Paediatric Anaesthesia

KEY POINTS
- The lumbar plexus is derived from the anterior rami of lumbar nerve roots L1 to L4, with variable contribution from T12 and L5, and provides innervation of the hip joint, anterior and medial compartments of the thigh, and the femur.
- The lumbar plexus block can provide analgesia for hip, proximal femur, and anterior thigh surgery, and may be combined with sciatic nerve blocks for complete unilateral lower limb analgesia.
- The lumbar plexus block is located within the psoas muscle, which is a noncompressible space, and is considered a ‘deep’ peripheral nerve block. It should not be performed in patients with coagulation disorders due to the risk of haemorrhage with inadvertent vascular or renal puncture.
- The use of ultrasound allows identification of key anatomic landmarks for block placement, including transverse process, psoas muscle, and blood vessels.
- The lumbar plexus nerves may be difficult to visualise on ultrasound; therefore, a combined technique utilising both ultrasound and peripheral nerve stimulation is recommended to decrease the risk of inadvertent nerve injury.
- The lumbar plexus block requires advanced regional and ultrasound skills due to the complexity of the sonoanatomy, the deep location of the lumbar plexus, and potential for complications (eg haematoma, epidural spread).
- The deep location of the lumbar plexus facilitates a well-anchored placement of a catheter. Placement of a catheter allows for a continuous infusion of local anaesthetic thus prolonging the duration of analgesia.
INTRODUCTION
The lumbar plexus (LP) is a web of nerve roots located within the psoas muscle and forms part of the larger lumbosacral plexus.1 Blockade of this plexus (lumbar plexus block) may be performed to provide intraoperative and postoperative analgesia for hip, proximal femur, and anterior thigh surgery, and in combination with sciatic nerve blocks for thigh and knee surgery.2,3 The psoas muscle compartment is a noncompressible space; therefore, the LP block is considered a ‘deep’ peripheral nerve block and advanced skills and training are required.
Traditionally this block has been performed using surface landmark and peripheral nerve stimulator techniques. Its use has been limited due to the increased risk of inadvertent vascular or renal injury.4,5 More recently, ultrasound-guided techniques have been developed for performing this block that improve its safety profile. The use of ultrasound allows for real-time visualisation of the needle and relevant nearby anatomy. However, due to the depth, well-defined sonographic visualisation of the LP nerves may be challenging. Therefore, a combined approach using an ultrasound along with a peripheral nerve stimulation technique is recommended to ensure safe needle placement.6
Anatomy
The LP is derived from the anterior rami of lumbar nerve roots L1 to L4, with variable contributions from T12 and L5.1,7 These roots divide into anterior and posterior divisions within the psoas major muscle. They join to form 6 major nerves: iliohypogastric nerve, ilio-inguinal nerve, genitofemoral nerve, femoral nerve, obturator nerve, and lateral cutaneous nerve of the thigh (Figure 1). The origin and function of each of these branches are outlined in Table 1.1,7
The obturator nerve emerges on the medial border of the psoas muscle, the genitofemoral nerve emerges on the anterior surface, and the remaining nerves run along the lateral border of the psoas muscle (Figure 2).
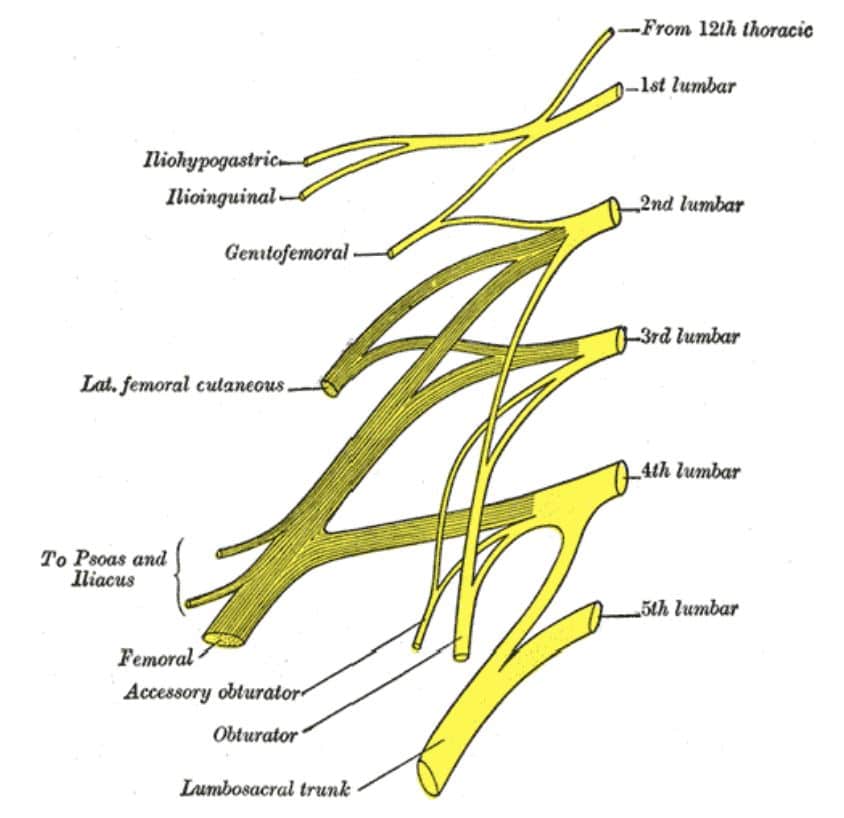
Figure 1. Lumbar plexus anatomy. Source: Public domain.8
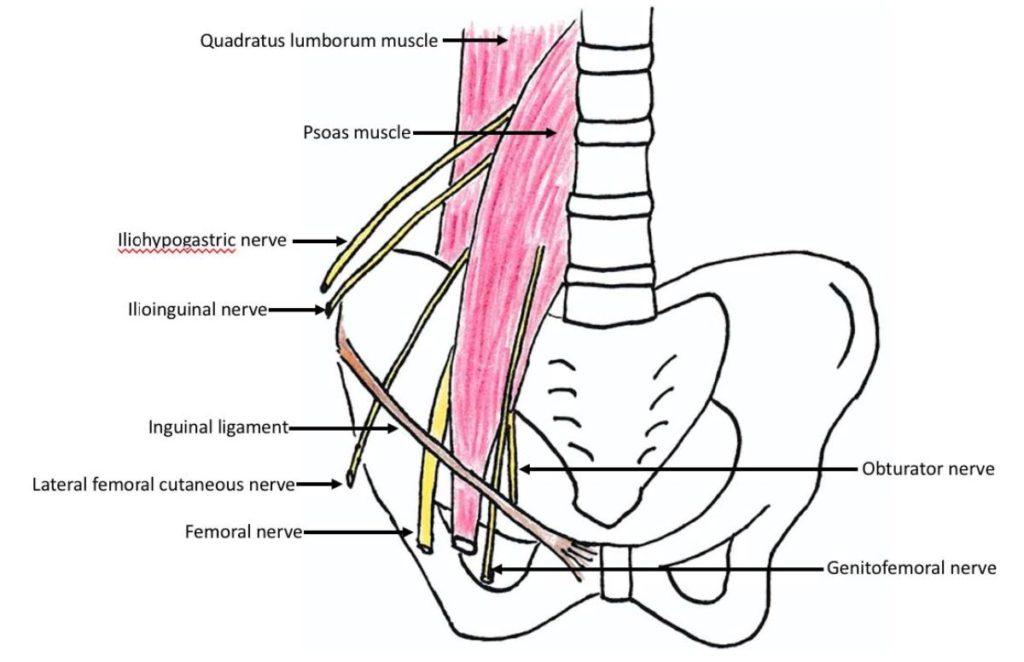
Figure 2. Relationship between the lumbar plexus nerves and the psoas muscle. Source: illustration by tutorial author C.C.
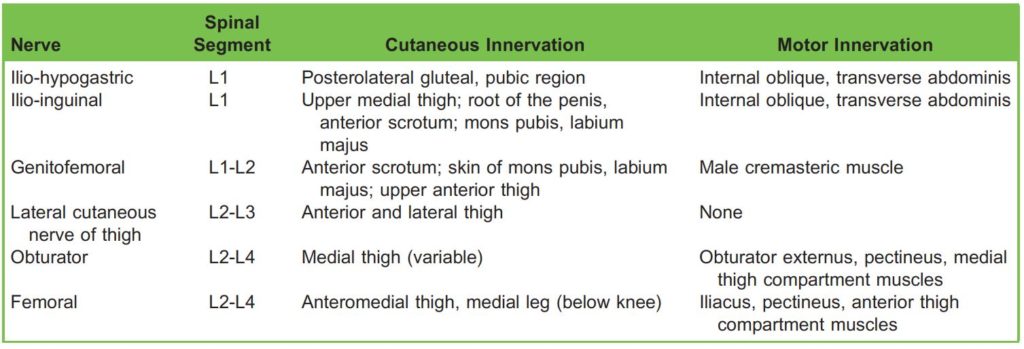
Table 1. Sensory And Motor Functions of Nerves Arising From the Lumbar Plexus
The LP is located within the ‘psoas compartment’, which is a deep fascial plane within the posterior one-third of the psoas muscle. The lateral cutaneous nerve of the thigh and the femoral nerve are located in the psoas muscle compartment. The obturator nerve has a variable location, and may lie in a different intramuscular fold, separated from the lateral cutaneous nerve of the thigh and the femoral nerve.6 The obturator nerve is spared in approximately 10% of LP blocks, and this is likely due to its variable location.
The psoas muscle is anterior to the transverse processes of the lumbar vertebrae.1 The erector spinae muscle complex is located posterior and medial, and the quadratus lumborum muscle is located lateral to the psoas muscle (Figure 3).1 The kidney is located anterior and lateral to the psoas muscle, usually at the L2-L3 level but may be lower, at the L4-L5 level, in
young children and infants and those with significant curvature of the thoracolumbar spine. The dorsal branch of the lumbar artery is located between the psoas muscle and the transverse process and the psoas compartment itself contains a network of arteries and veins (Figure 3).1,4
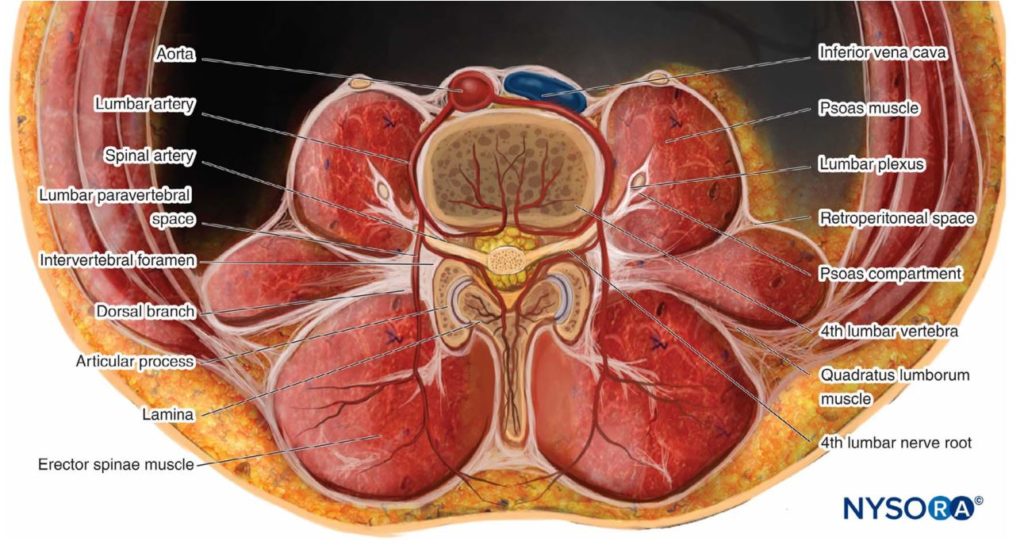
Figure 3. Transverse anatomy of the lumbar paravertebral region at the L4 vertebral level. Source: Reprinted with permission from New York School of Regional Anesthesia.6
Obtaining high-quality sonographic visualisation of the LP neural structures may be challenging, particularly in adolescents and adults.8 The depth of the LP varies with weight, rather than age (Figure 4).9 Typically, in younger children the LP is more superficial and therefore less sonographic tissue penetration is required. Higher ultrasound frequencies can be used allowing for better image resolution (Figure 4). Furthermore, in younger children, there are fewer fibrous structures within the psoas muscle compared to adults. There is greater contrast between the hypoechoic muscle tissue and hyperechoic neural structures of the lumbar plexus, and the LP nerves are more easily visualised.9
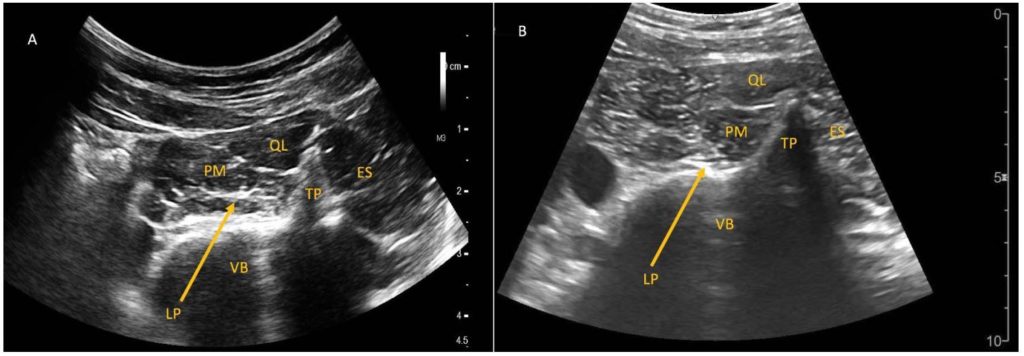
Figure 4. Shamrock approach to lumbar plexus block in (A) 18-kg 5-year-old; (B) 68-kg 20- year-old. The lumbar plexus is located more superficial and has greater resolution in the 18-kg child (2 cm depth) compared to in the 68-kg adult (5 cm depth). TP indicates transverse process; VB, vertebral body; PM, psoas muscle; LP, lumbar plexus; ES, erector spinae muscle; QL, quadratus lumborum muscle. Patient or parent permission obtained for use of images.
INDICATIONS, CONTRAINDICATIONS, AND COMPLICATIONS
Indications
The LP block provides analgesia for surgeries of the hip, proximal femur, and anterior thigh, and may be combined with a sciatic nerve block to achieve entire unilateral lower limb analgesia (eg above- or below-knee amputation procedures). For both adults and children, it is often used in conjunction with general anaesthesia. The LP block is not commonly used as the sole anaesthesia technique because it tends to be used for operations that are several hours in duration and are associated with significant blood loss. Furthermore, the obturator nerve is spared in 10% of LP blocks, limiting its usefulness as a sole anaesthesia technique.
In comparison to analgesia provided by central-neuraxial blockade, a unilateral LP block offers some advantages:
- A unilateral sympathectomy may prevent the intraoperative haemodynamic instability that can occur with central-neuraxial blockade.
- The motor and sensory function of the opposite lower limb is preserved.
- When compared to a single-injection caudal block, a single-injection LP block provides greater duration of analgesia and a decrease in opioid requirements.10
- It does not cause urinary retention and urinary catheterisation is not required.10
- It may allow earlier postoperative mobilisation compared to central-neuraxial blockade.
The LP block may be advantageous compared to more distal peripheral nerve blocks as multiple nerves are blocked by a single injection or placement of a single continuous catheter infusion.
Contraindications
See Table 2 for absolute and relative contraindications.

Table 2. Absolute and Relative Contraindications
Complications
While the use of ultrasound is believed to improve the safety and efficacy of LP blocks when compared to surface landmark or nerve stimulator techniques, there is minimal published data to support this claim. When performing an LP block, if the needle is inserted too medial or too deep, injury to major blood vessels and organs such as the kidney, aorta, lumbar arteries, vena cava and bowel, may occur (Figure 5). See Table 3 for generic and specific complications.
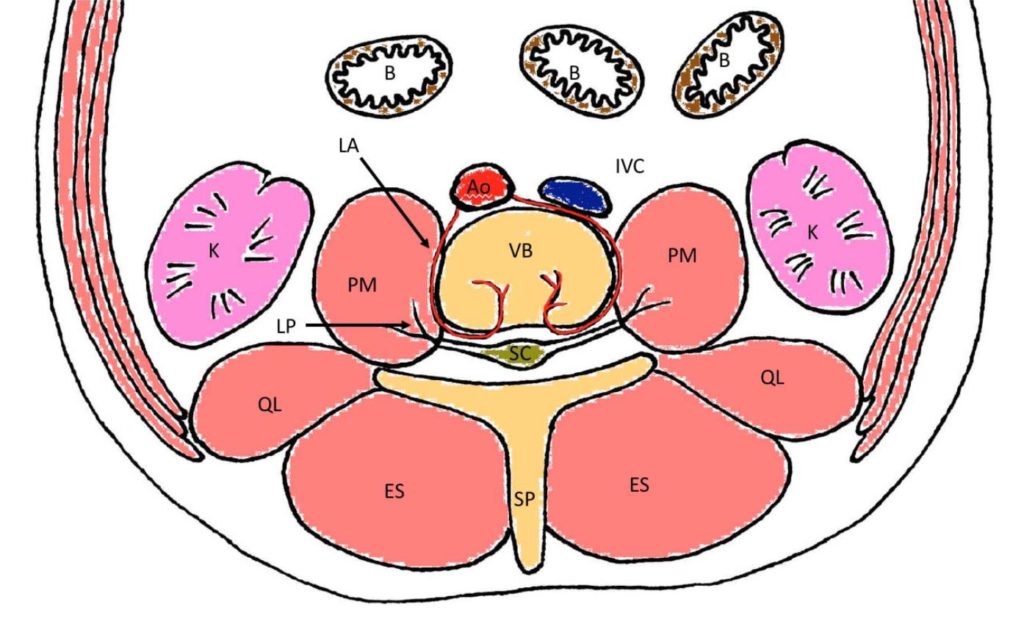
Figure 5. Transverse cross-section of the lumbar region at the L4 vertebral level, demonstrating potential organs and vessels that may be injured during lumbar plexus block. Ao indicates aorta; IVC, inferior vena cava; LA, lumbar arteries; VB, vertebral body; PM, psoas muscle; SP, spinous process; LP, lumbar plexus; QL, quadratus lumborum muscle; ES, erector spinae muscle; K, kidney; B, bowel; SC, spinal cord. Source: illustration by C.C.
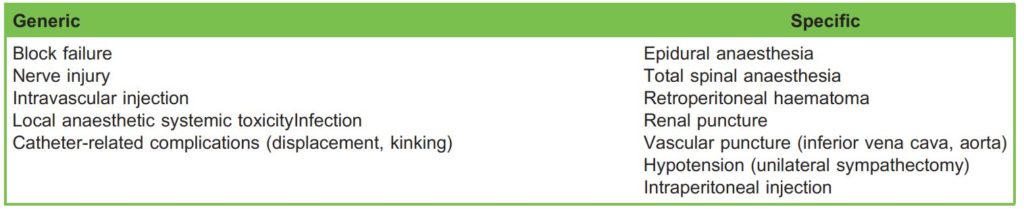
Table 3. Generic and Specific Complications
PERFORMING A LP BLOCK
Antithrombotic or Thrombolytic Therapy
The American Society of Regional Anesthesia, the European Society of Anesthesiology, and the Association of Anaesthetists of Great Britain and Ireland consider the LP block to be a ‘deep plexus block’, and recommend that guidelines for central neuraxial blocks be followed.11
Equipment
- Standard monitors (pulse oximeter, electrocardiogram, blood pressure)
- Skin antiseptic, preferably chlorhexidine and alcohol-based solutions
- Sterile gloves, gown, mask, drapes, ultrasound probe cover, ultrasound conductance jelly
- Ultrasound machine with 2-6MHz curvilinear transducer (allows improved depth penetration). In smaller children and infants where the LP is more superficial, consider using linear array transducer.
- Echogenically enhanced, nerve-stimulating Touhy needle (5 or 10 cm, 20 or 22 gauge depending on patient body habitus)
- Peripheral nerve stimulator
- Resuscitation equipment including 20% lipid emulsion. Providers must be familiar with emergency management of local anaesthetic systemic toxicity guidelines.12
Dosing
This block relies upon spread of local anaesthetic within the psoas compartment and requires a bolus volume of 0.3 to 0.5 ml/kg. Given this relatively large volume, dilute local anaesthetic such as 0.2% ropivacaine or 0.25% bupivacaine is typically used in paediatric patients. It is imperative that the maximum allowable safe dose of local anaesthetic is calculated and not exceeded. See Table 4 for recommendations on catheter infusion rates.

Table 4. Dosing Recommendations for Continuous Local Anaesthetic Infusions
Preparation
- Obtain informed consent, ensure intravenous access, apply patient monitoring.13
- A skilled assistant should be available (for example, to help adjust ultrasound and peripheral nerve stimulator settings).
- Confirm no contraindications.
- Avoid administration of long-acting neuromuscular blockade prior to block performance because peripheral nerve stimulation will be used during LP block insertion.
- ‘Stop before you block’ and perform a block safety checklist. This is essential to confirm correct patient, allergies, and surgical procedure, including side and block being performed to minimise risk of wrong block and/or wrong side.14
Patient Positioning
Due to limited cooperation and anxiety in children, LP blocks are usually performed under general anaesthesia. Prospective multicentre data from the Paediatric Regional Anaesthesia Network demonstrated no permanent neurological deficits when performing regional anaesthesia under general anaesthesia, and this should be considered as safe as when performing a block in an awake child or adult.15
The patient should be placed in the lateral decubitus position with operative side uppermost, and hips and knees flexed (Figure 6). This allows optimal visualisation of the quadriceps muscle contraction when using peripheral nerve stimulation.
To optimise sonographic visualisation, place a pillow between the lower extremities to align the pelvis and spine. When performing the Shamrock method, place a gel support underneath the dependent flank to open the space between the nondependent 12th rib and iliac crest (Figure 6).

Figure 6. Patient positioning for Shamrock approach using soft flank and axillary support. Parent permission obtained for use of image.
Operator ergonomics should be optimised such that the ultrasound machine is aligned with the operator’s line of vision, on the opposite side of the patient. Ensure that the bed height is appropriate for the operator.
Performing the Block
To perform an LP block, local anaesthetic is injected into the psoas compartment. The local anaesthetic spreads around the LP branches and cephalad to the nerve roots, providing blockade in the femoral nerve, lateral cutaneous nerve of the thigh, and obturator nerve distributions.
Several ultrasound techniques have been described to perform the LP block in children. The most commonly described techniques include the paramedian transverse oblique (PMTO) method, Trident method, and Shamrock method. These 3 methods are performed in the lateral decubitus position. There are also novel descriptions of techniques that are performed in the supine position. However, these novel techniques are less widely performed, have been found to be challenging due to difficulties obtaining optimal anatomical and needle sonographic visualisation, and may have an increased risk of renal injury. Their detailed description is beyond the scope of this tutorial.16,17
Compared to the PMTO and Trident method, the Shamrock approach allows for the most easily identifiable sonographic landmark and has the most easily identifiable external surface anatomy landmarks to guide ultrasound transducer positioning and needle insertion.18 A randomised controlled trial comparing the Shamrock method versus the Trident method concluded that the Shamrock method is faster to perform and requires fewer needle insertions with concomitant reductions in bleeding risk.19 To our knowledge, there are no other published studies comparing the different approaches to performing the LP block. While all 3 techniques are described below, the Shamrock method is recommended and described in the greatest detail.
Paramedian Transverse Oblique Method
- Probe position: The transducer is positioned in a transverse orientation over the L3-L4 spinous processes, and then is moved laterally to the paravertebral region until the articular and transverse processes are visualised (Figure 7A).
- Needle visualisation: In-plane.
- Needle direction: Ultrasound beam is directed through the lumbar intertransverse space at the level of the articular processes, or between the transverse processes of L3 and L4 (Figure 7B, C).20
- Disadvantages: Obtaining in-plane visualisation of the needle may be challenging due to the steep angle of the needle relative to the transducer. This steep angle causes high sonographic reflective losses, reducing the image quality. Furthermore, if the needle is directed lateral-to-medial towards the neural foramina, it increases the risk of epidural spread.18
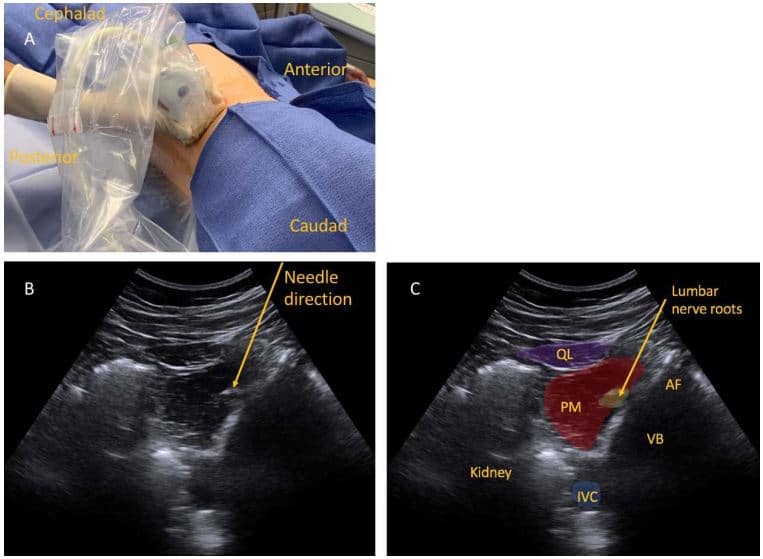
Figure 7. Paramedian transverse oblique approach to ultrasound-guided lumbar plexus block. (A) Transducer position. (B) Sonographic image demonstrating needle direction. (C) Sonographic image. AF indicates articular facet; VB, vertebral body; PM, psoas muscle; QL, quadratus lumborum muscle; IVC, inferior vena cava. Parent permission obtained for use of images.
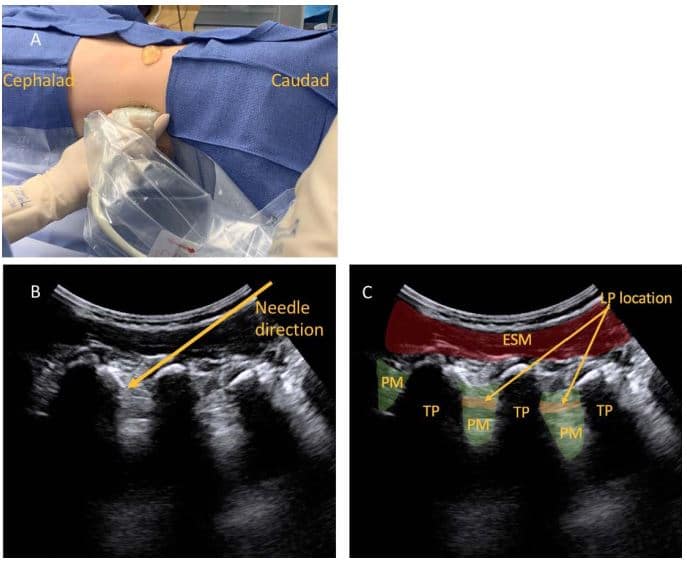
Figure 8. Trident approach to ultrasound-guided lumbar plexus block. (A) Transducer position. (B) Sonographic image demonstrating needle direction. (C) Sonographic image. TP indicates transverse process; PM, psoas muscle; LP, lumbar plexus; ESM, erector spinae muscle. Parent permission obtained for use of images.
Trident Method
- Probe position: The transducer is positioned in a sagittal orientation in the paravertebral lumbar region at the L3-L4 level (Figure 8A).
- Needle visualisation: In-plane.
- Needle direction: The needle is inserted between the transverse processes of L3 and L4 to the posterior part of the psoas muscle (Figure 8B, C). The L2, L3, and L4 transverse processes are visualised as the ‘trident sign’.21
- Disadvantages: Similar to the PMTO method, the needle requires a steep insertion angle which may reduce its visibility on sonography. This approach does not allow visualisation of nearby major vessels or kidney during needle insertion.
Shamrock Method
The Shamrock method was first described in 2013 by Sauter.22 Obtaining optimal needle visibility is less challenging as the needle is inserted in-plane, in a posterior-anterior direction, parallel with the footprint of the transducer. The risk of epidural spread is minimised, as the needle tip is directed away from the neural foramina.
To perform the block, take the following steps:
- Clean lumbar region using skin antiseptic and place sterile drapes.
- Place the transducer in transverse orientation in the midaxillary line, immediately above the iliac crest (Figure 9A).
- Using ultrasound, visualise the key anatomical structures including the transverse process, vertebral body, and psoas muscle. The lumbar plexus may be seen in the posterior aspect of the psoas muscle (Figure 9B, C).
- Insert the needle perpendicular to the skin at the same depth measured on the ultrasound screen, from the footprint of the transducer to the level of the psoas muscle (or alternatively, measure from the spinous processes or vertebral body to the psoas muscle).
- Using an in-plane technique, advance the needle while maintaining visualisation of the needle tip.
- As the needle is advanced, use a nerve stimulator with current of 1 mA. Correct needle placement within the psoas muscle is confirmed by quadriceps contraction at <0.6 mA. No motor manifestations should be elicited at <0.3 mA as this indicates intraneural needle placement.
- A test dose containing 0.5 μg/kg epinephrine may be used to assist in identifying intravascular needle placement; however, false-negative results may occur.23 Local anaesthesia should be injected slowly, with repeated aspiration, to minimise the risk of inadvertent intravascular injection.
- Spread of local anaesthetic should be visualised under ultrasound as it is injected. If spread is not seen, consider possible intravascular injection.
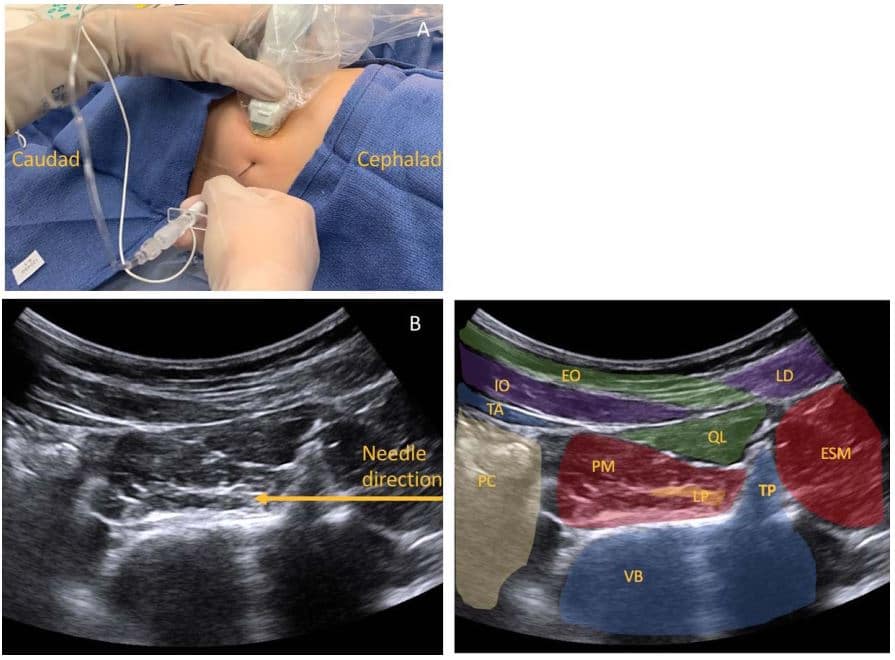
Figure 9. Shamrock approach to ultrasound guided lumbar plexus block in 5-year-old. (A) Transducer position and direction of needle insertion. (B) Sonographic image demonstrating needle direction. (C) Sonographic image. TP indicates transverse process; VB, vertebral body; PM, psoas muscle; LP, lumbar plexus; ESM, erector spinae muscle; QL, quadratus lumborum muscle; PC, peritoneal cavity; TA, transverse abdominis muscle; IO, internal oblique muscle; EO, external oblique muscle; LD, latissimus dorsi muscle. Parent permission obtained for use of images.
Tips for Performing the Shamrock Method
- Use a needle with enhanced echogenicity to aid needle-tip visualisation.
- Estimate the depth of the LP from the site of needle insertion: Identify a line passing through the posterior superior iliac spine (PSIS), parallel to the spine. Identify the intercristal line. Then identify the intersection between the intercristal line and the line from the PSIS. The distance between the PSIS and the intersection between the PSIS line and intercristal line correlates closely with the depth of the lumbar plexus in children. This knowledge may help reduce the risk of the needle being inserted too deep, and also guides needle length selection (Figure 10).24
- If bone (transverse process) is contacted, withdraw the needle and redirect caudally to walk off the bone.
- Some operators prefer to keep the transverse process in view, especially if imaging is poor, and deliberately advance the needle until bone is contacted; at this point, the needle can be withdrawn slightly, redirected either cranially or caudally, and advanced into the psoas muscle. The redirected needle can easily be revisualized by simply tilting the ultrasound in the opposite direction (ie cranial probe tilt for caudal needle redirection).
- If stimulation is obtained with a nerve stimulator current of <0.3 mA, withdraw the needle slightly as this may indicate intraneural or dural sleeve injection, with risk of epidural or intrathecal spread.
- Two-dimensional and colour Doppler can help to identify arterial and venous vasculature. Hydro-dissection with normal saline (0.9% NaCl) may help determine needle tip location, especially when anatomy is challenging.
- If the operator finds the sonographic anatomy challenging and the needle position is unclear, the block should be aborted.
- Avoid forceful injection of local anaesthetic and consider using an in-line injection pressure monitor if available. Injection of local anaesthetic with pressures >138 kPa (20 psi) have been associated with an increased risk of epidural spread and bilateral blockade.25
- Nerve stimulation in combination with ultrasound guidance is recommended as the LP nerve roots may be difficult to visualise (Table 5).
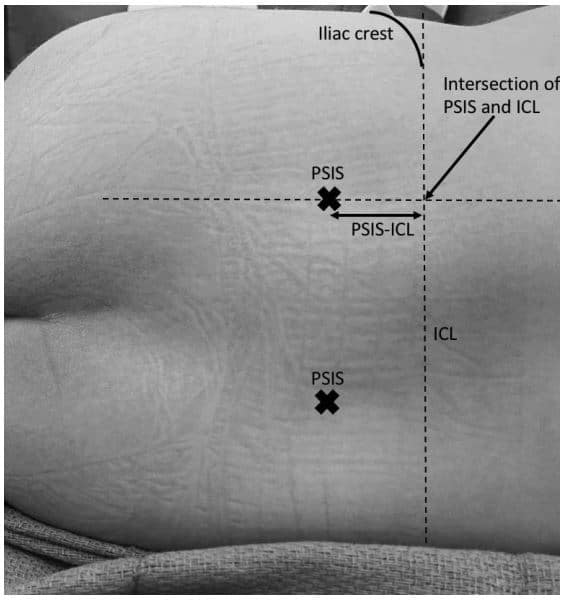
Figure 10. Surface landmarks to estimate depth of needle insertion. PSIS indicates posterior superior iliac spine; ICL, intercristal line; PSISICL, distance between PSIS and the intersection of the line passing through the PSIS and the ICL. Parent permission obtained for use of image.
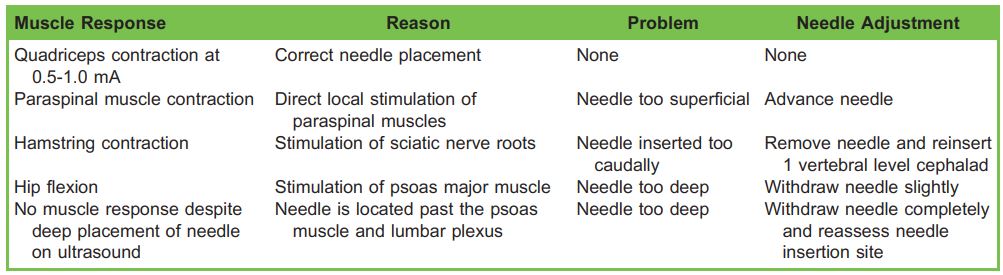
Table 5. Recommendations When Inappropriate Muscle Responses Occur25
Continuous LP Catheter Infusions
The lumbar area is an ideal location for catheter placement for continuous perioperative analgesia. LP catheters should be considered for periacetabular osteotomies, open reduction internal fixation of the hip, femoral osteotomies, and above-knee amputations. Following induction of anaesthesia, the catheter can be placed prior to surgical incision as it is distant from the surgical incision site and can potentially reduce systemic opioid requirements. Care must be taken with dressing the catheter so that it is does not contaminate the surgical field or risk becoming adherent to the surgical drapes.
Method for Insertion
- Use strict aseptic technique.
- Insert the Touhy needle using the same method as for the single-shot technique described above.
- Thread the catheter approximately 3 cm beyond the tip of the needle into the psoas compartment. Hydro-dissection using normal saline may assist in threading the catheter more easily.
- The catheter will feel more difficult to advance than an epidural catheter; an unusually smooth catheter insertion suggests intravascular placement.
- Correct catheter placement may be confirmed by sonographic visualisation of spread of local anaesthetic or normal saline in the psoas compartment.
- Secure the catheter using adhesive skin glue (for example, Dermabond®), securing device and an adhesive dressing.
- Label catheter as a ‘nerve catheter’ to avoid medication administration errors.
Alternatively, the Tsui catheter needles may be used, where the catheter is situated over the needle and does not need to be advanced beyond the tip of the needle. However, the hub and tubing attachment for this catheter is considerably bulky, and this may cause a pressure area when it is secured on the patient’s back in the lumbar region.
For infants less than 6 months old, it is recommended to use chloroprocaine for continuous infusions. Infants metabolise amide local anaesthetics at a slower rate and are at greater risk of amide local anaesthetic toxicity. Ester local anaesthetics, such as chloroprocaine, are metabolised in the plasma via pseudocholinesterase and are less likely to cause local anaesthetic systemic toxicity.
LP nerve catheters can safely remain in situ for up to 3 days; beyond this, the risk of infection is increased.27
SUMMARY
- The ultrasound-guided LP block allows identification of major anatomical structures, including the transverse process, psoas muscle, kidney, and major blood vessels. It also allows visualisation of needle tip, guiding the site and direction of insertion.
- Compared to other methods, the Shamrock method is the least challenging approach to obtain high-quality visualisation of the needle and major anatomical structures.
- A combined technique utilising both ultrasound and peripheral nerve stimulator guidance is the safest approach to avoid inadvertent intraneural injection.
- The LP block requires expert skills due to the potential for inadvertent vascular or renal injury, epidural spread, and local anaesthetic systemic toxicity.
- LP continuous catheter infusions allow prolonged duration of analgesia and reduce the requirement for systemic opioid administration.
REFERENCES
- Farag E, Mournir-Soliman L, Brown DL. Brown’s Atlas of Regional Anesthesia. 5th ed. Philadelphia, PA: Elsevier; 2017.
- Touray ST, Leeuw MA, Zuurmond WWA, et al. Psoas compartment block for lower extremity surgery: a meta-analysis. Br J Anaesth. 2008;101(6):750-760.
- Boretsky K, Hernandez MA, Eastburn E et al. Ultrasound-guided lumbar plexus block in children and adolescents using a transverse lumbar paravertebral sonogram: initial experience. Pediatr Anesth. 2018;28:291-295.
- Aveline C, Bonnet F. Delayed retroperitoneal haematoma after failed lumbar plexus block. Br J Anaesth. 2004;93:589-591.
- Aida S, Takahashi H, Shimoji K. Renal subcapsular hematoma after lumbar plexus block. Anesthesiology. 1996;84:452-455.
- Karmakar MK. Considerations for ultrasound guided lumbar plexus block. Accessed May 11, 2020. https://www.nysora.com/regional-anesthesia-for-specific-surgical-procedures/lower-extremity-regional-anesthesia-for-specific-surgical-procedures/anesthesia-and-analgesia-for-hip-procedures/lumbar-paravertebral-sonography-considerations-ultrasound-guidedlumbar-plexus-block/.
- Drake RL, Vogl AW, Mitchell AWM. Gray’s Basic Anatomy. 2nd ed. Philadelphia, PA: Elsevier; 2018.
- Gray’s Anatomy of the Human Body. 20th ed. [Public domain]. Accessed 11 May 2020. https://commons.wikimedia.org/wiki/File:Gray822.png
- Kirchmair L, Enna B, Mitterschiffthaler. Lumbar plexus in children: a songraphic study and its relevance to pediatric regional anesthesia. Anesthesiology. 2004;101:445-450.
- Omar AM, Mansour MA, Kamal AS. Psoas compartment block for acute postoperative pain management after hip surgery in paediatrics: a comparative study with caudal analgesia. Reg Anesth Pain Med. 2011;36:121-124.
- Horlocker TT, Vandermeuelen E, Kopp SL. American Society of Regional Anaesthesia and Pain Medicine evidencebased guidelines: regional anesthesia in the patient receiving antithrombotic or thrombolytic therapy. Reg Anesth Pain Med. 2018;43:263-309.
- American Society of Regional Anesthesia and Pain Medicine. Checklist for treatment of local anesthetic systemic toxicity. Accessed May 11, 2020. https://www.asra.com/content/documents/asra_last_checklist_2018.pdf.
- American Society of Anesthesiologists. Standards for basic anesthetic monitoring. Accessed May 11, 2020. https://www.asahq.org/standards-and-guidelines/standards-for-basic-anesthetic-monitoring.
- Royal College of Anaesthetists. Wrong site block. Accessed May 11, 2020. https://www.ra-uk.org/index.php/stop-beforeyou-block.
- Walker BJ, Long JB, Sathyamoorthy M, et al. Complications in pediatric regional anesthesia: an analysis of more than 100, 0000 blocks from the Pediatric Regional Anesthesia Network. Anesthesiology. 2018;129:721-732.
- Sato M, Hara M, Uchida O. An antero-lateral approach to ultrasound-guided lumbar plexus block in supine position combined with quadratus lumborum block using single-needle insertion of pediatric hip surgery. Pediatr Anesth. 2017;27:1064-1065.
- Liu Y, Ke X, Wu X, et al. Ultrasound-guided lumbar plexus block in supine position. Anesthesiology. 2018;128(4):812.
- Neilsen MV, Bendtsen TF, Borglum J. Superiority of ultrasound-guided Shamrock lumbar plexus block. Minerva Anestesiol. 2018;84:115-121.
- Strid JMC, Sauter AR, Ullensvange K, et al. Ultrasound-guided lumbar plexus block in volunteers; a randomised controlled trial. Br J Anaesth. 2017;118:430-438.
- Kirchmair L, Entner T, Wissel J et al. A study of the paravertebral anatomy for ultrasound-guided posterior lumbar plexus block. Anesth Analg. 2001;93:477-481.
- Karmakar MK, HoAM, Li X, et al. Ultrasound-guided lumbar plexus block through the acoustic window of the lumbar ultrasound trident. Br J Anaesth. 2008;100:533-537.
- Sauter AR. The ‘‘Shamrock Method’’ a new and promising technique for ultrasound guided lumbar plexus block. Br J Anaesth. 2013:111 (eLetters supplement).
- Ivani G, Suresh S, Ecoffey C. The European Society of Regional Anaesthesia and Pain Therapy and the American Society of Regional Anesthesia and Pain Medicine Joint Committee practice advisory on controversial topics in pediatric regional anesthesia. Reg Anesth Pain Med. 2015;40(5)
- Walker BJ, Flack SH, Bosenberg AT. Predicting lumbar plexus depth in children and adolescents. Anesth Analg. 2011;112(3):661-665.
- Gadson JC, Lindenmuth DM, Hadzic A, et al. Lumbar plexus block using high-pressure injection leads to contralateral and epidural spread. Anesthesiology 2008;109:683-688.
- Vloka JD, Tsai T, Hadzic. Lumbar plexus block—landmarks and nerve stimulator technique. Accessed September 9, 2020. https://www.nysora.com/regional-anesthesia-for-specific-surgical-procedures/lower-extremity-regional-anesthesiafor-specific-surgical-procedures/lumbar-plexus-block/.
- Walker BJ, Long JB, De Oliviera GS, et al. Peripheral nerve catheters in children: an analysis of safety and practice patterns from the pediatric regional anesthesia network (PRAN). Br J Anaesth. 2015;115 (3):457-462.
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/