General Topics
Tutorial 292

QUESTIONS
Before continuing, try to answer the following questions. The answers can be found at the end of the article, together with an explanation.
- Describe the anatomical columns of the cervical spine.
- What are the potential difficulties with the airway?
- What are the signs and symptoms of autonomic hyper-reflexia?
INTRODUCTION
- There are approximately 10,000 cases of acute spinal cord injury in the US every year.
- These are often associated with other severe trauma with or without traumatic brain injury.
- Risk factors for injury:
- Age
- Youth (risk taking behaviour)
- Older adults (age related degeneration and falls)
- Gender: males more than females
- Alcohol or drug use
- Motor vehicle collisions.
- Age
Patterns of injury include:
- Hyperflexion: due to a blow to the back of the head or deceleration; often stable with no neurological damage.
- Hyperflexion-rotation: disruption of posterior ligamentous complex, may cause cervical root injury usually without spinal cord damage.
- Axial loading (vertical compression): causes loss of vertebral body height with disruption of the vertebral body; it may displace posteriorly causing cord damage although the spine remains relatively stable.
- Hyperextension: due to applied force to the front of the head or severe whiplash injury; more common than flexion injuries; often associated with cord injury (for example, a “hangman’s fracture,” fracture of both pedicles or pars interarticularis of C2, the axis).
- Hyperextension-rotation: a very unstable combination, associated with a high incidence of cord damage.
- Lateral flexion: often associated with flexion or extension injuries.
The pathophysiology of injury:
- Primary injury causes microscopic haemorrhages in grey matter and oedema of white matter of cord. Microcirculation is impaired by oedema and haemorrhage, further compromised by vasospasm.
- Necrosis of grey and white matter occurs. Function of nerves through the injured area is lost.
- Acceleration and deceleration, as occurs in motor vehicle accidents and falls, is the most common mechanism of abnormal spinal column movements.
- Other causes include penetration by bullets or foreign objects.
Instability
- Instability can be defined as “the loss of ability of the cervical spine under physiological loads to maintain relationships between the vertebrae in such a way, that spinal cord or nerve roots are not damaged or irritated and deformity or pain does not occur” (Leemans and Calder, 2012 – see further reading).
- The spine consists of three columns:
- Anterior: consisting the anterior longitudinal ligament and the anterior half of the vertebral body
- Middle: comprising the posterior half of the vertebral body, disc, annulus and the posterior longitudinal ligament
- Posterior: made up of the facet joints, their ligaments and the ligamentum flavum.
- Loss of any of these columns can cause instability.
- The most commonly affected regions are cervical (C1, C2 and C4-C6) and thoraco-lumbar junction (T11 to L2).
- Cervical spine instability may also be caused or exacerbated by chronic conditions – rheumatoid arthritis, ankylosing spondylitis, infection, tumors or congenital conditions such as Klippell-Feil or Down’s syndrome.
Assessment of level of injury
- Manifestations of injury at cervical level:
- Paralysis or weakness of all limbs
- Respiratory distress
- Pulse < 60bpm; blood pressure < 80mmHg
- Decreased peristalsis.
- Manifestations of injury at thoracic or lumbar level:
- Flaccid paralysis or weakness of legs
- Spinal shock
- Loss of skin sensation
- Areflexia
- Absent bowel sounds
- Bladder distention
- Loss of cremasteric reflex in male.
- The American Spinal Injury Association impairment scale (figure 1) is widely used by neurosurgeons to aid assessment.
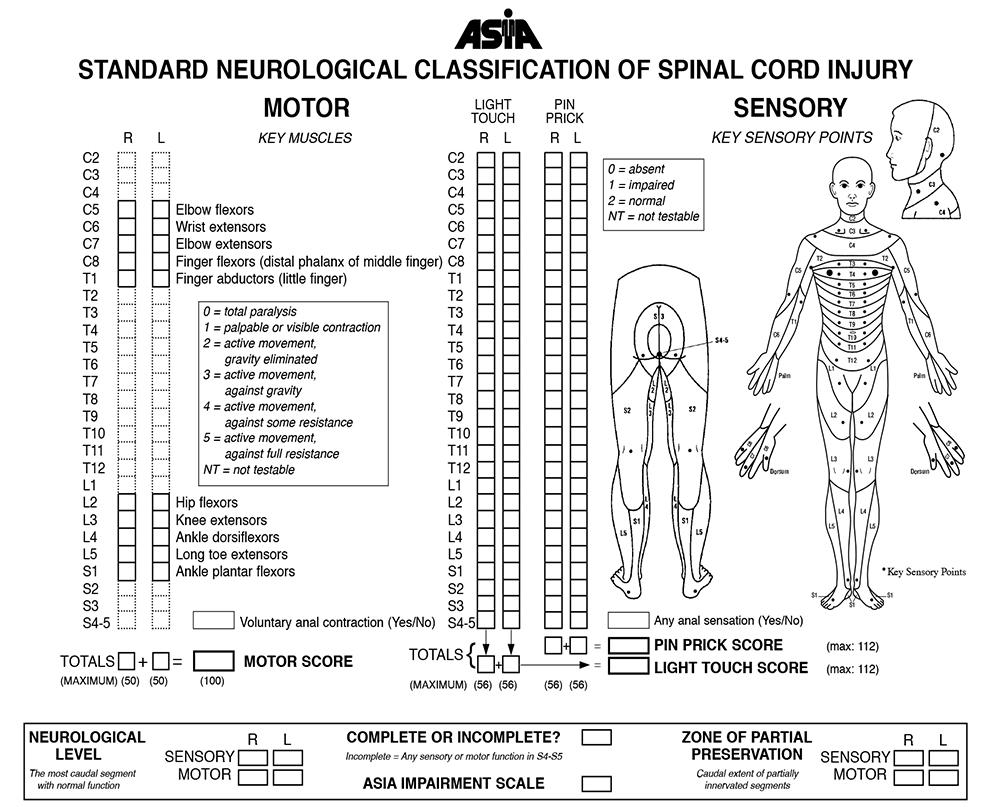
Figure 1. The American Spinal Injury Association impairment scale
MANAGEMENT
- All patients with major trauma should be considered to have a potential cervical spine injury unless proven otherwise.
- Care must start at scene of injury to reduce injury and preserve function.
- It involves rapid assessment of ABC (airway, breathing, circulation). Immobilise and stabilise head and neck, use cervical collar before moving onto backboard.
- Take care with all transfers not to aggravate original injury.
- Injuries at C1 – C4 may result in respiratory paralysis but advances in trauma care allow patients to survive with ventilator assistance.
- Address other injuries that necessitate immediate care.
Clearing the C-spine
- The C-spine of awake and alert patients may be cleared by history of a low risk mechanism and normal physical examination (using the Nexus criteria or Canadian C-spine rule).
- Given the probability of head injury or other significant trauma this is not always possible.
- For these patients, a multi-slice CT scan should be performed, this is most practical at the same point as a CT head. Scanning should be from occiput to T1 and allow sagittal and coronal reconstruction to exclude ligamentous instability. This should be as soon as practically possible, and is advisable within 72 hours.
- CT scanning has a very high sensitivity so unless there is a very strong suspicion of injury, a normal scan can be used to clear the C-spine to minimise the potential complications from prolonged immobilisation.
Airway Management
- The anaesthetist may need to secure an airway in a patient with an unstable cervical spine for resuscitation or subsequent surgery, including on other trauma injuries.
- It is advisable to perform a detailed assessment of the neurological deficit before intubation, if practical.
- The basic principle is to maintain a patent airway whilst minimising any potential risk to the cervical spine.
- Every patient with a suspected cervical injury should be considered a potential difficult airway, due to:
- Inability to achieve optimal positioning because of inline manual stabilisation or collar
- Presence of blood, secretions or oedema secondary to the initial injury.
- The main choice for the anaesthetist is between awake fibreoptic intubation (FOI) and intubation by direct laryngoscopy with inline manual stabilisation (or asleep FOI).
- Awake FOI should only be attempted by an experienced practitioner and is not advisable in situations where a patient cannot be co operative (for example – intoxication or head injury).
- Careful use of sedation and appropriate use of local anaesthetics can smooth the process and minimize any sympathetic response.
- An acceptable dose of lignocaine is as high as 9mg/kg, given the small amount of systemic absorption.
- This may be combined with cautious use of sedation, such as a remifentanil infusion.
- Awake FOI allows the anaesthetist to assess neurology after intubation and prior to surgery.
- Direct laryngoscopy should use a minimum amount of force.
- Many advocate the use of a bougie to minimise the force required. Some studies have suggested no significant increase in complications, hypoxia or time to intubation with bougie use.
- Video laryngoscopes may improve the view at laryngoscopy. They may require less force to obtain the view, although should only be used by those experienced in its practice in this situation.
- The use of cricoid pressure to minimise passive regurgitation of gastric contents may be necessary in unfasted patients but it may worsen intubating conditions and may possibly worsen C-spine instability. Suction should be on and readily accessible.
- We recommend inline manual stabilisation keeping in place the posterior part of the collar to reduce risk of movement.
- High spinal injuries cause significant respiratory dysfunction and these patients need airway control to maintain oxygenation and carbon dioxide clearance, even if there is no urgent operative intervention.
- Development of extra-junctional acetylcholine receptors makes the potential for significant hyperkalaemia when using suxamethonium. It should not be used later than 72 hours after the injury.
Conduct of Anaesthesia
- Whilst airway management is crucial, the anaesthetist has to maintain a perfusion pressure to the damaged cord.
- Given the possibility of altered haemodynamics, we aim for a MAP of at least 80mmHg.
- Invasive arterial blood pressure monitoring is mandatory for any spinal cord injury. As with other neurosurgical cases, large fluctuations in pressure are probably worse than a single brief episode.
- Ventilation should maintain PaCO2 within normal range (33-35mmHg).
- Large bore IV access is required given the possibility of significant blood loss and central venous access to facilitate vasopressor infusion to manage spinal shock.
- Serial serum lactates can asses progression of shock.
- Careful intra-operative positioning can improve surgical access and decreases the risk of venous congestion, for example from compression of the inferior vena cava.
- Spinal surgery is high risk for damage to vulnerable, pressure areas, particularly the eyes.
- It is critical that the eyes are well protected with no external pressure.
- A review of those with visual loss following surgery found that obesity, male gender, Wilson frame use, increased duration and greater blood loss were all risk factors.
- We advocate the use of a skull fixation device to reduce morbidity.
- Analgesic requirements will depend on the nature of surgery – some patients will have lost sensation below the level of injury.
- When sensation remains, operations may be particularly painful due to the dissection of spinal muscles.
- All patients will need to go to a high dependency area post-operatively.
- The level of injury may necessitate returning the patient to an intensive care bed prior to “waking up.” Determining whether to extubate a patient will be a “case-by-case” decision.
- Doubt over the patient’s ability to ventilate or prolonged, extensive surgery or significant blood loss increase the probability of postoperative ventilation.
- Approximately, a vital capacity while intubated of greater than 20mg/kg would support early extubation.
SPECIAL SITUATIONS
Neurogenic Shock
- Cervical spinal injury, particularly transection, can cause profound cardiovascular instability.
- The loss of sympathetic vasoconstriction results in venous pooling of blood, whilst absence of sympathetic cardiac input prevents a compensatory tachycardia.
- Careful fluid resuscitation and early introduction of vasopressors can help counter hypotension.
- Invasive monitoring is mandatory and should include CVC.
Autonomic Hyper-reflexia
- In the weeks following a high spinal injury (above T6), stimulation of the autonomic nervous system can lead to profound systemic symptoms, including hypertension, tachycardia, flushing, sweating and headaches.
- A stimulus, often from the bladder or bowel, causes nerve conduction up the spinal cord until terminated by the level of injury.
- A reflex is activated that increases activity of the sympathetic portion of the autonomic nervous system.
- This results in spasms and vasoconstriction, which causes a rise in the blood pressure. This is detected by the brain but due to the injury, cannot respond.
- For these patients, spinal anaesthesia may be useful although technically difficult.
- Otherwise, deep general anaesthesia reduces the risk of complications.
KEY POINTS
- Cervical spine injury is commonly associated with other trauma
- Airway maintenance is paramount but must ensure there is no contributory damage to the spinal cord
- Cervical spine injury can be complicated by respiratory failure, neurogenic shock or, later autonomic hyper-reflexia
ANSWERS
- There are three anatomical columns in the cervical spine that contribute to stability. The anterior consisting the anterior longitudinal ligament and the anterior half of the vertebral body; the middle comprising the posterior half of the vertebral body, disc, annulus and the posterior longitudinal ligament; and the posterior made up of the facet joints, their ligaments and the ligamentum flavum.
- All patients with cervical spinal injuries should be considered to have potentially difficult airway due to the presence of blood, oedema or secretions and due to the inability to achieve optimal positioning because of inline manual stabilisation or collar. The patient may be confused due to head trauma or intoxication or may have other significant trauma.
- Autonomic hyper-reflexia causes hypertension, tachycardia, flushing, sweating and headaches following visceral stimulation in those who have suffered a high spinal injury.
FURTHER READING and REFERENCES
- Leemans M. and Calder I.. The Unstable Cervical Spine. In: (eds) Johnston I., Harrop-Griffiths W. and Gemmell L. AAGBI Core Topics in Anaesthesia 2012. Chichester, UK: Wiley-Blackhall; 2012. p88-104.
- American Spinal Injury Association. ASIA Exam Sheet for International Standards for Neurological Classification of Spinal Cord Injury. 2011. Available at http://www.asia-spinalinjury.org (Accessed 18/01/2013).
- Nolan J.P and Wilson M.E.. Orotracheal intubation in patients with potential cervical spine injuries. Anaesthesia 2007 48 (7): 630-3.
- Postoperative Visual Loss Study Group. Risk factors associated with ischemic optic neuropathy after spinal fusion surgery. Anesthesiology 2012 116 (1): 15-24.
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/