Obstetrics Anaesthesia

KEY POINTS
- Labour epidurals provide safe, effective analgesia with minimal side effects to mother and fetus
- Knowledge of anatomy and pain pathways are key to providing epidural analgesia to labouring parturients
- Consent can be challenging during active labour
- Labour epidurals are beneficial in certain circumstances: high probability of emergency operative delivery; patients with predictors of a difficult airway; and medical conditions benefiting from reducing the stress response of labour e.g. pre-eclampsia
- Risk of permanent nerve damage in obstetric epidurals may be as high as 1 in 80,000
- Combined spinal-epidurals (CSE), single-shot spinals (SSS), and dural puncture epidurals (DPE) are alternative neuraxial techniques to epidurals for labour analgesia
INTRODUCTION
Labour epidurals are popular and safe; they provide effective analgesia for labouring parturients. Lower dose epidural regimes limit motor block, do not affect progress of labour, and have minimal side effects to mother and fetus. Labour epidurals can also be used to provide anaesthesia for assisted vaginal delivery or caesarean section.
Specific circumstances when labour epidurals may be beneficial1
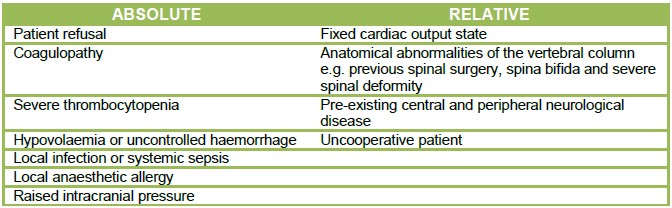
- Pre-eclampsia (without severe thrombocytopenia or coagulopathy)
- High Body Mass Index (BMI)
- Anticipated difficult airway or other risk factors for general anaesthetic
- High risk for assisted vaginal delivery e.g. breech or multiple gestation
- Trial of labour after previous caesarean section
- Maternal cardiovascular, cerebrovascular or respiratory disease1
- Spinal disorders when ‘urgent’ neuraxial anaesthesia placement may be difficult, for example with scoliosis
Contraindications to labour epidurals1:
Consent and risks for labour epidurals2
- 1 in 10 need further attention to help function (e.g. pull catheter back)
- 1 in 20 need catheter re-siting
- 1 in 100 accidental dural puncture
- 1 in 24,000 temporary nerve damage, such as temporary motor weakness or paraesthesia of a limb lasting less than 6 months
- 1 in 80,000 permanent nerve damage, such as permanent motor weakness or paraesthesia of a limb
- Bleeding, including epidural haematoma
- Infection, including epidural abscess
- Pruritus
- Hypotension
- Increased risk of assisted vaginal delivery
Informed consent for epidural insertion can be challenging in active labour. The process is improved if information can be given antenatally, e.g. with information leaflet.1 Retention of details of the consent discussion may be improved by requesting the parturient sign a written consent form prior to being in active labour.
ANATOMY OF THE LUMBAR SPINE AND THE EPIDURAL SPACE
Knowledge of lumbar spine anatomy is the cornerstone of providing safe labour epidural analgesia.
The vertebral column
The vertebral column provides support and protection for the spinal cord. There are five lumbar vertebrae, which have large vertebral bodies for weight-bearing, increasing in size from L1 to L5.3
Intervertebral discs separate each vertebral body. The spinal canal encloses the epidural and subarachnoid spaces. The vertebral bodies are connected anteriorly by the anterior longitudinal ligament and posteriorly (on the anterior wall of the vertebral canal) by the posterior longitudinal ligament; both extend from the occiput to the sacrum. Three ligaments are pierced during epidural insertion: supraspinous, interspinous, and the ligamentum flavum (Figure 1).
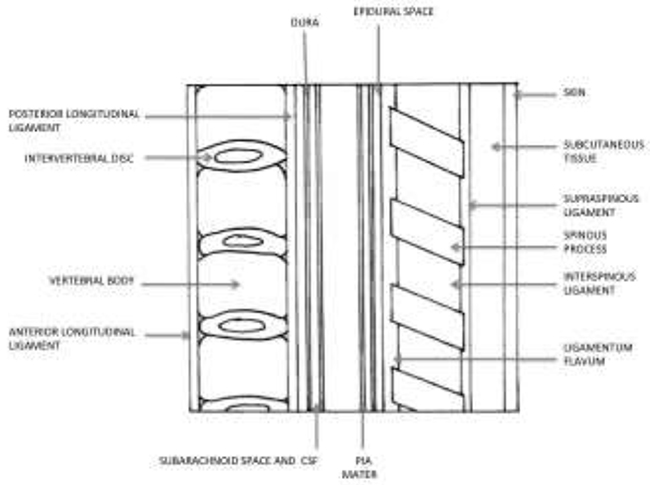
Figure 1. Anatomy relevant to epidural anaesthesia
The epidural space
The epidural space is a ‘potential space’ that surrounds the dura mater and extends from the foramen magnum to the sacral hiatus at the level of S2/3.
Boundaries of the epidural space are as follows:
- Superior fusion of the spinal and periosteal layers of dura mater at the foramen magnum
- Inferior sacro-coccygeal membrane
- Anterior posterior longitudinal ligament, vertebral bodies and intervertebral discs
- Lateral pedicles and intervertebral foramina
- Posterior ligamentum flavum and vertebral laminae
The epidural space contains fat, spinal nerve roots, spinal arteries, extra-dural venous plexuses, connective tissue, lymphatics and the dural sac.4
In adults the spinal cord most commonly ends at L1-L2 (L3 in 10% of adults), the dural sac ends at S2, continuing below this is the filum terminale, which attaches to the coccygeal ligament.5
Surface anatomy
Knowledge of surface anatomy is essential in identifying the correct vertebral level for epidural insertion. An imaginary line is drawn between the top of the iliac crests, which corresponds to the level of the L4 spinous process or the L4-L5 interspace, and is known as “Tuffier’s line”. In parturients, Tuffier’s line crosses the spine at a higher level (L3-4) due to the forward rotation of the pelvis.6 As a result anaesthetists are often at a higher level than anticipated. This is especially pertinent when a CSE technique is being planned.7 Pre-puncture neuraxial ultrasound can help confirm the correct vertebral level, midline and depth of the epidural space.8
Pain pathways in labour
During the first stage of labour, afferent nerve impulses from the lower uterine segment and cervix cause visceral pain, which is poorly localised and diffuse in nature. These nerve cell bodies are located in the dorsal root ganglia of T10 to L1. During the second stage of labour, afferent nerves innervating the vagina and perineum cause somatic pain, which is better localised. These somatic impulses travel primarily via the pudendal nerve to dorsal root ganglia of S2 to S4.9
The ideal labour epidural block should cover sensory loss from T10 – S5 dermatomes (with minimal motor block) to provide analgesia for the first and second stages of labour.
Patient positioning for neuraxial blockade
Insertion of labour epidurals is commonly performed in either the sitting, or the flexed lateral position. Positioning is governed by maternal comfort and compliance, as well as anaesthetist preference. Epidural placement in the sitting position has a higher success rate of first-pass insertion and the procedure can be performed faster compared with the lateral position.10
Equipment and Insertion Technique
The basic equipment required for epidural Insertion is:
- Scrub Pack: Hibiscrub, surgical hat, mask, gown, gloves
- Sterile Pack with swabs and drape
- Cleaning solution e.g. Chlorhexidine 0.5%
- Local anaesthetic for skin e.g. 1% lignocaine
- 0.9% saline
- Tuohy needle (18 or 16G)
- Loss of resistance syringe
- Epidural catheter
- Epidural filter
- Epidural lock/device for securing epidural to skin
A loss of resistance technique for epidural insertion can be performed with either air (LORA) or saline (LORS). There are case reports of pneumocephalus and an increased incidence of dural puncture and patchy blocks with LORA, therefore LORS is more commonly practiced.11
NEURAXIAL TECHNIQUES ON LABOUR WARD: WHAT ARE THE OPTIONS?
There are alternative neuraxial techniques to the traditional labour epidural. The first choice technique may differ with anaesthetist experience, institutional preference and the clinical situation.
Labour epidural
Labour epidurals do not increase caesarean section rates, but marginally prolong the second stage of labour and increase assisted vaginal delivery rates.12 Labour epidurals improve maternal pain and satisfaction scores in comparison to systemic analgesics and are the most effective analgesic option for labour.
Modern labour epidural dosing regimens (e.g. 0.0625% to 0.1 % bupivacaine with 2-4 mcg/ml fentanyl or 0.4 mcg/ml sufentanil) reduce the total local anaesthetic dose required and motor block experienced; potentially allowing the parturient to be ambulatory.13
There a several different regimes for administering labour epidural analgesia. Current practices are: intermittent physician or nurse bolus, Patient Controlled Epidural Analgesia (PCEA), Programmed Intermittent Epidural Boluses (PIEB) or continuous infusions.
Labour epidurals provide safe continuous analgesia throughout labour and can be converted with higher concentration local anaesthetic top-up to anaesthesia for operative delivery.
Combined Spinal-Epidural (CSE)
A CSE combines rapid onset of analgesia from the spinal component, with the benefit of continuing labour analgesia with the epidural catheter. A CSE can be performed as an individual single-shot spinal followed by placement of an epidural catheter as a separate technique (see below), or with a needle-through-needle technique. For dosing of the CSE’s spinal component, please see single-shot spinal section below.
When comparing CSEs with labour epidurals, there is no difference in: unintentional dural puncture; incidence of post Dural Puncture Headache (PDPH); rescue analgesia requirements; maternal satisfaction scores; and mode of delivery. There is an increased risk of transient hypotension and fetal bradycardia requiring intervention with CSE compared with labour epidural.14
CSE is a slightly more complicated technique and there is a theoretical risk of having an untested epidural catheter for labour analgesia and surgery if close to the time of CSE placement.
The 3rd National Audit Project2 in the UK showed there was an increased overall risk with the use of CSEs compared to epidurals. Both the optimistic and pessimistic interpretations of the incidence of permanent harm, and paraplegia or death per 100,000 was greater for CSEs than epidurals when used perioperatively in the general patient population. This was not shown in obstetric patients.
Single-shot spinal
Single-shot spinal block for labour analgesia can provide pain relief for immediate delivery.15 Multiparous parturients are probably the most suitable candidates for this technique due to rapid labour progression. A dose of 2.5mg bupivacaine and 25mcg fentanyl has been shown to last up to two hours in duration.15
There is greater incidence of transient hypotension and fetal bradycardia with a single-shot spinal compared with an epidural.2 The anaesthetist should anticipate this and have phenylephrine, ephedrine, and/or glyceryl trinitrate (GTN) immediately available. Transient hypotension may contribute to the fetal bradycardia but it is most likely to be caused by increased uterine tone secondary to the rapid reduction in circulating catecholamines (especially adrenaline/epinephrine). Administering GTN (intravenously or sublingually) provides tocolysis improving the fetal bradycardia.
Single-shot spinal followed by epidural
A single-shot spinal can be immediately followed with an epidural. This is a useful technique in a distressed parturient to facilitate fast pain relief and better positioning.
Dural Puncture Epidural (DPE)
An alternative for labouring parturients is the DPE technique. This technique is similar to a CSE, performing an intentional dural puncture with a spinal needle but without administering intrathecal drugs. DPE avoids the potential haemodynamic instability caused by intrathecal local anaesthetics and enhances labour analgesia when compared with standard epidural techniques.16 DPE improves analgesia compared with epidurals alone by “epidural rent” of the intrathecal space; when there is a puncture in the dura the anaesthetic can flow from the epidural space into the intrathecal space. This technique, along with the CSE technique allows partial confirmation of epidural catheter placement, e.g. cerebrospinal fluid (CSF) is seen in the spinal needle placed through the epidural needle, and therefore the epidural catheter itself is more likely to be midline.
The DPE technique is not currently widely practised.
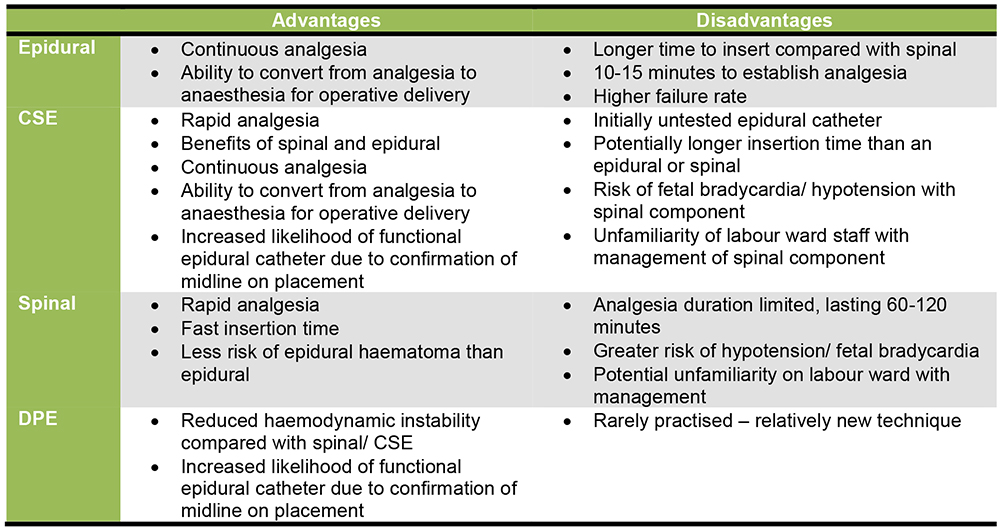
Table 1. Advantages and disadvantages of neuraxial techniques for labour analgesia
Test dose
An epidural test dose can identify inadvertent intrathecal or intravascular catheter placement. Unidentified intrathecal or intravascular epidural catheter placement can lead to a high or total spinal, or local anaesthetic systemic toxicity (LAST).
Historically, 3ml of 1.5% lidocaine with 1 in 200,000 adrenaline (epinephrine) was used as a ‘test dose’: intrathecal lidocaine would rapidly produce evidence of a spinal block; intravenous adrenaline would produce transient tachycardia. However, using adrenaline is unreliable (low sensitivity) because of confusion with transient tachycardia seen with contraction pains.16 – 17
The current trend is towards using low dose local anaesthetic without adrenaline as a ‘test dose’. This helps reduce motor block, thereby allowing better chance of ambulation. There is a large variation in drugs/ doses currently used for test doses, with ranges of 3-20 mg bupivacaine and 15-90 mg lidocaine.18 Every dose administered via an epidural catheter, whether to initiate a block, or treat breakthrough pain should be treated as a ‘test dose’ as catheters can migrate intrathecally and intravascularly, despite initially being placed correctly in the epidural space.
REFERENCES AND FURTHER READING
- Obstetrics Anaesthetists Association. Available from: http://www.oaaanaes.ac.uk/assets/_managed/editor/File/Guidelines/epidural%20for%20labour/ Painrelief_for_labou_Swales_Southampton.pdf (accessed 14 January 2016)
- The 3rd National Audit Project of the The Royal College of Anaesthetists. Available from: http://www.rcoa.ac.uk/system/files/CSQ-NAP3-Full_1.pdf (accessed 14 January 2016)
- Lumbar Spine Anatomy. Available from: http://emedicine.medscape.com/article/1899031-overview (accessed 14 January 2016)
- Richardson J, Groen G. Applied Epidural Anatomy. Contin Educ Anaesth Crit Care Pain 2005;5(3):98-100
- Barash PG, Cullen BF, Stoelting RK et al. Clinical anesthesia. 6th Edition. 1989. p565.
- Bucklin B, Gambling D, Wlody D. A Practical Approach to Obstetric Anaesthesia. 1st Edition. 2009. P145
- Margarido CB, Mikhael R, Arzola C et al.The intercristal line determined by palpation is not a reliable anatomical landmark for neuraxial anesthesia. Can J Anaesth 2011;58(3):262-6
- Amin WA, Osama Abou Seada M, Bedair EMA et al. . Comparative study between ultrasound determination and clinical assessment of the lumbar interspinous level for spinal anaesthesia. M E J Anesth 2014;22(4):407-12
- Shorthouse JR. SAQs for the Final FRCA Examination (Oxford Specialty Training Revision Texts) Paperback 28 July 2011
- Nishi M, Usukaura A, Kidani Y et al. Which is a better position for insertion of a high thoracic epidural catheter: sitting or lateral decubitus? J Cardiothorac Vasc Anesth. 2006;20(5):656-8
- Nistal-Nuño B, Gómez-Ríos MÁ. Case Report: Pneumocephalus after labor epidural anesthesia. F1000Research.2014; 3:166.
- Gaiser RR. Labor epidurals and outcome. Best Pract Res Clin Anaesthesiol. 2005;19(1):1-16
- Sunil T. Labour analgesia: Recent advances. Ind J Anaesth 2010;54(5):400–408
- McGrady E, Litchfield K. Epidural analgesia in labour. Contin Educ Anaesth Crit Care Pain 2004;4(4):114-17
- Viitanen H, Viitanen M, Heikkila M. Single-shot spinal block for labour analgesia in multiparous parturients. Acta Anaesthesiol Scand 2005;49(7):1023-9
- Cappiello E, O’Rourke N, Segal S et al.A randomized trial of dural puncture epidural technique compared with the standard epidural technique for labor analgesia. Anesth Analg 2008;107(5):1646-51
- Hermanides J, Hollmann MW, Stevens MF et al. Failed epidural: causes and management. Br J Anaesth 2012;109(2):144-54
- Gardner IC, Kinsella SM. Obstetric epidural test doses: a survey of UK practice. Int J Obstet Anesth. 2005 Apr;14(2):96-103.
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/