Regional Anaesthesia

KEY POINTS
- Day case surgery should take place through self-contained facilities with their own theatre, admission and discharge areas.
- Early information on regional anaesthetic (RA) techniques and what to expect during and after surgery decreases patient anxiety and promotes engagement in their own perioperative journey.
- Tourniquet pain may occur with any brachial plexus block, so preemptive counselling and management is essential.
- For hand and wrist surgery, clear superiority has not been demonstrated when comparing axillary, infraclavicular and supraclavicular RA techniques. However, they may not all be appropriate for an individual patient.
- An experienced team that works together regularly reduces adverse events and leads to higher success rates.
INTRODUCTION
This tutorial will describe aspects of patient, facility and staff setup for day case hand and wrist surgery while also exploring the choice of anaesthetic technique for different surgical procedures.
Day surgery is described as the practice of admission, procedure and discharge on the same calendar day.1 The scope of day surgical procedures is widening, and comorbidities such as morbid obesity or diabetes are no longer considered absolute contraindications. Although day case surgery traditionally describes planned procedures,2 semi-elective procedures following the same principles of same-day admission and discharge are now also often included.3
Upper limb surgery, in particular surgery on the hand and wrist, is an area in which day case surgery is thriving. In this setting, regional anaesthesia (RA) has been shown to offer significant benefits compared with general anaesthesia, such as reducing pain, opioid con- sumption and postoperative nausea and vomiting,4,5 as well as shorter recovery time and faster discharge following surgery.6,7
SETTING
The ideal day case surgical facility is purpose built, self-contained, with its own theatre(s), admission and discharge areas.3 A 2-stage recovery may be used so that patients not undergoing general anaesthesia or heavy sedation may bypass stage 1 and go straight to stage 2. Here, they can eat and drink, plan discharge, and participate in the early stages of postoperative care and rehabilitation. For orthopaedic or hand surgery, on-site clinic and X-ray facilities may enable efficient ongoing review of patients and booking for same-day procedures.
Self-mobilisation should be encouraged at all stages of the patient journey, including walking to the operating theatre and walking out of the ward at the end of the day, to limit inactivity and to promote early discharge. “Pyjama paralysis” should be discouraged. While a hospital gown prevents damage to patients’ clothes and facilitates access for RA and surgery, wearing their own clothes encourages self-care and adds familiarity.
PATIENT PREPARATION AND PREOPERATIVE ASSESSMENT
Patient preparation starts from the moment they are considered for surgery. Early information on RA techniques and what to expect during and after surgery promotes patient engagement and helps to reduce patient anxiety.
Patient selection is key for successful day case surgery. Advanced preoperative assessment of complex patients allows early planning for the likelihood and safety of day case surgery compared with an overnight admission. Important factors to consider include patient factors (such as comorbidities, body mass index, patient engagement), social factors (distance from local hospital, requirement for someone else to be with them for the first 24 hours postoperatively) and surgical/anaesthetic factors (duration and complexity of surgery/anaesthetic). Specific to day case hand and wrist surgery, engagement with detailed physiotherapy regimes and need for ongoing local anaesthetic infusion following complex surgery may limit same-day discharge. Complex hand and wrist surgery may be outside the remit of some smaller hospitals, and so distance from the patient’s home to the operating hospital should also be considered when planning discharge.
On the day of surgery, staggered arrival and tailored starvation times help limit dehydration and hunger and allow for a lower volume of patients in the department at any one time. Patient flow is facilitated because less room is required for fewer patients and staff are not as rushed preparing all patients for theatre at the same time. Patient admission to an area close to the operating theatre, more than 1 anaesthetist or an anaesthetic preoperative assessment clinic can overcome the potential problems associated with staggered arrival times, allowing all patients to be assessed and consented fully.
Patient comfort is paramount. Patients should be encouraged to visit the toilet immediately before arriving in theatre, and patients should be able to position themselves on the operating table prior to preparation for surgery. A comfortable temperature should be maintained in the operating theatre.
ANAESTHETIC TECHNIQUE
Supraclavicular, infraclavicular and axillary brachial plexus techniques are frequently used for hand and wrist surgery. Routine use of ultrasound guidance provides improved success rates, faster onset, longer block duration and shorter block performance time while also reducing the risk of vascular puncture.8
This tutorial will not discuss performance of brachial plexus or peripheral nervous blockade in depth, but some important factors are raised below. Readers wishing to review how to perform brachial plexus and peripheral nerve regional anaesthetic techniques are directed toward the Anaesthesia Tutorial of the Week library, which contains several tutorials detailing relevant anatomy and approaches to upper limb RA techniques.
Tailoring Anaesthetic Technique
There are several factors that influence the choice of local anaesthetic agent and technique for hand and upper limb surgery:
Duration of Surgery
Complex surgery of the upper limb can take several hours. It is important to consider patient comfort, including the use of sedation or general anaesthesia and maintenance of body temperature, but also balancing speed of onset and duration of RA. Local anaesthetic agents commonly used in our unit for different operative durations are listed in Table 1. It is worth noting that analgesic duration can vary between patients.
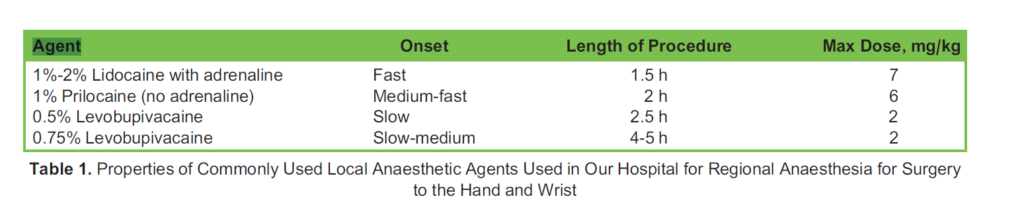
Mixing of local anaesthetics may provide the best properties of both, but this also dilutes the concentration of local anaesthetic (and additives if used), affecting the speed of onset and duration. Additives such as dexamethasone or dexmedetomidine to local anaesthetic solutions may prolong the duration of action.9 Use of short-acting agents in a brachial plexus block with longer-acting peripheral nerve blocks promotes earlier return of motor functions with prolonged postoperative analgesia.
Patient Comorbidities
Patient comorbidities may influence the anaesthetic technique used; injuries, limited range of movement or overlying skin infection may preclude certain techniques. More proximal brachial plexus blocks carry a higher risk of ipsilateral phrenic nerve palsy, which may cause significant respiratory compromise in patients with decreased pulmonary reserve such as severe chronic obstructive pulmonary disease (COPD), obesity or preexisting contralateral phrenic nerve palsy or diaphragmatic injury.
Severe vascular or cardiovascular disease requires caution with the use of adrenaline supplementation of local anaesthetic. Although not evidence based, it seems reasonable to suggest that a degree of vasoconstriction may contribute to ischaemia of susceptible nerves.
Tourniquet Use
Tourniquets are used to limit intraoperative bleeding and facilitate a clear surgical field. They are typically inflated to 100 mmHg above arterial pressure and so produce ischaemia distal to the site of application. Ischaemic pain is not eliminated by regional anaesthetic techniques. After a variable amount of time, patients may complain of pain in the anaesthetised limb or tightness from the tourniquet. Tourniquet time should be limited to 2 hours to limit nerve injury through direct compression. If longer tourniquet times are required, a period of reperfusion should be allowed before reapplication.
Brachial plexus RA techniques allow for longer tourniquet inflation times compared with distal nerve block techniques; how- ever, the motor block associated with plexus blockade can decrease patient satisfaction and cause shoulder discomfort.
Should an arm tourniquet be used, blockade of the medial cutaneous nerve of the arm and the intercostobrachial nerve is required. They derive from T1 and T1,2, respectively, and so may not be covered by brachial plexus blockade, although supra- clavicular plexus block may cover these nerves through proximal spread of local anaesthetic toward the T1 and T2 nerve roots. Techniques for anaesthetising these nerves include subcutaneous injection around the medial arm above the level of the tourniquet or injection superficial to the deep fascia of the arm in the axilla.10 A tourniquet block may aid tolerance of tourniquet pain for short procedures when brachial plexus blockade is not performed.11
If a peripheral tourniquet (eg, wrist or finger) is used and the surgical procedure is short, then peripheral nerve or ring/web- space blocks provide good effect and no motor block. Use of a narrow-gauge needle and slow injection aids tolerance of these sometimes painful injections.
Bone or Soft-Tissue Surgery
Soft-tissue surgery is usually less painful than surgery involving bone and periosteum, and so longer-acting analgesic blocks may not produce significant benefit over simple infiltration of local anaesthetic. If significant bony manipulation is planned (eg, wrist fusion with carpectomy or radial shortening procedures), then continuous local anaesthetic infusion via a catheter may be used as an adjuvant to systemic postoperative analgesia, although this may necessitate inpatient admission.
Patient Anxiety
Anxiety around the time of surgery is common. In many countries where general anaesthesia is considered the norm, the thought of being awake can cause significant anxiety. If a patient displays significant anxiety and they are likely to move during insertion of the block, axillary or infraclavicular plexus blocks are considered lower-risk approaches to the brachial plexus. Significant patient anxiety can make positioning of the anaesthetised limb difficult, prolonging surgery.
The location of the skin incision and/or tourniquet should be considered when planning nerve block for surgery more proximal than the wrist. Outside of hand and wrist surgery, high-arm tourniquets may be used for cubital tunnel release. For these cases, supraclavicular or infraclavicular techniques may be preferred to ensure blockade of the axillary nerve, which innervates the ‘regimental badge’ patch of skin on the upper arm; this is not covered by an axillary brachial plexus block.
Which Brachial Plexus Blocks Should I Choose?
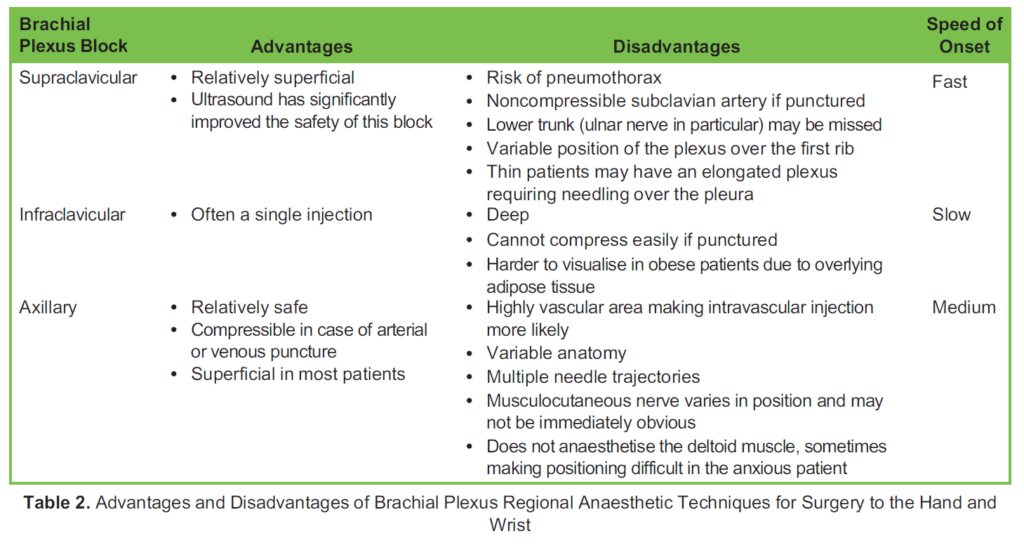
Superiority of axillary, infraclavicular or supraclavicular brachial plexus block for surgery below the shoulder has not been demonstrated.12 Many anaesthetists consider one brachial plexus block to be superior over another in their hands; however, for those learning, each has their advantages and disadvantages, as listed in Table 2.
The key with each technique is to spend time identifying each part of the plexus before starting and again toward the end to ensure good spread of local anaesthetic. Supplementation of individual nerves in the axilla (if not already used as the initial site of injection) or peripherally will allow coverage of any missed nerves. Testing prior to movement into the theatre allows for early detection of a failed or partial block. Often, simply asking the patient to try to scratch their nose with the anaesthetised limb is a good indicator of onset and reassures the patient. Direct testing of sensory and/or motor aspects of each nerve is encouraged.
Choice of peripheral nerve blocks is dependent on the location of the skin incision, but surgery to bones in particular may also require blockade of the nerves on the other side of the hand.
Anaesthesia for awake hand surgery is a skill and requires engagement from the patient, anaesthetist, surgeon and theatre/ perioperative teams. Anaesthesia Tutorial of the Week 44113 addresses block failure and troubleshooting in awake hand surgery, so this will not be covered in depth here; however, risk factors for failure include the following:
- Patient factors: language barriers, comorbidities (affecting both block performance but also sensitivity to local anaesthesia), anxiety
- Operator experience
- Inappropriate block/choice of local anaesthetic
- Tourniquet use
- Anatomical variation
Positioning
Most hand and forearm surgery occurs with the patient supine with the arm abducted to 608 to 908 and the hand in supination; however, some procedures may require alternative positioning, which can make communication with the patient and monitoring of sedation difficult. In positions in which the patient is not fully visible to the anaesthetist, minimal sedation is preferable. Capnography via a face mask or nasal oxygen delivery device may be a useful adjunct when access is limited.
Sedation
Short-acting anxiolysis such as low-dose midazolam is often beneficial before performing brachial plexus regional anaesthetic techniques; it can aid positioning and tolerance of the block, also providing some sedative effect intraoperatively. With appropriate monitoring, target-controlled infusions such as with propofol can also be used to avoid a general anaesthetic.
Distraction Techniques
Distraction techniques play a role in helping some patients tolerate surgery under RA. This may be through an additional member of staff in the operating theatre to hold their hand or talk to them, listening to their own music or watching a film on a portable device. Although still in its infancy, small studies have demonstrated that the use of virtual reality headsets provides improved patient satisfaction and decreased patient anxiety when used as distraction therapy in medical settings.14
WIDE-AWAKE LOCAL ANAESTHESIA NO TOURNIQUET (WALANT)
The 3 principles of WALANT are to control pain with local anaesthetic, control bleeding with adrenaline and control anxiety with surgical technique, communication and environment. Reported benefits of this technique include elimination of risks from using sedation, tourniquet and RA; it allows the surgeon to discuss the findings with the patient in real time; and it allows the patient to perform specific movements to assess function intraoperatively.
Traditionally, this technique has been used for very limited interventions, but there is evidence of its use for metacarpal sur- gery, carpal tunnel release, trigger finger, Dupuytren’s contracture and even plating of distal radial fracture.15
STAFFING
A well-prepared team that regularly manages awake patients is likely to achieve better outcomes. An experienced team is able to reassure patients, manage anxieties and avoid conversion to general anaesthesia. An anaesthetist experienced in RA and ‘awake surgery’ and an additional staff member in the operating theatre to be next to the patient throughout are preferable.
An efficient operating list utilising RA often involves managing 2 patients simultaneously. This promotes quicker turnover between cases and allows adequate time for the block to develop.
One option to achieve this is the use of a block room where one anaesthetist can perform the nerve blocks for several theatres and allow enough time for it to be fully effective before transfer to theatre. However, this requires the presence of an additional anaesthetist, and many suites of operating theatres do not have space amenable to being converted into such a facility. An alternative is to utilise the anaesthetic room whilst another patient is in theatre. This allows the anaesthetist to be closer to both patients, with another trained member of staff directly monitoring the patient in the operating theatre, providing that no sedation has been given.16 This requires the team in theatre to be aware of the needs of 2 patients simultaneously and timing of patient arrival so that there is no hammering or other loud noises in the theatre that may cause unnecessary distress.
POSTOPERATIVE CARE
Discharge within a few hours of surgery should be the aim, with advice and written information on rebound pain, arm elevation, care of the anaesthetised limb and 24-hour contact number for advice or in the event of any complications. Rebound pain following RA is common; patient counselling should include specific advice to take simple analgesics whilst the nerve block is still working and stronger analgesics for breakthrough pain.
OTHER FACTORS
Regular teaching and training in plexus anaesthesia and continuous audit of services provided contribute to continuous development of the service and further strengthen patient care. Ongoing training in new techniques and equipment should be provided.
SUMMARY
Day case hand and wrist surgery is an important area of development in the push for greater numbers of day case procedures. Anaesthetic technique and education and training of staff play important roles, but the setup of services is equally important to facilitate an efficient and productive service.
REFERENCES
- Castoro C, Bertinato L, Baccaglini U, et al. World Health Organisation on Behalf of the European Observatory on Health Systems and Policies. Policy brief. Day surgery: making it happen. Accessed January 4, 2023.
- National Health Service, Getting it right the first National Day Surgery Delivery Pack. Accessed January 4, 2023. https:// www.gettingitrightfirsttime.co.uk/wp-content/uploads/2020/10/National-Day-Surgery-Delivery-Pack_Sept2020_final.pdf
- The Royal College of Guidelines for the provision of anaesthesia services. Chapter 6: guidelines for the pro- vision of anaesthesia services for day surgery 2021. Accessed January 4, 2023. https://rcoa.ac.uk/gpas/chapter- 6#introduction
- Chan VWS, Peng PWH, Kaszas Z, et A comparative study of general anesthesia, intravenous regional anesthesia, and axillary block for outpatient hand surgery: clinical outcome and cost analysis. Anesth Analg. 2001;93:1181-1184.
- Hadzic A, Arliss J, Kerimoglu B et A comparison of infraclavicular nerve block versus general anesthesia for hand and wrist day-case surgeries. Anesthesiology. 2004;101:127-132.
- D’Alessio JG, Rosenblum M, Shea KP, et A retrospective comparison of interscalene block and general anesthesia for ambulatory shoulder arthroscopy. Reg Anesth. 1995;20:62-68.
- Brown AR, Weiss R, Greenberg C, et Interscalene block for shoulder arthroscopy: comparison with general anesthesia. Arthroscopy. 1993;9:295-300.
- Abrahams MS, Aziz MF, Fu RF, et Ultrasound guidance compared with electrical neurostimulation for peripheral nerve block: a systematic review and meta-analysis of randomized controlled trials. Br J Anaesth. 2009;102(3):408-417.
- Desai N, Kirkham KR, Albrecht Local anaesthetic adjuncts for peripheral regional anaesthesia: a narrative review. Anaesthesia. 2021;76:100-109.
- Feigl G, Aichner E, Mattersberger C, et al. Ultrasound-guided anterior approach to the axillary and intercostobrachial nerves in the axillary fossa: an anatomical investigation. Br J Anaesth. 2018;121:883-889.
- Sheikh ZI, Searle A, Townsley P, Radhakrishnan L. A novel block technique to improve tourniquet tolerance in day case distal hand surgery. Int J Periop Ultrasound Appl Technol. 2014;3:22-24.
- Stav A, Reytman L, Stav MY, et al. Comparison of the supraclavicular, infraclavicular and axillary approaches for ultra- sound-guided brachial plexus block for surgical anesthesia. Rambam Maimonides Med J. 2016;7:e0013.
- Pack E, Smith M. ATOTW 441. Regional anaesthesia for awake hand surgery: block failure and troubleshooting issues. Accessed January 4, 2023. https://resources.wfsahq.org/atotw/regional-anaesthesia-for-awake-hand-surgery-block-fail ure-and-troubleshooting-issues/
- Alaterre C, Duceau B, Sung Tsai E, et Virtual Reality for Peripheral Regional Anesthesia (VR-PERLA study). J Clin Med. 2020;9:215.
- Huang YC, Hsu CJ, Renn JH, et WALANT for distal radius fracture: open reduction with plating fixation via wide-awake local anesthesia with no tourniquet. J Orthop Res. 2018;13:195.
- Klein AA, Meek T, Allcock E, et Recommendations for standards of monitoring during anaesthesia during anaesthesia and recovery 2021. Guidelines from the Association of Anaesthetists. Anaesthesia. 2021;76:1212-1223.
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/