General Topics

KEY POINTS
- Optimising the patient’s position is essential.
- Approaches can be midline or paramedian. The latter approach is favoured for thoracic epidurals and in patients who are unable to flex their spines or those with significant spinal calcification or deformity.
- Air or saline with continuous or intermittent pressure is applied to the loss of resistance. Current evidence suggests no difference in the success, efficacy or complication rates between the different techniques.
- Dural puncture epidurals may safely improve detection of the epidural space.
- Some commonly encountered difficulties may be troubleshooted, whilst others require a new attempt.
INTRODUCTION
This tutorial covers the techniques to gain access to the epidural space. Previous tutorials discuss the general principles and rationale for epidural analgesia in paediatrics (Tutorial 334) and labour analgesia (Tutorial 365). The use of ultrasound for neu- raxial anaesthesia is covered in Tutorial 349. Complications of epidurals, including dural puncture with an epidural needle, are beyond the scope of this tutorial.
Epidurals can be inserted using the midline or paramedian approach. The epidural space is identified by loss of resistance (LOR). This phenomenon is the decrease in resistance felt whilst injecting saline or air as the needle passes from the ligamentum flavum to the potential epidural space. The operator detects the change from high resistance when trying to inject saline or air into the ligamentum flavum compared with the low resistance when injecting into the potential epidural space. In an Obstetric Anaesthetists’ Association (OAA) survey, the preferred technique is the loss of resistance to saline (LORS) with continuous pressure (58%) followed by the loss of resistance to air (LORA) with intermittent pressure (21%).1 Hand positioning requires adjustments based on the technique choice.
The dural puncture epidural (DPE) technique continues to be an affirming technique for labour epidural placement. The dura is intentionally punctured with a spinal needle to deduce a midline placement of an epidural catheter. The confirmation of the intrathecal space with the visualisation of cerebral spinal fluid (CSF) reduces the ambiguity of the indeterminate LOR that can occur due to individual anatomic differences. Studies of DPE show increased efficacy of labour epidural analgesia.
Whichever method is used, there are common pitfalls that may be encountered. Some of these can be safely troubleshooted, whilst others require removal of the epidural needle and further needling.
GENERAL PRINCIPLES
Procedure Outline
- Obtain consent, intravenous access and apply patient monitoring.
- Position the patient in the lateral decubitus or sitting position and identify landmarks.
- Prepare a sterile field, equipment and medication.
- Infiltrate the subcutaneous layer and along the projected needle trajectory with local anaesthetic.
- Insert a Tuohy epidural needle with stylet to 2 to 3 cm, until the needle is gripped by the surrounding connective tissue (the supraspinous ligament).
- Remove the stylet and attach a LOR syringe containing air or saline.
- Enter the epidural space on detection of LOR.
- Measure the depth at LOR.
- Remove the LOR syringe.
- In DPE, pass a spinal needle up to 3 mm beyond the epidural needle tip to obtain back flow of CSF. Then withdraw the spinal needle.
- Thread the epidural catheter to the depth of LOR plus an additional 4 to 5 cm.2
- Look for the falling meniscus sign (an air-fluid level within the catheter) if using a nonopaque catheter kit.
- Keeping sterile, secure the epidural catheter.
- Aspirate the catheter with a syringe to check for blood or CSF.
- Administer a test dose.
- Observe for signs of incorrect catheter placement (eg, rapid motor block [intrathecal] or neurologic or cardiovascular changes [intravenous]).
- Administer the main epidural infusion if no adverse signs are seen.
- Give ongoing maintenance doses and monitor.
Anatomical Landmarks
- For lumbar epidurals, the intercristal line is a horizontal line drawn across the highest points of both iliac crests and corre- sponds to the L4/5 space.
- For thoracic epidurals, the C7 prominence is most cranial, the spine of the scapula is at T3 and the inferior tip of the scapula is at T7.
Patient Positioning
- The sitting position is often favoured because the midline axis is more easily identified. It is important to avoid lumbar rotation as this may change the angle from the surface landmarks to the epidural space. The patient should be on a level surface with their shoulders and hips squarely aligned with one another. Feet should be balanced with the knees slightly above the hips to accentuate hip and lumbar flexion.
- The midline is usually identified by feeling for the spinous processes. The thoracic spinous processes may be more palpable, and running a finger along the spinous processes from this region may be easier.
- Ultrasound (Tutorial 349)3 is shown to help locate the spinous processes, depth of space and angulation of needle insertion required.4 Evidence also supports increased first-pass localisation and reduced time to successful placement.
- While the lateral position may be more comfortable, it is more difficult to ensure the spine is not rotated or flexed laterally.
Special Considerations for Parturients
- The lumbar lordosis is accentuated due to the centre of gravity being displaced forward by the gravid uterus.
- The intercristal line is often higher at L3/4 due to the forward rotation of the pelvis.5 A lower (L4/5) epidural provides better analgesia for perineal pain but may require more boluses early in labour.6 However, there is an association with higher rates of instrumental delivery when lower epidurals are sited.7
- Advancement of the needle may be challenging to time with the patient’s contraction pattern.
- Occasionally, the parturient may not be able to maintain the position long enough for an epidural to be inserted safely. A low- dose spinal, which is technically easier and has lower associated risks, may be used to provide some analgesia to allow better positioning for epidural placement. The approach can be midline or paramedian.
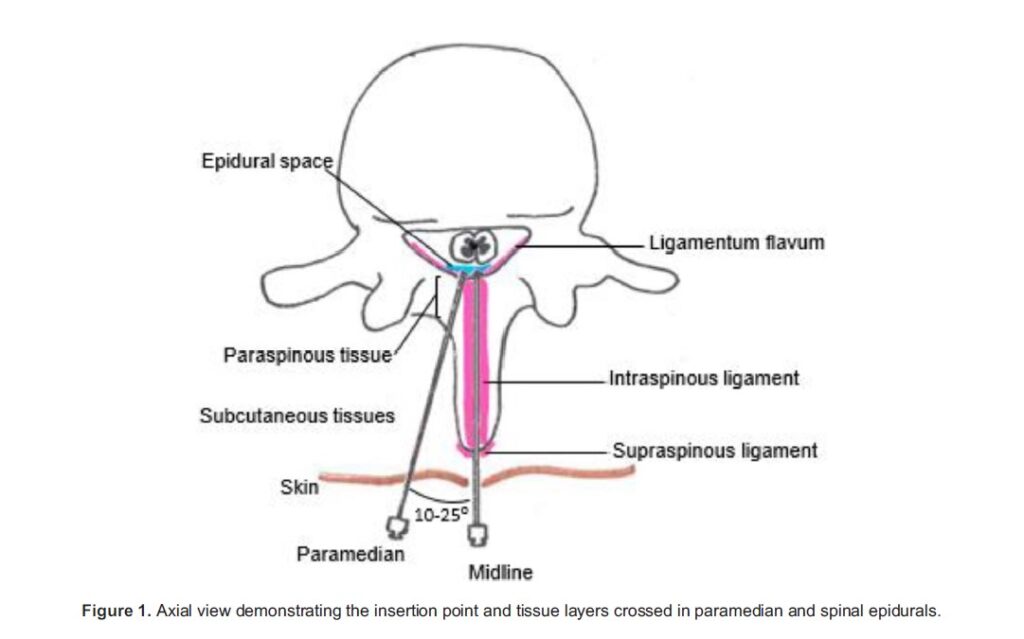
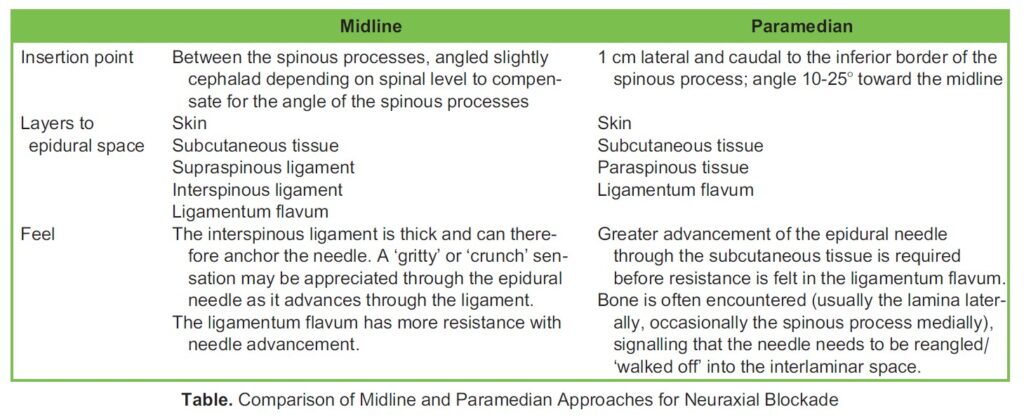
MIDLINE VERSUS PARAMEDIAN APPROACH
The midline approach is often favoured for initial epidural insertion. When the insertion point and needle tip point are midline and within the interspinous space, the only variable that can be altered is the degree of cephalad and caudal angulation.
The paramedian approach has more considerations. Lateral to medial angulation and lateral distance of needle insertion to midline require a better grasp of the spinal anatomy (Figure 1). In addition, the paramedian route can appear much deeper due to the indirect approach and may need a longer needle.
There are some circumstances in which the paramedian approach may be advantageous:
- In thoracic epidurals, the spinous processes are steeply angled
- In patients who are unable to flex the spine
- In those with significant spinal calcification or deformity (but any type of epidural may not be safe or practicable in those who have hardware from spinal fusion for scoliosis correction)
A comparison of the approaches is listed in Table 1.
LORA VERSUS LORS
It has been speculated that there is an increased failure rate with LORS, due to saline being misidentified as CSF. There is also a suggestion that that both high-volume injections and LORA are associated with headache, back pain, paraesthesia and unilateral block or missed segments.8
More conclusively, a meta-analysis in 2011 showed that LORA resulted in increased unblocked segments with no difference for catheter replacement or additional interventions.9 Presumably, the introduced air in the epidural space initially acts as an airlock, preventing the contact of local anaesthetics with the nerve roots in the missed segments. However, the air may be absorbed over time, meaning that the overall analgesic effect is adequate. More recently, a randomised, controlled study10 conducted in 2018 including 400 parturients showed no difference in pain scores or block efficacy at 30 minutes in LORA versus LORS.
Ultimately, there is insufficient evidence to say that either LORS or LORA is a superior technique for epidural insertion in terms of success, efficacy or complication. Instead, familiarity with the chosen technique is more important for navigating to the epidural space or troubleshooting placement.
CONTINUOUS OR INTERMITTENT PRESSURE ON THE LOR SYRINGE
With continuous pressure, saline is hypothesised to push the dura away from the epidural space. The technique relies on the constant application of pressure to the end of the plunger of the LOR syringe as the needle is being advanced toward the epidural space. When entering the low-pressure epidural space, all forward advancement of the plunger into the syringe occurs in the desired epidural space without forward advancement of the needle.
No studies have directly compared the application of continuous versus intermittent pressure techniques. Some argue that the continuous technique is safer because the nonadvancing hand can brace the wings of the epidural needle away against the patient’s back, preventing the needle from being advanced too rapidly.11 The intermittent technique may result in less control of the needle because the hand position changes frequently. It also heavily relies on the operator’s memory of resistance between advancements. However, proponents of the intermittent technique believe that they can detect more subtle changes in LOR and make finer adjustments with 2 hands holding the wings of the epidural needle.
As shown by an OAA survey,1 certain combinations are favoured: LORS with continuous pressure and LORA with intermittent pressure. In a small survey of trainees,12 there was no difference in the dural puncture rate between these 2 techniques.
HAND POSITION
When using continuous pressure with saline, there are many variations in hand position (Figure 2a-h). The goal is to optimise the ability to detect LOR as soon as the needle enters the epidural space. For intermittent pressure, both hands can advance the needle (Figure 2i). One hand checks the change in resistance in one of the ways described above, whilst the other main- tains the needle position.
DURAL PUNCTURE EPIDURAL
The DPE technique is one beneficial approach to the lumbar epidural because it is below the termination of the spinal cord at the conus medullaris (usually at L1 in adults). It is almost identical to the combined spinal and epidural, except that no drugs are directly administered to the intrathecal space. When preparing for a DPE, the spinal needle must be longer than an epidural needle and be able to fit inside it. Once LOR is detected, a spinal needle is passed through the epidural needle. If CSF flows back when the spinal needle tip is sufficiently beyond the tip of the epidural needle, the epidural space is confirmed. The spinal needle can then be removed, and the epidural catheter may be threaded.
DPEs are useful in patients in whom landmarks are difficult to identify or with indeterminate LOR (when the plunger of the LOR syringe can be gradually depressed, causing slow injection of air or saline). Subjectively, the pressure change may be subtle, compared with the usual loss of resistant felt. This may be due to the laxity of tissues or in people in whom the ligamentum flavum does not meet in the midline (0%-22% of people depending on the lumbar level).13 Conventionally, the operator relies on the experience of feeling the changing resistance and estimating the depth to the epidural space. With the DPE technique, if CSF is not detected in the spinal needle, the depth of the epidural space may not yet be reached or the needle is off midline.
TROUBLESHOOTING EPIDURAL INSERTION
Difficulty Locating the Epidural Space
As epidural insertion is a blind technique, bony obstructions may be felt when the trajectory of the needle fails to access the epidural space. In patients who are less able to flex the spine, a steeper approach may be needed. In other patients, this may be due to osteophytes. In a minority of patients, it may not be possible to locate the epidural space at all. The patient’s position should be optimised. The needle angle and insertion point may need to be redirected cranially or caudally in slight increments until the needle can pass between the spinous processes. Alternatively, readjusting to the space above or below the previously attempted space may be beneficial.
Cautious advancement into the epidural space is important to prevent temporary or permanent neuroinjury in the patient. Paraesthesia suggests close proximity of the epidural needle to the nerve roots. Recurrent paraesthesia should signal redirection or withdrawal of the epidural needle. The location and nature of the paraesthesia should be documented for reference.
Difficulty in Gaining or Confirming Access With the Epidural Catheter
The catheter may thread into an epidural vein. If frank blood is drawn back on aspiration from the epidural catheter, several steps may help reposition the catheter out of the vessel:
- Flush 1 to 2 mL of saline through the catheter prior to aspirating again.
- If unsuccessful, withdraw the catheter in 25-cm to 0.5-cm increments and repeat the flush and aspiration, or withdraw the catheter whilst simultaneously flushing saline.
- Once blood is no longer aspirated, the catheter may be secured and a test dose given to see if it is in the epidural space. However, be aware that small amounts of local anaesthetic may still enter the bloodstream.
- If a multiorifice catheter is used, it should not be withdrawn to less than LOR depth þ3 cm, to ensure the orifices are within the epidural space.
There has been a trend away from using a high-dose local anaesthetic (eg, 3-4 mL 2% lidocaine) to detect possible intravenous catheters due to the risk of local anaesthetic systemic toxicity.14 The lack of neurologic/cardiac symptoms with the development of an appropriate dermatomal block in the appropriate time frame (10-15 minutes) is highly suggestive of a catheter in the epidural space. However, negative aspiration does not out rule intravascular or intrathecal catheter placement.
The meniscus sign is a fluid level within the epidural catheter that rapidly falls when the catheter is raised above the lower-pressure epidural space and return of fluid (not continuous) when the catheter is lowered below the insertion site. It may not be detected in all patients (sensitivity 25%) but is highly specific for correct placement in the epidural space.15 If there is negative aspiration, and it is possible to flush 1 to 2 mL of saline, a test dose can still be given and the subsequent block tested for. Note that a meniscal drop may still be present with an epidural vein catheter depending on the pressure gradient between the height of the catheter and the pressure in the epidural vein.
The catheter may not thread due to the epidural needle only partially entering the epidural space or being half occluded by the ligamentum flavum. This may be addressed by rotating the needle and catheter by 908 or by trying to advance a thinner catheter. In some circumstances, it is possible to advance the needle by 0.5 mm to see if the epidural space can be entered. How- ever, if there is any doubt, it is advisable to remove the epidural needle and the catheter together to prevent the catheter from shearing off in the bevel of the needle. Hydrodissection through the catheter may be attempted, but it may then be difficult to test whether the catheter is in the epidural space. Usually, another attempt should be made to determine LOR and the epidural space.
SUMMARY
Whether it is LORA or LORS, continuous or intermittent pressure, there is no evidence regarding which combination of techniques is superior. Commonly, the technique comes down to what is taught and operator experience. DPEs are being proposed as an additional layer to provide more effective and safer epidural placement.
REFERENCES
- Wantman A, Hancox N, Howell Techniques for identifying the epidural space: a survey of practice amongst anaesthe- tists in the UK. Anaesthesia. 2006;61(4):370-375. doi:10.1111/j.1365-2044.2006.04534.x
- Beilin Y, Bernstein HH, Zucker-Pinchoff B. The optimal distance that a multiorifice epidural catheter should be threaded into the epidural space. Anesth Analg. 1995;81(2):301-304. doi:1097/00000539-199508000-00016
- McDonald A, Murgatroyd H. Ultrasound guided neuraxial anaesthesia [Internet]. ATOTW. 2008 Available at: https:// resources.wfsahq.org/atotw/ultrasound-guided-neuraxial-anaesthesia/ (Accessed: 25 August 2023).
- Tao B, Liu K, Ding M, Xue H, Li X, Zhao Ultrasound increases the success rate of spinal needle placement through the epidural needle during combined spinal-epidural anaesthesia. Eur J Anaesthesiol. 2021;38(3):251-258. doi:10.1097/EJA. 0000000000001380
- Baysinger C, Bucklin B, Gambling D. A Practical Approach to Obstetric Anesthesia. Philadelphia, PA: Lippincott Williams and Wilkins; 2009.
- Moore A, Villeneuve V, Bravim B, et al. The labor analgesia requirements in nulliparous women randomized to epidural catheter placement in a high or low intervertebral space. Anesth Analg. 2017;125(6):1969-1974.
- Antonakou A, Papoutsis D. The effect of epidural analgesia on the delivery outcome of induced labour: a retrospective case series. Obstet Gynecol Int. 2016;2016:5740534. doi:1155/2016/5740534
- Norman Epidural analgesia using loss of resistance with air versus saline: Does it make a difference? Should we reeval- uate our practice? AANA J. 2003;71(6):449-453.
- Murphy JD, Ouanes JPP, Togioka BM, et al. Comparison of air and liquid for use in loss-of-resistance technique during labor epidurals: a meta-analysis. J Anesth Clin Res. 2011;2:175. doi:4172/2155-6148.1000175
- Brogly N, Guasch E, Alsina E, et al. Epidural space identification with loss of resistance technique for epidural analgesia during labor. Anesth Analg. 2018;126(2):532-536. doi:1213/ANE.0000000000002593
- Scrutton MJL, Kinsella SM. Continuous or intermittent loss of resistance for identifying the epidural space. Anaesthesia. 2000;55(5):489-518. doi:1046/j.1365-2044.2000.01425-13.x
- MacMahon MJ, Baird CRW. Survey of accidental dural puncture rates by anaesthetic trainees using constant or intermit- tent plunger pressure. Int J Obstet Anesth. 2013;22(1):80-81. doi:1016/j.ijoa.2012.09.004
- Lirk P, Moriggl B, Colvin J, et The incidence of lumbar ligamentum flavum midline gaps. Anesth Analg. 2004:1178-1180. doi:10.1213/01.ANE.0000101486.41355.35
- Gardner IC, Kinsella SM. Obstetric epidural test doses: a survey of UK practice. Int J Obstet Anesth. 2005;14(2):96-103. doi:1016/j.ijoa.2004.07.013
- Servin MN, Mhyre JM, Greenfield ML, Polley An observational cohort study of the meniscus test to detect intravascular epidural catheters in pregnant women. Int J Obstet Anesth. 2009;18(3):215-20. doi:10.1016/j.ijoa.2008.11.008
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/