Regional Anaesthesia

KEY POINTS
- We recommend marking the skin with an indelible marker prior to commencing any ultrasound-based anatomical survey.
- Knowing your needle tip location is essential at all times to avoid inadvertent pleural puncture or entry into the intervertebral foramen.
- In all ultrasound-guided paravertebral block techniques, an indication of correct needle tip placement is the anterior displacement of the parietal pleura when the solution of local anaesthetic is being injected.
- Hydrolocation with saline can be used to help with needle tip position; this is particularly useful when the anatomy on ultrasound is challenging.
INTRODUCTION
Paravertebral blockade (PVB) aims to result in ipsilateral somatosensory and sympathetic nerve block at multiple vertebral levels. First described by Sellheim in 1905, it was used for a wide variety of indications, particularly thoracoplasty and lobe resections for tuberculosis, but then fell out of favour by the 1950s and 1960s. It was ‘‘rediscovered’’ in 1979 by Eason and Wyatt and now PVBs are widely used in both the paediatric and adult populations.
Traditional PVB uses a landmark and/or loss-of-resistance technique. However, modifications such as nerve stimulator guidance and ultrasound (US) guidance have been described. US has a number of advantages, such as enabling sonographic measurements to be made, visualization of pleura and lung tissue, and visualization of the needle and of perineural catheter placement in real time. Heightened interest in PVB is also due to current evidence of the possible beneficial role PVB may play in cancer recurrence.
Skill Level Required: Advanced
ANATOMY
The paravertebral space is within the extrapleural space. Extending from thoracic levels 1 to 12, it is a wedge-shaped potential compartment bordering the vertebral bodies bilaterally.
Boundaries of the Paravertebral Space
Anterolateral: Parietal pleura
Posterior: Superior costo-transverse ligament
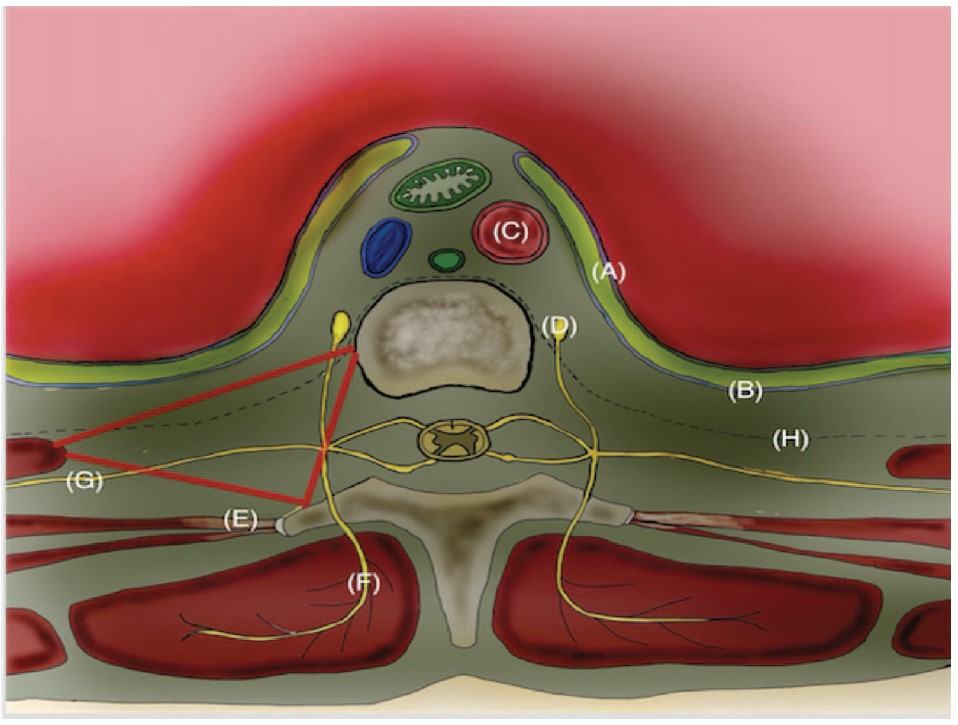
Figure 1. Illustrated cross section of paravertebral space (red triangle) at thoracic level. A, visceral pleura; B, parietal pleura; C, aorta; D, sympathetic chain; E, internal intercostal ligament, continuous with costo-transverse ligament medially; F, posterior division of intercostal nerve; G, intercostal nerve; H, endothoracic fascia.
Medial: Vertebrae, intervertebral disc, and intervertebral foraminae
Superior: Inferior aspect of head of rib
Inferior: Superior aspect of head of rib
The paravertebral space itself has the endothoracic fascia that further divides it into an anterior and a posterior compartment (Figure 1).
For further detail, please refer to ATOTW Tutorial 224, ‘‘Thoracic Paravertebral Block: Landmark Techniques.’’
INDICATIONS AND CONTRAINDICATIONS TO US-PVB
Indications
PVB results in ipsilateral somatic and sympathetic nerve blockade. It can be considered for a variety of surgical procedures in conjunction with general anaesthesia. It is also used, but less commonly, as a sole anaesthetic technique. While it is more widely applied in providing unilateral effective intraoperative and postoperative analgesia for breast surgery and thoracic surgery, it can also be used to provide analgesia for nonsurgical pain management (such as rib fractures). For a summary of indications for PVB, see Table 1.
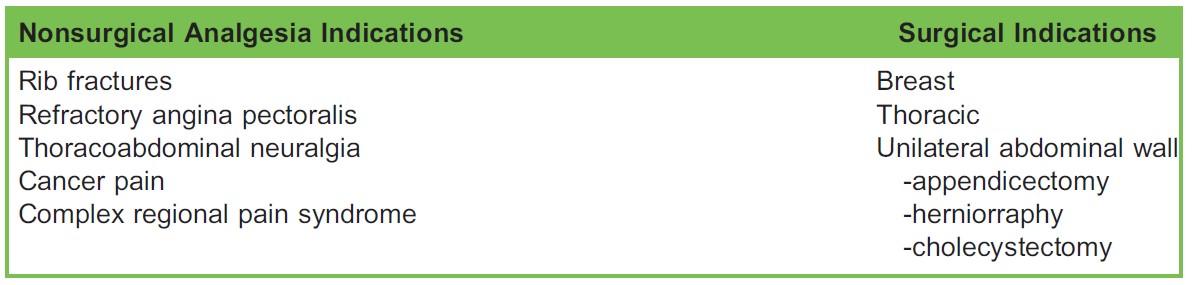
Table 1. Indications for Paravertebral Blockade (Note: The list is not exhaustive)
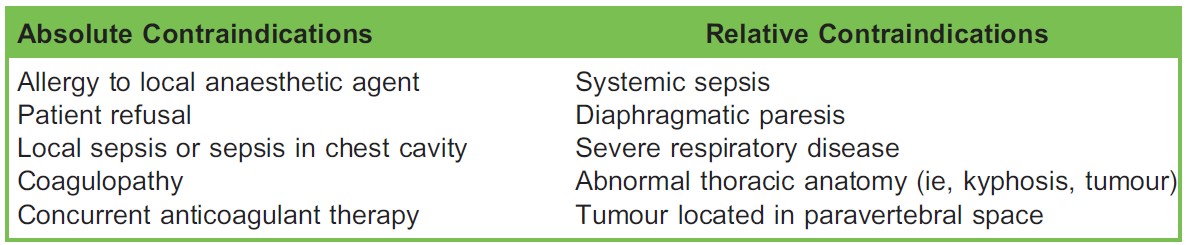
Table 2. Contraindications to Paravertebral Blockade
Contraindications
Prior to performing any regional anaesthesia technique, indications and contraindications need to be addressed for each patient. For PVBs, contraindications to their use are similar to those for neuraxial blockade. Table 2 shows absolute and relative contraindications to PVB.
COMPLICATIONS
US guidance has the potential of increasing safety for PVBs compared to traditional landmark technique. There are limited data on US-based complications. In a retrospective study at Massachusetts General Hospital over a 4-year period of US-guided thoracic PVB in breast surgery, 6 complications were documented in over 1400 blocks performed. These included bradycardia with hypotension, a vasovagal episode, and possible local anaesthetic toxicity but no incidence of accidental pleural puncture or pneumothorax.1 See Table 3 for general and specific complications of PVB.
Bilateral PVB
The use of bilateral PVBs instead of epidural anaesthesia can be considered. Less profound sympathectomy is seen with bilaterally placed PVBs compared to an epidural and this could potentially lead to less cardiovascular instability. In a study with thoracotomy patients, bilateral continuous thoracic PVB provided similar pain control in addition to reduced colloid and vasopressor support when compared to patients receiving an epidural. 2
However, using bilateral blocks is shown to increase the risk of complications when compared to a unilateral PVB. The risk of a pneumothorax and pleural puncture increases from 0.4% to 3% while vascular puncture risk increases from 5% to 9% in landmark-based blocks. 3
CLINICAL EFFICACY AND SENSORY DISTRIBUTION
The landmark technique for adult PVB has demonstrated a failure rate of 10.7%,4 whereas nerve stimulator techniques show a 6.1% failure rate. 3 For US-guided PVB, the failure rates have been rarely reported. One study reported a failure rate of 3.5%; however, the sample size was small, with only 22 patients.5 Table 4 summarises the clinical studies which investigated clinical efficacy and sensory distribution of US-guided PVB.
PREPARATION
Basic preparation as for any regional anaesthesia is mandatory. This includes obtaining patient informed consent, having a skilled assistant available, applying continuous vital monitoring (blood pressure, ECG, and SpO2), establishing intravenous access, and confirming that emergency medication and equipment are readily available. A ‘‘Stop Before You Block’’ timeout should be carried out just before the block is started.
This topic is covered in more detail in ATOTW Tutorial 134, ‘‘Peripheral Nerve Blocks—Getting Started.’’
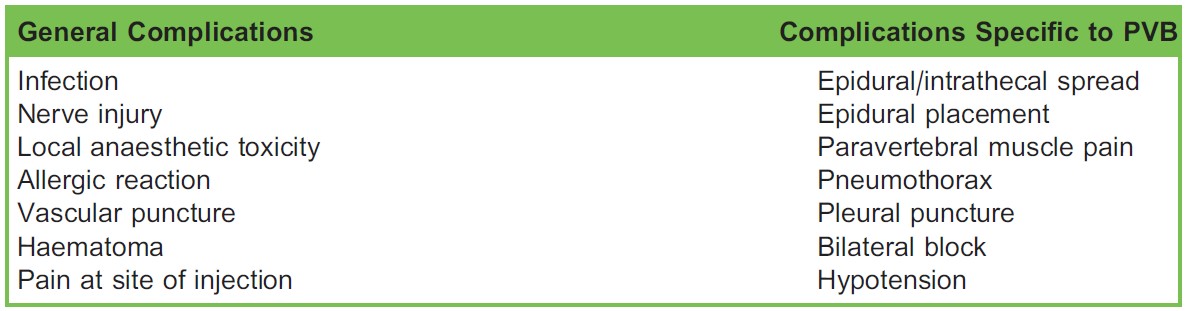
Table 3. Complications of Paravertebral Blockade (PVB)

Table 4. Clinical Studies Assessing Clinical Efficacy of Ultrasound-Guided Paravertebral Blockade
Specific Equipment Required
- High-frequency (10-12 MHz) linear or curvilinear US transducer
- An 18-gauge echogenic Tuohy needle
- A 10-mL syringe plus 25-gauge needle with short-acting local anaesthetic for skin infiltration
- High-volume long-acting local anaesthetic solution (15-20 mL) for injecting into paravertebral space.
Echogenic Needles
There is significant deterioration in needle visibility with steep needle angles due to limitations in US physics. The steeper the angle of insonation, the higher the sonographic reflective losses that occur, leading to reduced quality of needle visualized. This limiting factor in US blocks has resulted in echogenic needles being introduced into anaesthetic practice. A myriad of needleenhancing techniques have been employed ranging from scoring, dimpling, and polymer coating of the needle, all aimed at improving needle acoustics at deeper tissue angles.
In PVB using US, visualization of peripheral nerve needle is a distinct problem due to the steep nature of the needle trajectory required to perform the block. Manipulation of the needle within tissue and, more importantly, visualization of the needle tip is challenging. The introduction of echogenic needles has proven beneficial in visualizing the needle during deep-angled regional blocks, in particular, PVB.
Choice of Local Anaesthetic
Choice of local anaesthetic used should be based on the duration of anaesthesia or analgesia required from the blockade.
Nerve fascicles in the paravertebral space are minimally covered, having lost any dural cuff before exiting the intervertebral foramina, and not having formed a robust outer epineurium around each fascicle as they are formed more distally. This makes nerves in the paravertebral space very susceptible to local anaesthetics.
Table 5 lists the different durations of commonly used local anaesthetics.
Positioning
Position the patient as you would for neuraxial anaesthesia. In compliant patients, it is common to perform this block with the patient in the sitting position while arching their back. Another commonly used position is to place the patient in the lateral ‘‘foetal’’ position with the side to be blocked uppermost.

Table 5. Commonly Used Local Anaesthesia for Paravertebral Blockade with Characteristics of Onset and Anaesthesia and Analgesia Duration. Reproduced with permission from New York School of Regional Anaesthesia (NYSORA)
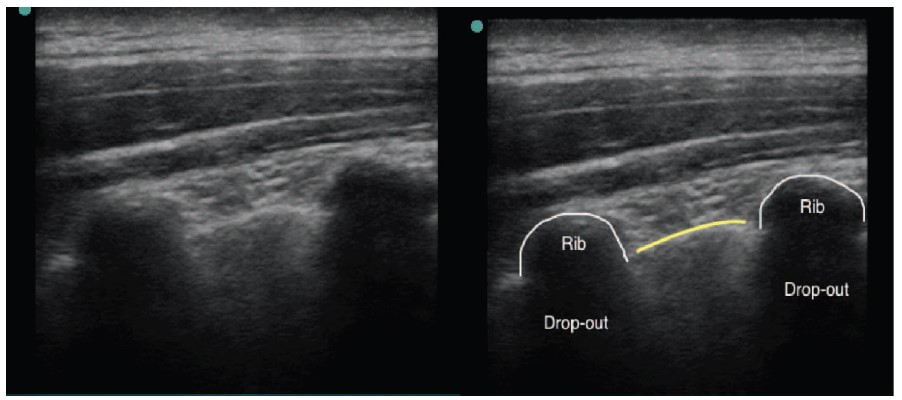
Figure 2. (Left) Basic ultrasound (US) appearance of bone and pleura. (Right) Structures are outlined. Longitudinal axis of US probe. Yellow line demonstrates parietal pleura.
Choosing the Level
The level chosen depends on the dermatomal spread required for blockade. Communication between paravertebral spaces in the cervical and thoracic areas exists and injecting a volume of local anaesthetic should lead to spread of injectate to adjacent levels along the paravertebral space. However, injectate spread is highly variable, it can lead to longitudinal (which is ideal), lateral, or cloud-shaped spread in the thoracic paravertebral space. 6 Although there is no constant relationship between the volume of local anaesthetic injected and the subsequent paravertebral spread, a generally accepted guide is that a largevolume single shot (such as 20 mL of local anaesthetic) PVB will provide dermatomal spread to 4-5 levels. Local anaesthetic spreads in both in the caudad and cephalad directions. Thus, a PVB placed at a mid-dermatomal level with reference to the surgical site should suffice for most surgical procedures where PVB is indicated. As an example, in simple mastectomy, a single-shot block at thoracic level 3 or 4 would be considered appropriate for the dermatomal spread required for the surgery.
When greater dermatomal spread is desired, the use of multilevel PVB injections is very effective. An example is in mastectomy surgery in conjunction with latissimus dorsi flap reconstruction. For greater dermatomal spread, a 2-level PVB can be done for this surgery—the first block at T3-4 level and a second block at T7 level. Of note, PVB spread at the lumbar region compared to the thoracic region is even less predictable.
US Scanning and Needle Approaches
There are 2 commonly performed approaches—the ‘‘US-assisted’’ PVB and the ‘‘US- guided’’ PVB.
US-assisted PVB refers to the initial use of US to identify specific anatomical landmarks (ie, vertebral column, transverse processes, pleura) and then performing a PVB without the continuous use of the US.
US-guided PVB implies that the operator performs a PVB with continuous real-time US visualization throughout the entire procedure. This requires a higher level of expertise in US handling and needling under US guidance.
US scanning is never a static process. Dynamic scanning of the anatomy (anatomical surveying) to identify structures is essential to plan a safe and successful approach to any nerve block. Additionally, US-guided PVB provides information on needle position and spread of local anaesthetic within the visualized field, and is also helpful to confirm absence of pneumothorax after a block is performed.
Basic Ultrasound Appearance of Key Structures
Bone appears as a hyperechoic line with acoustic shadowing below (also known as dropout). Ribs will appear as more convex structures compared to transverse processes, which will appear more squared off and lie more superficial to skin compared to ribs (step-up on sonographic image).
Pleura appear as a bright hyperechoic line. Visual echogenicity of pleura can be accentuated by asking the patient to breathe deeply. There is no acoustic shadowing seen with pleura (Figure 2).
PROCEDURE
It is important to first identify key surface landmarks to aid in establishing the relevant spinal level. While carrying out US scanning, it is often easy to drift away from the initially intended level to carry out the block; therefore a visual aid on the patient’s skin is advisable. We advise that prior to commencing any US-based anatomical survey, relevant skin markings should be made with an indelible marker. Key landmarks to identify include the following:
- The most prominent cervical spinous process, C7
- Spine of scapula, which corresponds to the T3 vertebral level
- Lower tips of scapulae (inferior angle of scapula) which corresponds to the T7 vertebral level.
If carrying out a lumbar PVB, identify the iliac crest bilaterally (Tuffiers line), which corresponds to the L4 vertebral body. These provide a form of visual aid to the operator while US scanning is performed to locate a suitable location for the block.
The authors use intravenous sedation and opioid analgesia for carrying PVB as it is quite an uncomfortable block for the awake patient. If there are no contraindications, we generally titrate to effect using intravenous midazolam (2-4 mg) and intravenous fentanyl (25-50 µg).
Technique
There are numerous descriptions for US probe orientation regarding alignment and angulation. For needle visualization, either an in-plane (full length of needle visualized) or out-of-plane (cross section of the needle only visualized) approach is used. We will describe the more common approaches used in PVB in this tutorial.
US approaches to PVB comprise the longitudinal view and the transverse view.
In the in-plane techniques, the authors advocate visualization of the needle tip at all times throughout the procedure, though this can be very challenging when the target structures are deep. Intermittent injection using a small volume of saline can be used to aid needle location within the difficult US image, a technique called ‘‘hydrolocation’’; however, the authors do stress to the reader that in most circumstances PVB is carried out as an adjunct to multimodal analgesia. If the operator finds the anatomy on US very challenging and needle position is questionable, the block should not be carried out. The risk of pneumothorax is real.
We will describe 3 techniques.
1) Longitudinal oblique, in-plane technique
Probe orientation: Longitudinal oblique
US needle visualization:In plane
Place the US probe in a caudocranial orientation about 5 cm from midline at the level where anaesthesia/analgesia is to be achieved. At this point identify the ribs on sonography. Next identify the pleura deep to the ribs. Deep to pleura, the pulmonary tissue is not seen due to its air content.
Continuing to manoeuvre the probe medially, look for the transition of ribs to transverse processes marked by a change in shape and a slight step-up of bony image. At this point there are 2 alternatives to improving the ability to needle the space:
- Slide the transducer cranially, such that the targeted paravertebral space lies towards one side of the US screen (the caudad edge of the screen; Figure 3). This produces a steep needle insertion angle, but avoids the double-fulcrum effect of the lower transverse process (as seen in US image in Figure 5)
- Rotate the probe slightly anticlockwise while fixing the cranial (uppermost) end of the probe so it acts as a fulcrum (fixed point). This will result in the cranial end of the probe remaining medially (same original location) and the caudal end of the probe will now be located more laterally. The image acquired will have the transverse process located superiorly and an image of lower rib located inferiorly on the screen (Figure 4). The probe is then tilted slightly laterally (outwards)—this ‘‘sharpens’’ the bony image.
The advantage of this technique is that by stepping out the lower edge of the transducer, an oblique cut is made and results in both a transverse process and a rib being in the same sonographic image. The image obtained, with the transverse process superiorly and rib inferiorly, allows a more superficial needle trajectory to reach the paravertebral space. This allows improved needle visibility, whilst maintaining a more familiar target position.
Needle placement is in a caudocradial direction in line with the US probe orientation. The main challenge with in-plane needling technique is to maintain constant visualization of the needle path. Once the costotransverse ligament is breached (a ‘‘pop’’ or ‘‘crunch’’ may be felt), the needle tip should lie in the thoracic paravertebral space. Confirm negative vessel or lung tissue breach via aspiration, then proceed with local anaesthetic delivery slowly in aliquots. The local anaesthetic is delivered slowly in 5-mL aliquots followed by repeated aspiration and injection of local anaesthesia to reduce the risk of intravascular administration. The injectate will be seen to ‘‘push’’ the highly echogenic pleura downwards (away from your needle). Commonly during injection, patients will report a heaviness or uncomfortable pressure sensation in the chest.
2) Longitudinal, out-of-plane technique
Probe orientation: Longitudinal oblique

Figure 3. (Left) Longitudinal orientation of the probe, with the chosen paravertebral space at the caudad end of the ultrasound (US) screen (in this example, this is on the right-hand side of the U.S. image provided).(Right) Red arrow indicates orientation of US needle. TP, transverse process.
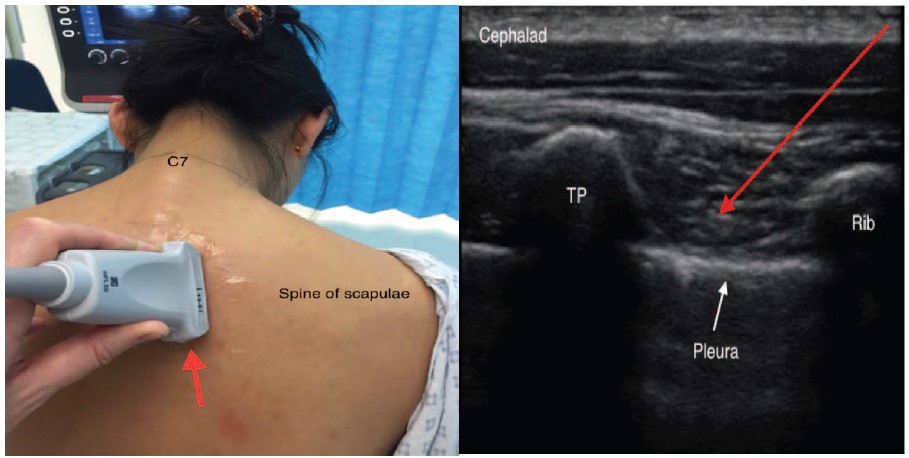
Figure 4. Longitudinal oblique probe orientation. Red arrow indicates orientation of peripheral needle. TP, transverse process. Note that rib is inferior (right side of image) and is deeper than the transverse process, which is superior (left side of image), hence needle trajectory can be less steep, improving ultrasound visibility.
US needle visualization: Out-of-plane
Starting in a similar way to the technique described above, place the US probe in a sagittal orientation about 5 cm from midline at the level where anaesthesia/analgesia is to be achieved. Identify ribs and pleura on sonography. Continuing to manoeuvre the probe medially, observe for the transition of the ribs to transverse processes (a change in shape and a slight step-up of bony image). At level of the transverse process, insert the needle from a lateral to medial direction to contact the transverse process. Once the transverse process is hit, walk the needle off the bone in a caudal direction to pierce the superior costotransverse ligament. Confirm negative vessel or pleural breach via aspiration then proceed with local anaesthetic delivery slowly as described above; the pleura will be seen to be pushed downward (Figure 5).
3) Transverse, in-plane technique
Probe alignment: Transverse or axial
US needle visualization: In-plane
Place the US probe in an axial orientation just lateral to the midline at the level where anaesthesia/analgesia is to be achieved. The aim is to obtain an image of rib identified with a hyperechoic borderline and acoustic shadowing below. From this point, manoeuvre the probe in a caudad direction to get to the intercostal space where the paravertebral space is identified. The
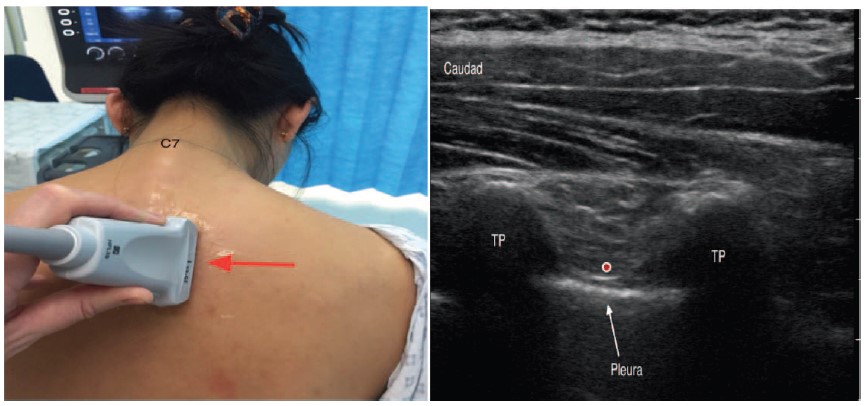
Figure 5. Longitudinal orientation of probe; out-of-plane technique. Red arrow indicates orientation of peripheral needle. Red dot indicates final needle tip position. TP, transverse process.
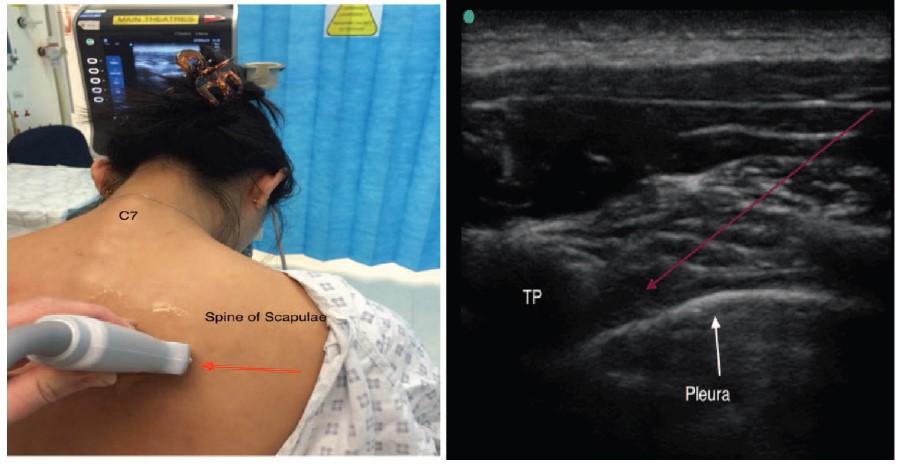
Figure 6. Transverse orientation of probe. Between adjacent ribs, pleura is visualized (no drop-out effect). Red arrow indicates orientation of peripheral needle. TP, transverse process.
paravertebral space image on US is characterized by the distinctive hyperechoic line of the pleura below and internal intercostal membrane (IIM) above. The IIM is an aponeurotic continuation of the internal intercostal muscle, which is contiguous with the superior costotransverse ligament.
Place the needle in an in-line lateral-to-medial (towards the transverse process) approach aiming to breach the IIM. Confirm negative vessel or lung tissue breach via aspiration then proceed with local anaesthetic delivery slowly in aliquots. Again the pleura will be pushed downwards during injection.
Theoretically, with this needle approach there is a higher risk of epidural spread. Cadaver studies have shown an incidence of up to 40% of epidural spread using the US-PVB transverse in-plane technique.[7] The lateral-to-medial needle direction may result in the needle positioning at the neural foramen (Figure 6).
Catheter Technique
Continuous PVB technique provides excellent extended analgesia for patients. However, the performance of perineural catheter infusions is highly reliant on the fact that the catheter is placed in the ‘‘desired’’ position. Ensuring this placement requires accurate US visualization of the catheter location and specifically the tip of the catheter where the infusion is carried out. While it is relatively easy to position the needle tip in the correct location, this does not indicate that the catheter will thread to the correct location.
The advantage of using US for PVB catheter placement is the ability to see pleural displacement while injecting via the catheter, indicating that the catheter tip has remained in the paravertebral space. Inability to see correct spread is likely to indicate that the tip has migrated, and block failure will ensue.
The catheters themselves are usually challenging to visualize with US given the angles of insertion. Echogenic perineural catheters have been designed, using various methods of diffractive surfaces to produce reflections. No formal clinical data have yet been published on these new devices, therefore the authors are unable to make any recommendation for them.
SUMMARY
- Local anaesthetic should be injected slowly in small aliquots. Avoid injecting forcefully at high pressure to reduce the risk of epidural spread.
- Aspiration for blood should always be carried out before injection of local anaesthetic solution.
- Real-time depression of pleura during local anaesthetic injection is a sign of correct placement of needle tip in the paravertebral space for single-shot block and catheter techniques.
- Echogenic needles for PVB placement may further aid needle visualization.
- Pneumothorax is a serious complication of this block.
- Patients should be reminded to inhale and exhale during your injection into the paravertebral space—breath holding during this uncomfortable procedure can lead to syncope.
REFERENCES
- Pace MM, Sharma B, Anderson-Dam J, Fleischmann K, Warren L, Stefanovich P Ultrasound-guided thoracic paravertebral blockade: a retrospective study of the incidence of complications. Anesth Analg. 2016;122(4):1186-1191.
- Pintaric TS, Potocnik I, Hadzic A, Stupnik T, Pintaric M, Novak Jankovic V. Comparison of continuous thoracic epidural with paravertebral block on perioperative analgesia and hemodynamic stability in patients having open lung surgery. Reg Anesth Pain Med. 2011;36(3):256-260.
- Naja Z, Lonnqvist PA. Somatic paravertebral nerve blockade. Incidence of failed block and complications. Anaesthesia. 2001;56(12):1184-1188.
- Lonnqvist PA, MacKenzie J, Soni AK, Conacher ID. Paravertebral blockade. Failure rate and complications. Anaesthesia. 1995;50(9):813-815.
- Uskova A, LaColla L, Albani F, Auroux AS, Chelly JE. Comparison of ultrasound-assisted and classic approaches to continuous paravertebral block for video-assisted thoracoscopic surgery: a prospective randomized trial. Int J Anesthesiol Res. 2015;3(1):9-16.
- Conacher ID. Resin injection of thoracic paravertebral spaces. Br J Anaesth. 1988;61(6):657-661.
- Cowie B, McGlade D, Ivanusic J, Barrington MJ. Ultrasound-guided thoracic paravertebral blockade: a cadaveric study. Anesth Analg. 2010;110(6):1735-1739.
- Pusch F, Wildling E, Klimscha W, Weinstabl C. Sonographic measurement of needle insertion depth in paravertebral blocks in women. Br J Anaesth. 2000;85(6):841-843.
- O Riain SC, Donnell BO, Cuffe T, Harmon DC, Fraher JP, Shorten G. Thoracic paravertebral block using real-time ultrasound guidance. Anesth Analg. 2010;110(1):248-251.
- Hara K, Sakura S, Nomura T, Saito Y. Ultrasound guided thoracic paravertebral block in breast surgery. Anaesthesia. 2009; 64(2):223-225.
- Ben-Ari A, Moreno M, Chelly JE, Bigeleisen PE. Ultrasound-guided paravertebral block using an intercostal approach. Anesth Analg. 200; 109(5):1691-1694.
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/