multiple holes. These multiple stabs result in a greater CSF leakage than a single 22G perforation.
- Always use an introducer. A sharp 18 G needle will suffice if an introducer is not packaged with the spinal needle.
Spinal tray:
- 2 ml plastic syringe – for the lidocaine 1% skin infiltration.
- 5 ml plastic syringe – for the bupivacaine 0.5%.
- 26 G pencil point needle (90 mm) + Introducer.
- 18 G blunt drawing up needle.
- 26 G (40 mm) needle for lidocaine infiltration.
- Galley pot + Betadine solution (alcoholic povidone/iodine).
- Sterile drapes.
- Bupivacaine 0.5% plain (or heavy) in 4 ml sterile ampoule.
- Small pack of gauze squares.
- Sterile gloves.
Other equipment:
- 16 or 18 G intravenous cannula + intravenous fluid infusion.
- Monitors (Pulse oximetry, ECG, BP).
- Oxygen via mask or nasal prongs.
TECHNIQUE
- Monitors are connected and oxygen administered.
- Insert an 18 G intravenous cannula and commence an intravenous infusion of normal saline or lactated ringers. Start the infusion so that 500 – 1000 ml has been infused by the time the spinal injection has been completed. This compensates for the expected peripheral vasodilation.
- Administer an anxiolytic dose of iv midazolam. Be careful not to over sedate the patient as it is useful to have their cooperation when positioning.
- Correct positioning is all important in performing a successful spinal block. A knowledgeable assistant who understands how to position the patient is invaluable.
- There are two positions – sitting and lateral.
- I seldom employ the sitting position as patients can suffer vasovagal episodes (usually at the most inopportune time).
- The sitting position is useful in the morbidly obese or the pregnant patient as it is easier for the patients to maintain flexion and easier for the anaesthetist to stay in the midline.
- The sitting position is ideal for a saddle block. A small volume of “heavy” bupivacaine is injected and the patient is kept sitting for 5 minutes to allow the LA to sink down and block the sacral roots.
- A word of warning: Don’t give sitting patients iv midazolam. The prospect of a morbidly obese patient in a semi-comatosed state slumping forward onto the assistant doesn’t bear thinking about.
- I recommend using the left lateral position wherever possible. Ask the patient to “curl up in a foetal position” or “arch your back like a cat” or “push your back out towards me”.
- The assistant embraces the patient with one arm behind the neck ant the other behind the knees. Good flexion is paramount. The back should be vertical – a pillow between the knees may facilitate this.
- Elevate the operating table so that, when seated, your eye is on the same level as the spinal needle insertion site. This helps you to stay in the midline.
- Paint the skin with alcoholic povidone/iodine and drape the patient.
- Identify the intercristal line (L4) and infiltrate lidocaine 1% using the 25 G long needle. Warn the patient you are about to do this as they will instinctively pull away and it may be difficult to coax them into fully flexing again.
- I infiltrate to a depth of 2 –3 cm but the subcutaneous tissues are not particularly sensitive. What is sensitive however are the periosteum and nerves. Keep away from both.
- Place your index and middle finger on either side of the spinous process at the L 3 – 4 interspace.
- Insert the introducer in a slightly cephalad direction and pass the 26 G pencil point needle through it.
- The key to success is staying in the midline. This can prove difficult in obese patients as the spines may not be palpable.
- If the needle strays from the midline it can pierce a nerve root causing the patient to complain of pain – usually in the leg. Take note of which leg as this will guide the redirection of the needle.
- At a variable depth of 3 – 7 cm (average 4 cm) a definite “gripping” resistance will be felt – not unlike trying to push a needle through a rubber eraser. This is the ligamentum flavum.
- Advance the needle a few more millimetres and you should feel a “pop” as you perforate the dura. Continue for 2-3 mm and withdraw the stilette. CSF should appear at the hub.
- Slowly inject 2 – 4 ml of LA.
- If bone is struck, reinsert the introducer and needle in a more cephalad direction.
- If a nerve root is struck, you have deviated from the midline.
- If blood appears in the hub, you have probably pierced an epidural vein. If the CSF is blood stained but the blood clears, it is safe to inject.
- If you are unable to reach the subarachnoid space despite optimum flexion, make another attempt at an adjacent interspace. Some anaesthetists try a lateral approach (the point of entry is 1 – 2 cm lateral to the spines and the needle is angled appropriately). I don’t find it particularly useful.
- The Taylor approach is a godsend in these situations. It is a surprisingly easy approach via the L5 – S1 interspace. Identify the posterior superior iliac spine and introduce a 22 G long spinal needle at a point 1 cm medial and 1 cm caudal to this landmark.
- Aim the needle cephalad and medially to hit the L5 – S1 interspace. You may have to walk the tip along the sacrum to reach the subarachnoid space.
- It is a long way in and you should increase the volume of injected LA by 25%.
- With the 26 G needle it is common to get a passive flow of CSF but be unable to aspirate it. Try rotating the needle 90° and pushing it in another couple of millimetres. If you still can’t aspirate (but can obtain a passive flow of CSF) go ahead and inject the LA. I don’t understand what causes this but suspect it is a membranous tissue acting like a flap valve when negative pressure is applied.
- Roll the patient supine and assiduously monitor the cardiovascular and respiratory parameters.
DRUGS
- I use two local anaesthetic agents in subarachnoid blocks – bupivacaine and lidocaine. Ropivacaine is not currently licensed for subarachnoid use.
- Other LA’s are popular in North America and Europe (eg Cinchocaine, Tetracaine and Mepivacaine).
- I will describe bupivacaine and lidocaine usage only. If the reader wishes to use the other LA’s, he should consult an appropriate anaesthetic textbook.
- Lidocaine is an excellent choice for a short duration SAB (ie 1 – 2 hours). I have used it for many years without a problem but unfortunately there is now a question mark over its suitability for subarachnoid blockade.
- Occasionally a patient complained of transient radicular irritation (TRI) following a lidocaine SAB. Symptoms included back discomfort radiating into the buttocks and legs. These symptoms typically commenced a day after surgery and lasted 3 – 4 days. Patients made a full recovery.
- Although TRI is uncommon and probably harmless, the formal recommendation is to avoid using lidocaine in SAB.
- I have continued to use plain 2% lidocaine in selected cases and will describe its use in this manual. The reader may decide to avoid it altogether and only use bupivacaine.
- Plain bupivacaine and lidocaine are slightly hypobaric (ie less dense) compared to cerebrospinal fluid. If these drugs are administered in the sitting position, they will slowly rise cephalad if the patient remains sitting.
- This risks a high block. These LA’s are highly lipophilic and rapidly soak into the spinal cord (ie they become “fixed”), but the worry is they may rise too high before doing so.
- Likewise, when these drugs are administered in the lateral position they will float up and block the upper leg. Thus the upper leg has a denser block which lasts longer than in the dependent leg.
- These LA’s can be rendered “heavy” with respect to CSF by adding glucose. Heavy lidocaine 5% is no longer manufactured (or used) due to a high risk of neurotoxicity.
- Heavy Bupivacaine 0.5% (contains 6 – 8% glucose) is commercially available in 4 ml sterile ampoules. When administered in the sitting position it will sink to the sacral roots and give a saddle block. In the lateral position it gives a dense prolonged block to the dependent leg.
- If 3 ml of heavy 0.5% bupivacaine is administered at L 3-4 in the lateral position and the patient immediately turned supine, the heavy solution rapidly runs “downhill” to pool in the thoracic kyphosis. Fortunately the bottom of the “hill” is T4 and thus the block seldom rises above this segmental level.
- This can be thwarted by placing the patient in a head down position. If a large volume of drug is used and the patient is steeply head down, a total spinal may result.
- I routinely use 3 ml of heavy bupivacaine 0.5% (or 4 ml of plain bupivacaine 0.5%) administered in the lateral position at L 3-4. The dose depends on individual patient factors such as height and build. You will not go far wrong if you stick to these doses.
- The exception is caesarean section where 2 ml of heavy bupivacaine 0.5% may give a block to T4.
- Plain bupivacaine gives a more dense block and lasts longer than heavy bupivacaine. The reason is because plain, being essentially isobaric doesn’t move far in the CSF before fixing in the spinal cord. Heavy bupivacaine runs quite a distance downhill before fixing and therefore the spinal cord is more extensively coated with LA. This results in a higher, less dense block which is shorter acting.
- For very short procedures (eg knee arthroscopy) I use lidocaine 2% plain administered at L3-4. This gives a block to T10 and 45 – 60 minutes of surgical anaesthesia. Be very careful not to allow the patient to sit up as the lidocaine can rise cephalad.
- Epinephrine prolongs the block by decreasing the rate of LA reabsorption. I don’t find any advantage in using it.
- Clonidine also prolongs the block and is said to have a post block analgesic effect. I don’t find any advantage in using it.
- Morphine (0.15 – 0.25 mg) binds to the spinal cord opioid receptors and greatly improves post operative analgesia. Its effect lasts for 24 hours. I find it especially valuable in managing the post operative pain of total knee replacement.
- Morphine is associated with urinary retention, pruritus and nausea. There is a rare but serious risk of delayed respiratory depression – particularly in the elderly.
- I frequently use subarachnoid morphine and manage the side effects.
- Fentanyl (25 mcg) can be used in the same manner. It is shorter acting (a few hours) and the risk of respiratory depression is negligible.
RECOMMENDED DOSES FOR TYPICAL OPERATIONS:
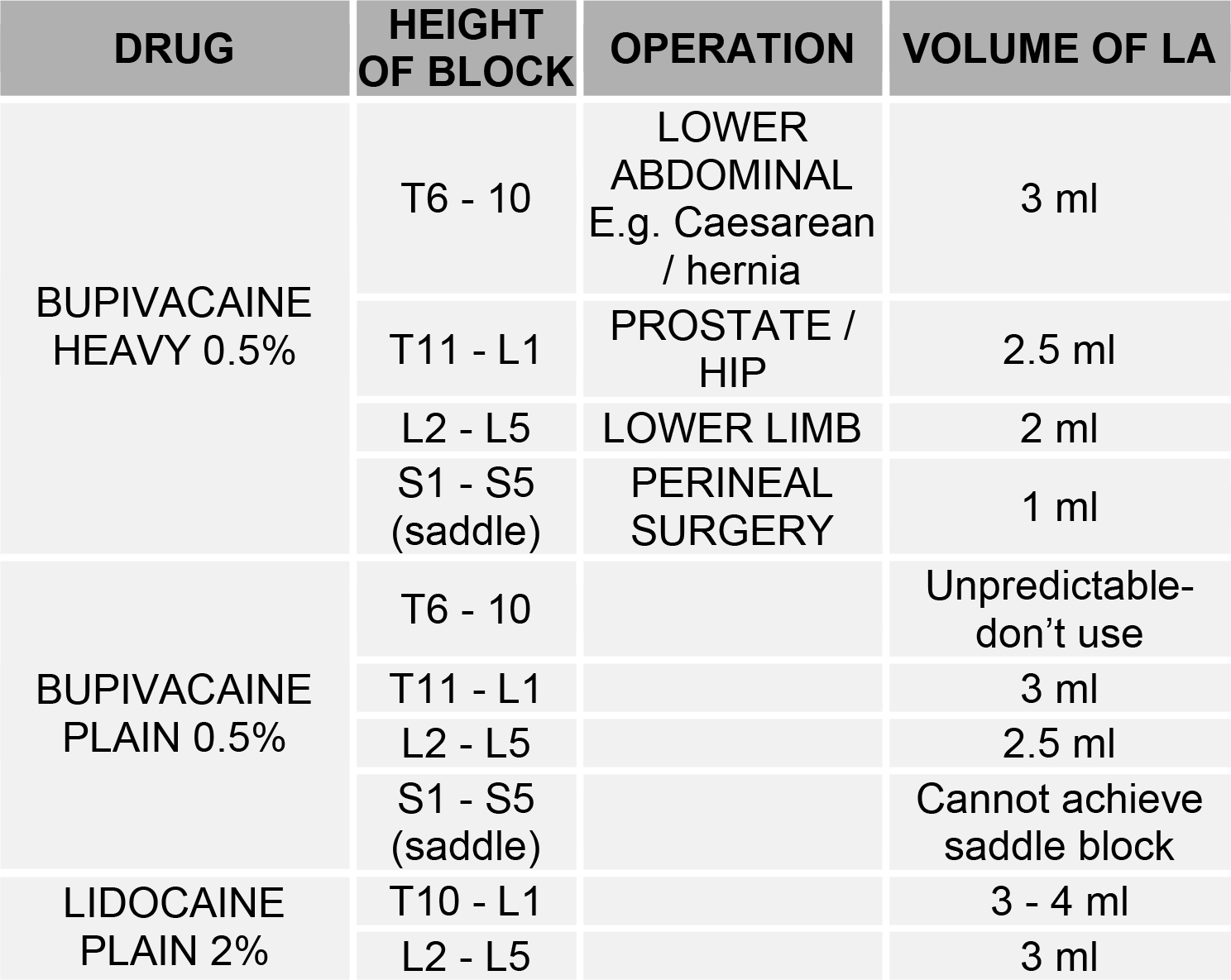
THESE DOSE RECOMMENDATIONS ARE FOR THE “AVERAGE” PATIENT AND SHOULD BE TAILORED TO SUIT THE INDIVIDUAL
MEASURING THE HEIGHT OF A BLOCK
- Always check the height of the block before allowing the surgeon to start.
- Place the subarachnoid block and roll the patient supine. Ask him to lift his leg off the bed. If the quadriceps is weak, we can assume he will eventually get a good block to L2.
- Take an alcohol swab or block of ice (not a needle prick) and touch the ice on the back of the patients hand to give him an idea of the cold sensation you are trying to elicit. Then start at the feet and move proximally until the patient says it feels cold.
- Consult a dermatome diagram to determine the upper level of the block. [Fig 34]
- A quick method is as follows:
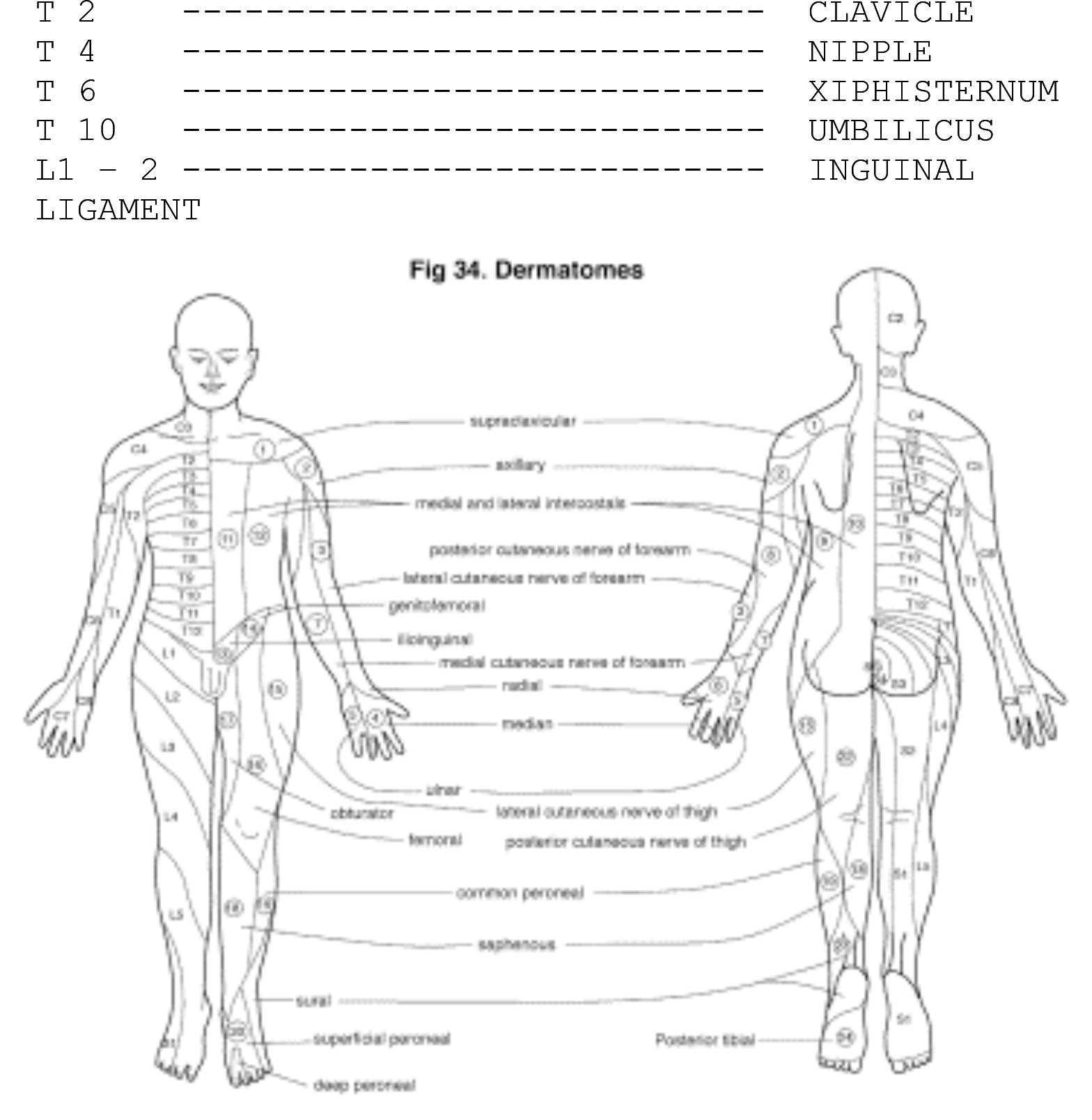
Figure 34 (Click to enlarge)
PROBLEMS…. and how to manage them
Hypotension and Bradycardia:
- The sympathetic vasopressor nerves are thin and unmyelinated. The LA soaks into them easily and they are rapidly blocked. Vasodilation induced hypotension occurs within minutes of performing a SAB.
- The hypotension is accentuated if the patient is hypovolaemic, dehydrated or on antihypertensive medication.
- If the spinal rises high enough it may block the cardiac sympathetic efferents (T1-4). This results in bradycardia due to the unopposed action of the cardiac vagus.
- Bradycardia: administer Atropine6 – 1.2 mg intravenously.
- Hypotension: administer 500-1000 ml of crystalloid rapidly and give Ephedrine 5 – 10 mg – this may be repeated at 5 minute intervals. If unresponsive, draw up 10 mg of Phenylephrine and dilute it in 20 ml of saline (ie 0.5 mg / ml). Give 1 ml doses – usually lasts 5 – 15 minutes.
- Ephedrine causes a mild tachycardia but its main action is vasoconstriction. It can be used in pregnancy as it does not vasoconstrict the placenta. Ephedrine 30 – 60 mg im will act for an hour or more.
- Phenylephrine should not be used in pregnancy as it causes placental vasoconstriction.
High or total spinal:
- The height of the block should not extend above T4 unless:
- A very large dose of LA has been administered
- The patient has been positioned head down after hyperbaric LA.
- The early warning signals of a high block are nausea and yawning. The patient becomes distressed and finds breathing difficult due to block of the intercostal muscles.
- Fortunately the diaphragm is supplied by the phrenic nerve (C3, 4, 5)— “three, four, five keeps the diaphragm alive”. If the block rises to the cervical level the patient can’t breathe or talk.
- THIS IS A REAL EMERGENCY. Support ventilation with a bag and mask. Intubation will probably be required for a few hours. Treat hypotension and bradycardia with vasopressors, intravenous fluids and atropine.
- Ideally a sleep dose of midazolam should be given as soon as possible as this is a terrifying ordeal for the patient.
Spinal headache:
- The incidence of spinal headaches is directly related to the diameter of the spinal needle.
- Traditional 20 –23 G spinal needles had a post puncture headache incidence of 15 – 20%.
- Modern 26 G pencil point needles have an incidence of < 1%.
- The headache is due to loss of CSF through the puncture hole.
- It presents on the first day post spinal.
- The headache is worse when the patient is upright and abates when lying flat.
- It is typically occipito-frontal and may be associated with photophobia and neck stiffness. It is extremely important to exclude meningitis.
- Treatment is bed rest, hydration and oral analgesia. If this fails an epidural blood patch may be administered to seal the hole ( an epidural needle is inserted and 20 ml of the patients own blood is taken and injected into the epidural space. This clots and seals the hole).
Urinary retention:
- Block of the bladder autonomic nerves prevents micturition. The bladder distends and it becomes progressively more difficult to void. A common occurrence in elderly men with prostate problems.
- Also caused by subarachnoid opioids.
- Exacerbated by overly generous iv fluid loading.
- Treatment is urinary catheterisation.
Neurological damage:
- This is very rare if proper technique and procedures are followed.
- The cord and nerve roots may be traumatised by the spinal needle.
- Epidural haematomas can compress the spinal cord and this has been known to result in paraplegia. NEVER perform a SAB on a patient with a serious coagulopathy or who is taking anticoagulants.
- Infection (meningitis / abscess) should be non-existent with proper sterile technique.
SUBARACHNOID BLOCK IN OBSTETRICS
- In obstetric practice, subarachnoid and epidural anaesthesia is usually superior to general anaesthesia (GA).
- SAB is invariably better than GA for mother and baby during labour and delivery.
- The risks of GA are avoided and there are psychological advantages for the mother and babe if minimal sedation is employed.
- Epidural catheters are often inserted during labour for analgesia during the first and second stage. If operative intervention is required (eg caesarean section or forceps) it is simply a matter of topping up or extending the epidural block.
- For a number of years I have done elective caesarean sections and elective forceps extractions under SAB.
- SAB is easier and quicker. The block is denser and more reliable. Bupivacaine SAB allows ample time for the operative procedure.
- Caesarean section technique:
- Insert wide bore iv cannula and infuse a preload of 1000 – 1500 ml of crystalloid.
- Full monitoring (Pulse oximeter, ECG, BP).
- Oxygen via facemask – 4 litres / minute.
- Routine antacid prophylaxis
- Be fully prepared to convert to a GA.
- SAB can be performed sitting or in the lateral position. I prefer the left lateral position. Enter at L3 – 4 with a 26 G pencil point needle.
- I use 2.5 ml of heavy bupivacaine 0.5%. You may add morphine 0.15 – 0.25 mg as it gives good analgesia for 24 hours. (I have ceased this practice as a significant number of the mothers became nauseated).
- Turn mother to supine position with a wedge under right buttock to avoid supine hypotension syndrome.
- Watch the blood pressure and heart rate like a hawk. Both can fall precipitously rather suddenly. Have atropine and ephedrine drawn up and ready to give. Ephedrine does not affect placental perfusion. Avoid phenylephrine as it causes placental vasoconstriction.
- Measure the height of the block. Ideally it should be at T4 – 6. It is not uncommon to find that the block is higher and the patients complains of dyspnoea and numbness of the little fingers (C8). Reassurance is necessary as the block recedes to a lower level within 30 minutes.
- Give Syntocinon at delivery.
- It is important to remember that pregnant patients require less LA for subarachnoid blockade.
- Retained placentae and perineal lacerations:
- I use Heavy bupivacaine 0.5% 1.0 – 1.5 ml in the sitting position.
- Lie the mother supine after 10 minutes and proceed with the surgery.
SUBARACHNOID BLOCK FOR INFANTS
- I try to avoid SAB in paediatric patients. The exception is the high risk neonate / infant. The anaesthetist may be presented with a premature baby with respiratory compromise requiring emergency herniotomy.
- This is a difficult anaesthetic, even in expert hands and a SAB is much safer in these situations.
- An assistant should flex the infant (either lateral or sitting) and the SAB is inserted at L5-S1. Infiltrate the skin with a small amount of 0.5% lidocaine first.
- Use a spinal needle (21 G- 50 mm). These are commonly used for diagnostic lumbar puncture in neonates.
- Use Heavy bupivacaine 0.5%. 0.13 ml / kg. This is a tiny volume (ie 0.39 ml in a 3 kg neonate) and it includes an extra volume to account for the needle dead space (don’t barbotage).
- The block comes on rapidly (the surgeon can start within a minute) but lasts less than an hour.
- The blood pressure and respiratory parameters remain surprisingly stable.
SUBARACHNOID BLOCK FOR HIP FRACTURES IN THE ELDERLY
- The following subarachnoid technique is an excellent way to manage frail, elderly patients presenting for hip fracture surgery.
- Cardiovascular stability is maintained due to a very reliable localised block.
TECHNIQUE:
- Intravenous fluids, oxygen and full monitoring.
- Positioning the patient into the lateral position can be painful. Give ketamine 20 – 30 mg slowly (over 1 minute to avoid apnoea). This is an “analgesic” dose of ketamine and will last 20 minutes. Always give a small dose of midazolam (1 – 2 mg) to cover possible hallucinations.
- Lateral position with fractured hip uppermost.
- Local anaesthetic solution: Take a 5 ml syringe and add 2 ml of bupivacaine plain 0.5%. Add 50 mcg of fentanyl. Make up to 5 ml with normal saline.
- (This gives a solution of Bupivacaine 2 mg / ml and fentanyl 10 mcg / ml).
- Lumbar puncture at L 3-4 and inject 2.5 ml of the above solution. Leave in lateral position for 5 minutes and then position for surgery.
- This solution is mildly hypobaric so it floats up and blocks the affected hip without causing major cardiovascular instability.
DAY SURGERY SUBARACHNOID BLOCKS
- Lidocaine has been ideal for short acting (ie 1-2 hours) subarachnoid blocks in day surgery.
- With the recent concerns about transient radicular irritation with subarachnoid lidocaine, a reasonable alternative is low dose bupivacaine + fentanyl.
- I have found the following doses suitable for lower limb surgery: Bupivacaine 7.5 mg + fentanyl 25 mcg – prepare this mixture by taking 1.5 ml of bupivacaine 0.5% and add 25 mcg of fentanyl. Add saline to make up a final volume of 4 ml.
- Perform this injection at L3-4 in the lateral position with the operative limb uppermost. Leave the patient in this position for a few minutes (the solution is slightly hypobaric and will float up and give a denser block on the operative side).
- Roll the patient supine. This should give a good sensory block to L2 lasting 90 minutes.
- Patients should be able to walk freely at 2 – 3 hours post injection.
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/