Basic Sciences

SELF ASSESSMENT
Multiple choice questions – state true or false:
- Regarding the use of propofol in total intravenous anaesthesia:
- Target controlled infusion pumps calculate their infusion rates according to patient factors like age and weight.
- Target controlled infusion pumps measure the plasma concentration of the drug.
- Total intravenous anaesthesia can be administered safely with use of syringe driver pumps.
- Target controlled infusion pumps use a bolus elimination transfer technique to administer drugs.
- The patient’s cardiac output alters the actual plasma concentration of drugs while using target controlled infusion pumps.
- Remifentanil – when used in target controlled infusion:
- Is ideal for use in prolonged infusion due to its short elimination half life.
- Does not offer postoperative analgesia.
- Shows synergism when used in combination with propofol.
- Its pharmacokinetics is not altered by patient age.
- Can be safely used as a sole anaesthetic agent for short surgical procedures.
- Pharmacokinetics of propofol.
- Propofol follows a three compartment model after a bolus dose.
- There is a lag between the plasma concentration and effect site concentration of propofol when used in continuous infusions.
- Target controlled infusion pumps can predict the time for patient to wake up after stopping the infusion.
- Loading dose is calculated using the desired plasma concentration and peripheral volume of distribution.
- Steady state of propofol concentration can be achieved without using a bolus dose in anaesthetic practice.
Questions:
- Define volume of distribution and clearance and describe how these could affect the pharmacokinetics of intravenous anaesthetic agents.
- Briefly outline the relationship between plasma concentration and effect site concentration of propofol.
- Describe problems associated with target controlled infusion pumps in anaesthetic practice.
- Outline how the pharmacokinetics of remifentanil is suitable for use in prolonged infusions.
- How does the target controlled infusion pump meant for total intravenous anaesthesia differ from an ordinary infusion pump?
History and evolution of intravenous anaesthesia
Intravenous administration of drugs dates back to the seventeenth century when Christopher Wren injected opium into a dog using a goose quill and pig bladder and the dog becomes ‘stupefied’. In the 1930s hexobarbital and pentothal were introduced into clinical practice.
It was in the 1960s Pharmacokinetic that models and equations for IV infusions were formed and in the 1980s, computer controlled IV infusion systems were introduced. In 1996 the first target controlled infusion system (the ‘Diprufusor’) was introduced.
Definition
A target controlled infusion is an infusion controlled in such manner as to attempt to achieve a user defined drug concentration in a body compartment of interest or tissue of interest. This concept was first suggested by Kruger Thiemer in 1968.
Pharmacokinetics
Volume of distribution.
This is the apparent volume in which the drug is distributed. It is calculated by the formula: Vd = dose/concentration of drug. Its value depends on whether it is calculated at time zero – after a bolus (Vc) or at steady state after an infusion (Vss).
Clearance.
Clearance represents the volume of plasma (Vp) from which the drug is eliminated per unit time to account for its elimination from the body. Clearance = Elimination X Vp.
As clearance increases the half-life reduces, and as the volume of distribution increases so does the half-life. Clearance can also be used to describe how quickly the drug moves between compartments. The drug is initially distributed into the central compartment before distribution to peripheral compartments. If the initial volume of distribution (Vc) and the desired concentration for therapeutic effect (Cp) are known, it is possible to calculate the loading dose to achieve that concentration:
Loading dose = Cp x Vc
It can also be used to calculate the bolus dose required to rapidly increase the concentration during a continuous infusion: Bolus dose = (Cnew – Cactual) X Vc. The rate of infusion to maintain steady state = Cp X Clearance.
Simple infusion regimens do not achieve a steady state plasma concentration until at least five multiples of the elimination half life. The desired concentration can be achieved more quickly if a bolus dose is followed by an infusion rate.
Pharmacokinetics of target controlled infusions
Pharmacokinetic models attempt to describe the relationship between dose and plasma concentration with respect to time. A pharmacokinetic model is a mathematical model that can be used to predict the blood concentration profile of a drug after a bolus dose or after an infusion of varying duration. These models are typically derived form measuring arterial or venous plasma concentrations after a bolus or infusion in a group of volunteers, using standardised statistical approaches and computer software models.
Mathematical models generate some pharmacokinetic parameters such as volume of distribution and clearance. These can be used to calculate the loading dose and rate of infusion necessary to maintain a steady-state plasma concentration at equilibrium.
Since it has been recognised that pharmacokinetics of most anaesthetic agents conform best to a three compartmental model, numerous algorithms for targeting blood and effect site concentrations have been published and several automated systems have been developed.
In 1968, Kruger-Theimer illustrated how pharmacokinetic models can be used to design efficient dose regimens. This Bolus, Elimination, Transfer (BET) regimen consists of:
- a bolus dose calculated to fill the central (blood) compartment,
- a constant-rate infusion equal to the elimination rate,
- an infusion that compensates for transfer to the peripheral tissues: [exponentially decreasing rate]
Traditional practice involved calculating the infusion regimen for propofol by the Roberts method. A 1.5 mg/kg loading dose is followed by an infusion of 10 mg/kg/hour that is reduced to rates of 8 and 6 mg/kg/hr at ten minute intervals.
Effect site targeting
The principal effects of anaesthetic intravenous agents are the sedative and hypnotic effects and the site at which the drug exerts these effects, termed the effect site is the brain. Unfortunately it is not feasible in clinical practice to measure brain concentration [effect site]. Even if we could measure direct brain concentration, it would be necessary to know the exact regional concentrations or even receptor concentrations where the drug exerts its effect.
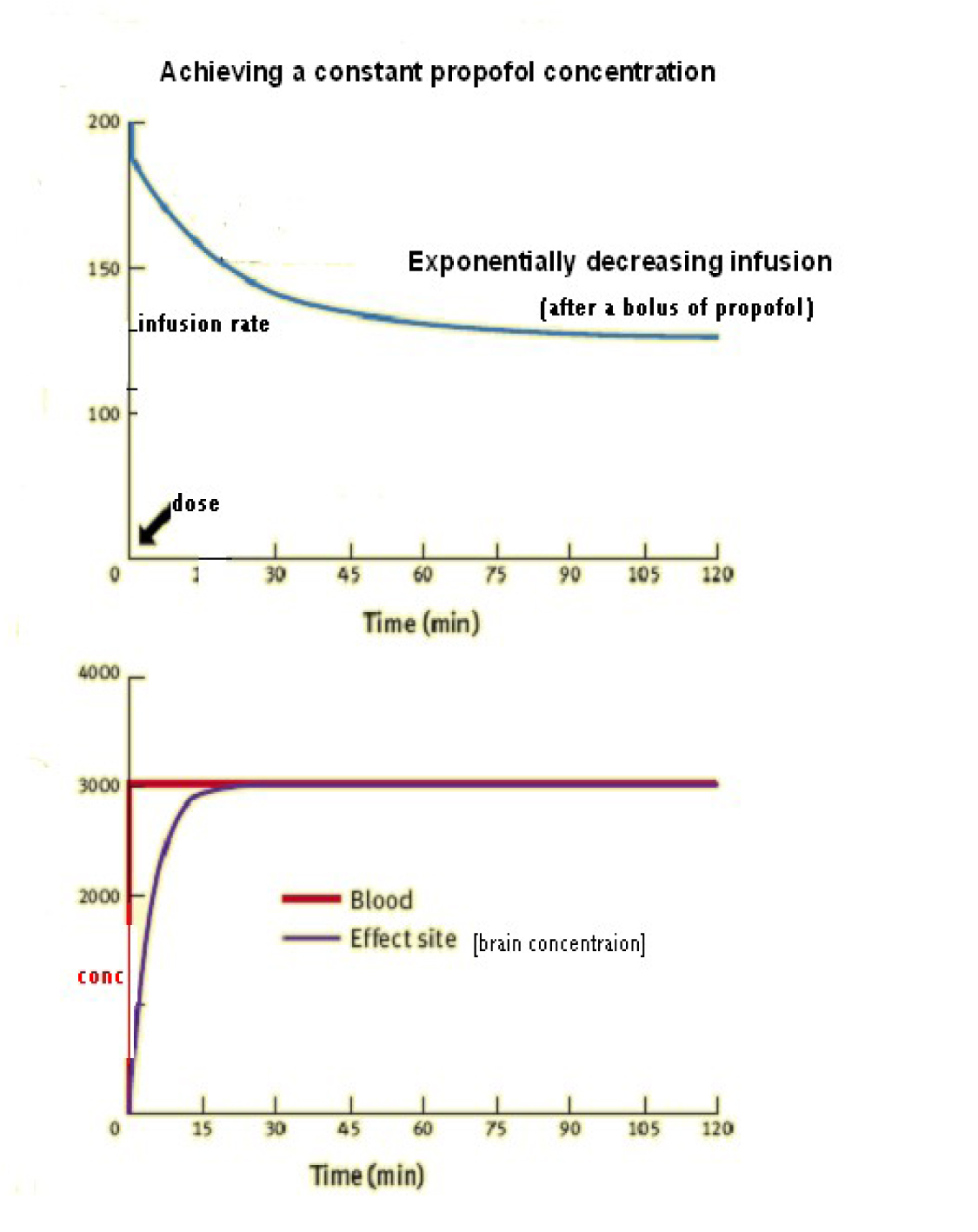
Achieving a constant propofol concentration
The diagram below illustrates the infusion rate required at an exponentially decreasing rate after a bolus dose in order to maintain a steady state blood concentration of propofol. It also shows the lag between the blood and effect site concentration.
Computer controlled pharmacokinetic models
Using a pharmacokinetic model, a computer continuously calculates the patient’s expected drug concentration and administers a BET regimen, adjusting pump infusion rates, typically at 10-second intervals. Models are derived from previously performed population pharmacokinetic studies. By programming desired target concentrations, the anaesthetist uses the device in a fashion analogous to a vaporizer. There are differences between predicted and actual concentrations, but these are not of great consequence, provided the true concentrations are within the drug’s therapeutic window.
Patient pharmacokinetics and pharmacodynamics vary with age, cardiac output, coexisting disease, concurrent drug administration, body temperature and weight of patient. These factors play an important role in choosing target concentrations.
Vaughan Tucker developed the first computer assisted total IV anaesthetic system [CATIA]. The first commercial target-controlled infusion device was the Diprufusor introduced by Astra Zeneca, dedicated to propofol administration in the presence of a pre-filled propofol syringe with a magnetic strip at its flange. Many new systems are available for use now. Patient data like weight, age and height are programmed in the pump and the pump software, by using pharmacokinetic simulation, apart from administering and maintaining appropriate infusion rates, displays the concentrations calculated and the expected time to recovery.
The TCI pumps have three superimposed infusions, one infusion at a constant rate to replace drug elimination and two exponentially decreasing infusions to match drug removed from central compartment to other peripheral compartments of distribution.
Key components of a TCI infusion system
- User interface to enter patient details and target blood concentration.
- Software with pharmacokinetic model-validated for specific drug to control infusion rate.
- Communication between ‘control unit’ and pump hardware
Common TCI models available
- Marsh model used by Diprufusor for propofol
- Schüttler and White-Kenny (WK) models for propofol
- Schnider model for propofol
- Kataria and Paedfusor model in children
- Minto model for remifentanil
Commonly available pumps include: Fresenius vial master TCI [diprufusor], Alaris IVAC TCI, Terumo TE372 TCI (Diprufusor), Alaris Asena PK and Fresenius Base Primea.
Propofol TCI models
The pharmacokinetic model most anaesthetists may be familiar with is the Marsh model published by Marsh et al. Several other models are available now.
Marsh model:
This model uses the diprufusor software used by the diprufusor introduced by Astra Zenca. This model requires age to be programmed in the pump, but does not incorporate it into its calculation [however does not function if age < 16 is entered]. The diprufusor model is used by the Graesby 3500 TCI pump, vial medical TCI pump and the Alaris IVAC TIVA TCI pump.
Schnider model:
This is a more recent pharmacokinetic model for propofol. This model is used in the Alaris Asena TCI pumps. It requires age, height, and total body weight to be input for programming. The pump calculates the lean body mass for that patient and calculates doses and infusion rates accordingly. It would be more suitable in the elderly who have a lower lean body mass and would require lesser doses of propofol for induction and maintenance of a constant plasma concentration.
At present there is no method of measuring drug concentrations real time analogous to the end tidal volatile agent concentration, which gives reassurance the drug is reaching the target organs. In 1992 a set of standardised criteria were published for assessing the predictive performance of computer controlled infusion systems.
When a drug is administered as a target controlled infusion, the choice of which figure to use for the body weight is critical. The pump uses the model that makes assumptions about clearance rates and volumes of distribution that will have a significant impact on ongoing infusion rates and total dose administered. Older models like the Marsh model which used the total body weight can significantly overdose patients if actual body weights are used in obese patients. Anaesthetists in these situations while administering drugs usually look for the ideal body weight based on the patients height. More recent models such as those published by Schnider and colleagues for propofol and Minto and colleagues for remifentanil use age and lean body mass in their calculations. These models require the user to enter the total body weight, height and gender and then use the variables to calculate the lean body mass according to the following formulae:
Males:
- LBM = 1.1 X weight – 128 X {weight/height}²
Females:
- LBM = 1.07 X weight – 148 X {weight/height}²
One major difference between the Marsh model and the Schnider model is the size of the central compartment. For a 70 kg patient the Marsh model calculates the central compartment volume as 15.9 L whereas the corresponding value for Schnider model is 4.27 L. Because of this the estimated concentrations following a bolus or rapid infusions vary greatly. When propofol administration is stopped, large differences in the estimated concentrations are again found, with the Schnider model estimating a much more rapid fall in concentration than the Marsh model.
Remifentanil TCI models:
Remifentanil is an ultra short acting opioid which has unique properties allowing prolonged infusions without drug accumulation. The commonly used pharmacokinetic model for remifentanil is the Minto model which is a three compartmental pharmacokinetic model specific for remifentanil. This model was produced from a study of pharmacokinetics of remifentanil in a heterogeneous population. As with propofol infusions, if blood targeting is used and rapid onset of anaesthesia is required, then the blood concentration should be set to a level higher than the likely therapeutic effect site concentration. After induction target concentrations are adjusted according to the level of surgical stimulus and clinical responses.
Pharmacodynamics with use of TCI pumps
In an un-premedicated patient, plasma concentration of propofol required to produce loss of consciousness is about 5 to 6 mcg/ml. This may vary up to 8 mcg/ml in young fit un-premedicated adults. In premedicated patients it is 4-5 mcg/ml. Volunteers waking from anaesthesia have a blood concentration of around 1- 2 mcg/ml.
Adequate analgesia with remifentanil is achieved with 3- 8ng/ml and may require concentrations up to 15 ng/ml for stimulating procedures. A remifentanil infusion of 0.25-0.5 mcg/kg/min in 70kg, 170cm, 40 yr old man produces a blood concentration of around 6ng/ml after 25 minutes.
Interaction does occur with propofol and remifentanil when used in combination during TIVA. Propofol and remifentanil tend to show synergism. Propofol and remifentanil together cause a 41% decrease in apparent volume of distribution. It can be seen from the diagram below the effect site concentration lags behind the plasma concentration and the effect site concentration [brain concentration] cannot readily be measured.
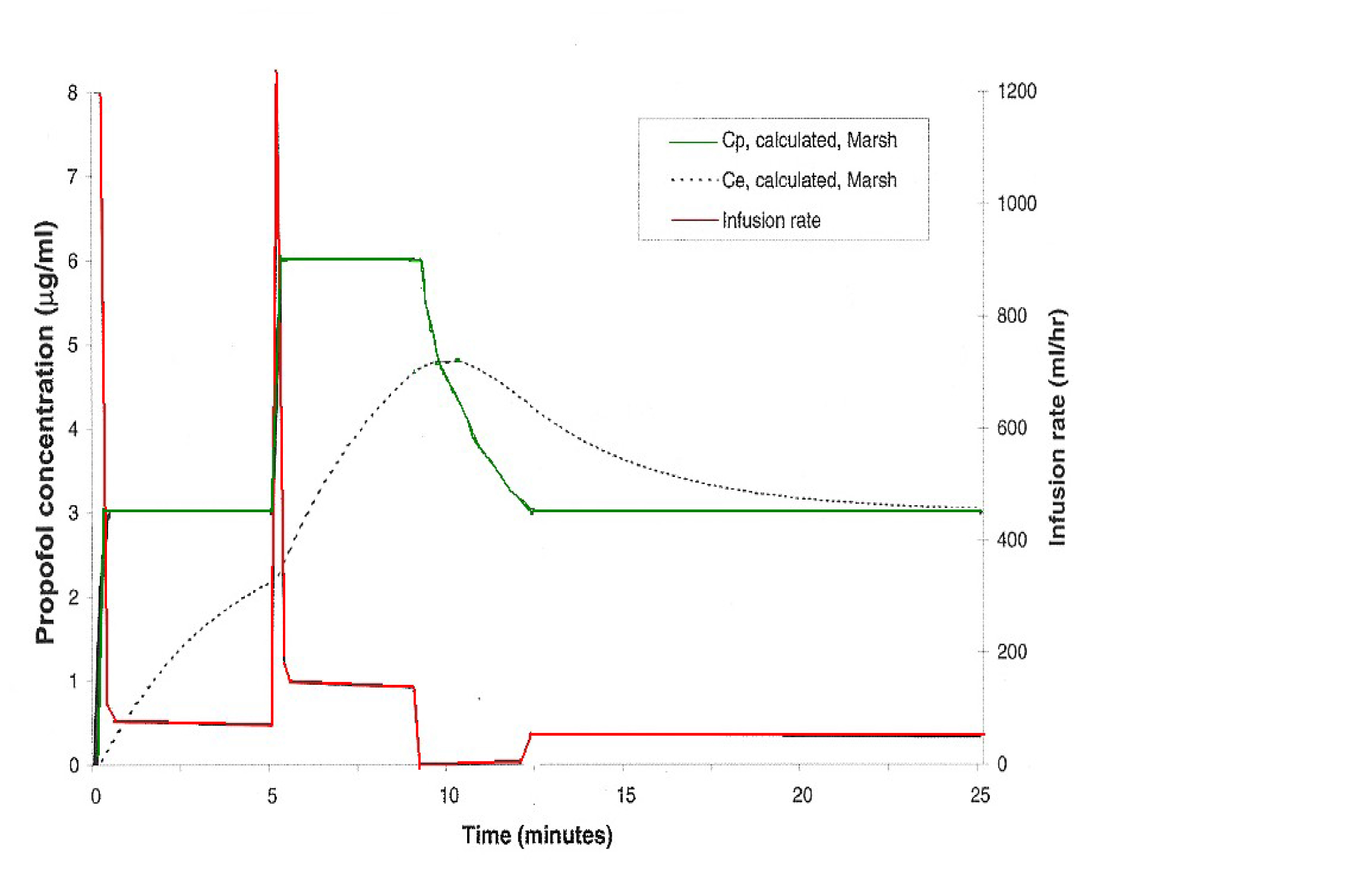
The above diagram explains the plasma and effect site concentrations during a target controlled infusion of propofol [Marsh model].
The initial target concentration is set at 3 micrograms per ml, then after five minutes the target concentration is altered to 6 micrograms per ml and at 10 minutes the target concentration is set back to 3 micrograms per ml.
It can be seen to achieve the set target plasma concentration [green line] the infusion rates constantly changes. An initial bolus dose achieves a plasma concentration of 3 micrograms per ml and the infusion rate is maintained at a steady level. At 5 minutes in order to achieve a target plasma concentration of 6 micrograms per ml, a bolus dose is delivered and the infusion changes to new steady infusion rate.
The amount infused is calculated according to the estimated central compartment volume and the difference between the current calculated concentration and target concentration. To achieve lower plasma levels the infusion pump may stop transfusing transiently till the new desired lower plasma concentration is achieved. Thus the TCI pump gives a bolus dose when a higher target concentration is set and usually stops transiently when a lower target plasma concentration is set. The TCI pump repeats its calculation at discrete intervals [typically every 10 seconds] and alters the infusion rate as necessary.
As the clinical effect of the drug depends on the concentration at the effect site, there is usually a hysteresis in the clinical effect when the target blood concentration of the agent is increased and then decreased. The rate of equilibration between blood and effect site depends on several factors, such as the rate of drug delivery, cardiac output, cerebral blood flow, lipid solubility and degree of ionisation of drug.
With a blood targeted TCI system, the user defined the blood concentration and the effect site concentration follows passively, with a time delay. With effect site targeting the system manipulates the blood concentration to bring about a target concentration as rapidly as possible. Anaesthetists planning to use effect site targeted system need to bear in mind that there are layers of assumptions inherent in the model.
Typical target concentration for remifentanil during induction and intubation are initially set at around 4 to 7 ng/ml. This could be soon reduced after intubation depending on the patients clinical response. Target concentrations up to 10 -15ng / ml may required during very stimulating procedures.
Accuracy of TCI infusions
There are changing pharmacokinetics of a drug with age and the effect site concentration is calculated and not measured. Rate of equilibration between blood and effect site depends on cardiac output, central blood volume, and other pharmacokinetic factors such as lipid solubility etc. The elderly have smaller central volume of distribution, decreased clearance and increased time to peak effect.
TCI in elderly and children
Several physiological factors influence the pharmacokinetics of drugs at extremes of age. In elderly there is a smaller central volume of distribution, decreased clearance, increased receptor sensitivity to drugs and increased time to peak effect. The elderly lose consciousness at lower blood concentrations of anaesthetic drugs and also develop cardio-respiratory compromise at increased concentrations. In the elderly and frail it is best when inducing anaesthesia with TCI propofol, to start at a very low target concentration and increase the target concentration in small steps every few minutes.
The use of TCI in children is not very popular. Children have a larger central volume of distribution and a rapid clearance in comparison with adults. In 1990s the accuracy of TCI propofol using Marsh model in 20 children were studied and found to be associated with a significant overestimation in blood concentrations. Consistent findings from several groups found pharmacokinetics of propofol differs between adults and children. Later models like the Paedfusor model performed better than the Marsh model. Currently there are no large randomised trials to establish their efficiency. There have been several reports of metabolic acidosis, lipaemia and fatty liver infiltration with use of prolonged propofol infusion in intensive care.
Practical aspects
Initial programming of pump is done based on patient’s weight, height age and sex. Programmes are made specific for the drug. [i.e. propofol or remifentanil]
Typical initial blood propofol induction concentrations would be in the order of 6 to 8mcg/ml in un-premedicated young adults. Caution should be exercised in elderly and those with cardiovascular instability. When consciousness is lost and again during manipulation of the airway it is advisable to take note of the estimated effect site propofol concentrations to assess patient’s sensitivity to propofol. After induction the target concentration should be increased or decreased as appropriate for the level of surgical stimulus.
During the intra-operative phase the patient should be observed closely and the target concentrations should be adjusted according to the clinical responses and will also be influenced by co-administration of other agents like remifentanil, benzodiazepines and other opiates. Toward the end of the case as the intensity of surgical stimulus reduces the target concentration can be gradually reduced to promote a more rapid recovery. Generally the infusion can be stopped once the final sutures or dressings have been applied. The machine usually gives us an estimated time for the patient to be awake, corresponding to a blood concentration of around 1.5 mcg/ml for propofol.
When propofol/remifentanil combinations are used it is the choice of the anaesthetist to decide which to commence first. It is important to know that the effect site remifentanil concentrations rise more rapidly than the propofol concentrations. Ideally therefore propofol should be started first to produce a faster induction. By commencing remifentanil infusion prior to propofol the patient is likely to stop breathing before losing consciousness and caution is required in those with difficult airway.
An infusion of remifentanil and propofol used intra-operatively is likely to result in significant postoperative pain once the infusions are stopped. Longer acting opioids such as morphine need to be administered towards the end of the surgery to establish adequate postoperative pain relief.
A dedicated intravenous line for the target controlled infusions is essential and vigilant monitoring of the cannula site checking for disconnection and tissuing are essential. It is important to bear in mind there is no definitive monitor analogous to the end tidal volatile agent monitor while using TCI pumps.
Future of TCI
Most models describe healthy volunteers and there is poor correlation in unwell patients. The trend of increasing obesity does alter pharmacokinetics and accuracy of the pumps. Closed loop TCI models with AEP and bispectral index monitoring feedback to the pumps are under development. More information on the new esterase anaesthetic agent [THRX98661] is awaited.
KEY POINTS
- Target concentrations are calculated, not measured.
- TCI pumps maintain three superimposed infusions, one at a constant rate to replace drug elimination and two exponentially decreasing infusions to match drug removed from central compartment to other peripheral compartments of distribution.
- At present in clinical use there is no method of measuring drug concentrations real time analogous to the end tidal volatile agent concentration.
References:
- Kruger-Thiemer. Continuous intravenous infusion and multicomparment accumulation. European Journal of Pharmacology 1968; 4:317-24.
- Principles and practice of Pharmacology for Anaesthetists. T.N. Calvey and N.E Williams.
Answers to MCQ’s
-
- True
- False
- False
- True
- True
-
- False
- True
- True
- False
- False
-
- True
- True
- True
- False
- False
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/